Article Text

Abstract
Objective Anti-neutrophil cytoplasmic antibodies and anti-Saccharomyces cerevisiae mannan antibodies (ASCAs) have been detected in the serum of patients with ulcerative colitis (UC) and Crohn's disease (CD) and their unaffected family members. The aim of this study was to establish the value of serological markers as predictors of UC and CD.
Design Individuals who developed CD or UC were identified from the European Prospective Investigation into Cancer and Nutrition (EPIC) study. At recruitment, none of the participants had a diagnosis of CD or UC. For each incident case, two controls were randomly selected matched for centre, date of birth, sex, date of recruitment and time of follow-up. Serum of cases and controls obtained at recruitment were analysed for ASCA IgG, ASCA IgA, perinuclear anti-neutrophil cytoplasmic antibody (pANCA), antibodies against Escherichia coli outer membrane porin C (OmpC) and flagellin CBir1. Conditional logistic regression was used to determine risk of CD and UC. Receiver operating characteristic curves were constructed to test accuracy.
Results A total of 77 individuals were diagnosed with CD and 167 with UC after a mean follow-up of 4.5 (SD 3.2) and 4.4 (SD 3.1) years following blood collection, respectively. Combinations of pANCA, ASCA, anti-CBir1 and anti-OmpC were most accurate in predicting incident CD and UC (area under curve 0.679 and 0.657, respectively). The predictive value of the combination of markers increased when time to diagnosis of CD or UC decreased.
Conclusion A panel of serological markers is able to predict development of CD and UC in individuals from a low-risk population.
- Crohn's disease
- ulcerative colitis
- serology
- predictive accuracy
- inflammatory bowel disease
- Crohn's colitis
- dysplasia
- colonic neoplasms
- IBD clinical
- gallstones
- diverticular disease
- IBD
- quality of life
- Barrett's metaplasia
- Barrett's carcinoma
- Barrett's oesophagus
- oesophageal cancer
- nonalcoholic steatohepatitis
- nerve
- gut interactions
- autoimmune liver disease
- liver
- primary biliary cirrhosis
- epidemiology
- nutrition
- cancer epidemiology
Statistics from Altmetric.com
- Crohn's disease
- ulcerative colitis
- serology
- predictive accuracy
- inflammatory bowel disease
- Crohn's colitis
- dysplasia
- colonic neoplasms
- IBD clinical
- gallstones
- diverticular disease
- IBD
- quality of life
- Barrett's metaplasia
- Barrett's carcinoma
- Barrett's oesophagus
- oesophageal cancer
- nonalcoholic steatohepatitis
- nerve
- gut interactions
- autoimmune liver disease
- liver
- primary biliary cirrhosis
- epidemiology
- nutrition
- cancer epidemiology
Significance of this study
What is already known on this subject?
-
Anti-neutrophil cytoplasmic antibodies and several antimicrobial antibodies, including anti-Saccharomyces cerevisiae mannan antibodies (ASCAs), antibodies against Escherichia coli outer membrane porin C (OmpC) and against the flagellin CBir1, have been detected in serum of patients with Crohn's disease (CD) and ulcerative colitis (UC)
-
A previous study with small patient numbers reported that perinuclear anti-neutrophil cytoplasmic antibody (pANCA) and ASCA were able to predict development of UC and CD years before these diseases were clinically diagnosed
What are the new findings?
-
A combination of pANCA, ASCA, anti-CBir1 and anti-OmpC is able to predict the development of CD and UC in individuals from a low-risk population
-
The predictive value of this combination of markers increases when time to diagnosis of CD or UC is shorter
How might it impact on clinical practice in the foreseeable future?
-
The identification of individuals at risk of inflammatory bowel disease using the combination of serological markers as described in the present study opens new avenues for pathogenetic studies in a ‘prediagnostic inflammatory bowel disease phase’ and thereby introduces a window of opportunity for early intervention.
Introduction
Although the mechanisms underlying the development of inflammatory bowel disease (IBD) are still incompletely understood, it is biologically plausible that the aetiology of IBD involves an inappropriate response of the mucosal immune system to the commensal intestinal flora in genetically susceptible individuals. This abnormal response may be facilitated by failure of the intestinal epithelial barrier function and/or defects in the mucosal immune system.1 These mechanisms probably facilitate the generation of anti-Saccharomyces cerevisiae mannan antibodies (ASCA)—antibodies against mannose epitopes from the yeast Saccharomyces cerevisiae—and perinuclear anti-neutrophil cytoplasmic antibodies (pANCA)—antibodies against proteins in the nuclear lamina of neutrophils. The combination of these antibodies has been shown to differentiate Crohn's disease (CD) from ulcerative colitis (UC) with a sensitivity of 52–64% and specificity of 92–94%2 ,3 and may be used in patients in whom the distinction between CD and UC cannot be made on clinical, histological and/or endoscopical grounds. More recently, other serological markers have been identified, including antibodies against the outer membrane porin C (OmpC) of Escherichia coli, antibodies against subtypes of flagellins (CBir1) and various anti-glycan antibodies. Both pANCA/ASCA and the more recent identified antibodies were found to be associated with specific clinical and phenotypical characteristics in CD and UC patients. For example, both ASCA and anti-OmpC have been linked to ileal disease, complicated disease behaviour and early surgery in CD.4–7 Patients with UC that have a high level of pANCA are at an increased risk of pouchitis after ileal pouch-anal anastomosis.8 ,9
The appearance of serum antibodies might precede the onset of clinical symptoms in autoimmune diseases by several years. For instance, anti-cyclic citrullinated peptide (anti-CCP) antibodies and rheumatoid factor (RF) have been reported to predate clinical rheumatoid arthritis by up to 22 years10 ,11 and the presence of these antibodies is associated with a significantly increased risk of development of rheumatoid arthritis in these individuals (OR 16.1, 95% CI 3.3 to 76.7 and OR 5.1, 95% CI 1.6 to 16.0 for anti-CCP and RF-IgA, respectively).10 Whether serological markers predict the future development of IBD in asymptomatic individuals is presently largely unknown. Only one small study reported the presence of ASCA (IgG/IgA) and pANCA in 32 individuals with incident CD and 8 individuals with incident UC respectively, before the clinical diagnosis was made.12 We aimed to investigate whether serological markers predict the development of either CD or UC in a large European cohort of individuals.
Patients and methods
Study population
Participants were enrolled in the European Prospective Investigation into Cancer and Nutrition (EPIC) study, which recruited ∼520 000 volunteers from 23 centres in 10 European countries between 1992 and 2000. The study design has been reported extensively elsewhere.13 For the present study, data and serum were available from participants in 6 European countries, constituting a sub-cohort of 354 398 participants. Subjects were recruited from centres in Sweden, Denmark, The UK, France, Germany and The Netherlands.
Case and control identification
At recruitment, none of the participants had a diagnosis of CD or UC. Individuals who subsequently were diagnosed with CD or UC during follow-up until July 2010 (incident CD and UC cases) were identified by different measures in order to acquire the most complete coverage, including EPIC follow-up questionnaires, population-based disease registries, hospital-based registries, pathology records and health insurance schemes. For each case, local physicians confirmed the diagnosis of CD or UC on the basis of endoscopy, histopathology, surgery and/or radiology reports and reported the date of diagnosis and extent of disease.
For each incident case of IBD, two controls were randomly selected from the same EPIC centre, matched for date of birth (±6 months), sex and date of recruitment into EPIC (±3 months). Controls were alive at the date that the matched case was diagnosed (incidence density matching), which ensured that the time of follow-up was similar for all subjects.
Antibody testing
Serum samples donated by participants at recruitment were stored in liquid nitrogen containers and shipped on dry ice to Prometheus Laboratories (San Diego, California, USA) where they were analysed for ASCA IgG, ASCA IgA, pANCA, anti-OmpC and anti-CBir1.14–17
The laboratory technicians were blinded to the case/control status of participants.
Statistical analysis
For incident cases, we defined time to event by calculating the difference between sampling date and date of diagnosis. To test the accuracy for each of the serological markers studied, receiver operating characteristic (ROC) curves were constructed by plotting sensitivity versus 1-specificity, using the titres of the individual markers. Furthermore, to study whether a combination of markers improved their predictive accuracy, a new ROC curve was compiled which included the relative contribution of each marker based on its concentration, as assessed by conditional logistic regression analysis with backward selection of all five markers. This resulted in two serological scores; one for CD versus controls and one for UC versus controls. In order to assess risk of CD or UC in different time frames before the diagnosis using the serological scores of the two cohorts, each cohort was divided into three equally-sized groups based on time to diagnosis. Risk of CD or UC was then calculated by conditional logistic regression for each time frame and adjusted for cigarette smoking at recruitment. All statistical analyses were performed using SPSS V.15.0 for Windows. A p value <0.05 was considered statistically significant.
Ethical considerations
This study was carried out with the approval of the International Agency for Research and Cancer Institutional Review Board and that of local ethics committees in each centre. At recruitment, all participants gave written informed consent for future use of their data and material.
Results
Baseline characteristics
A total of 244 patients with incident IBD were identified, of whom 77 had CD (74% women) and 167 UC (53% women, table 1). Mean age was 57.2 years (SD 10.0) at CD diagnosis and 58.0 years (SD 10.5) at UC diagnosis. At recruitment, 29 incident CD cases (38%) and 54 incident UC cases (33%) were cigarette smokers as compared with respectively 50 (33%) and 104 (31%) of matched controls. Of CD cases, 26 (34%) had colonic disease, 23 (30%) ileal disease and in 21 (27%) disease that was located in both the ileum and colon. Thirty-two UC cases (19%) had a proctitis, 74 (44%) a left-sided colitis, while in 46 cases (28%) disease extended beyond the splenic flexure. Individuals were diagnosed with CD and UC after a mean follow-up period of 4.5 (SD 3.2) and 4.4 (SD 3.1) years after serum sampling, with a maximum of 14.2 and 15.5 years, respectively.
Demographics of cases and controls
Predictive accuracy of combination of markers
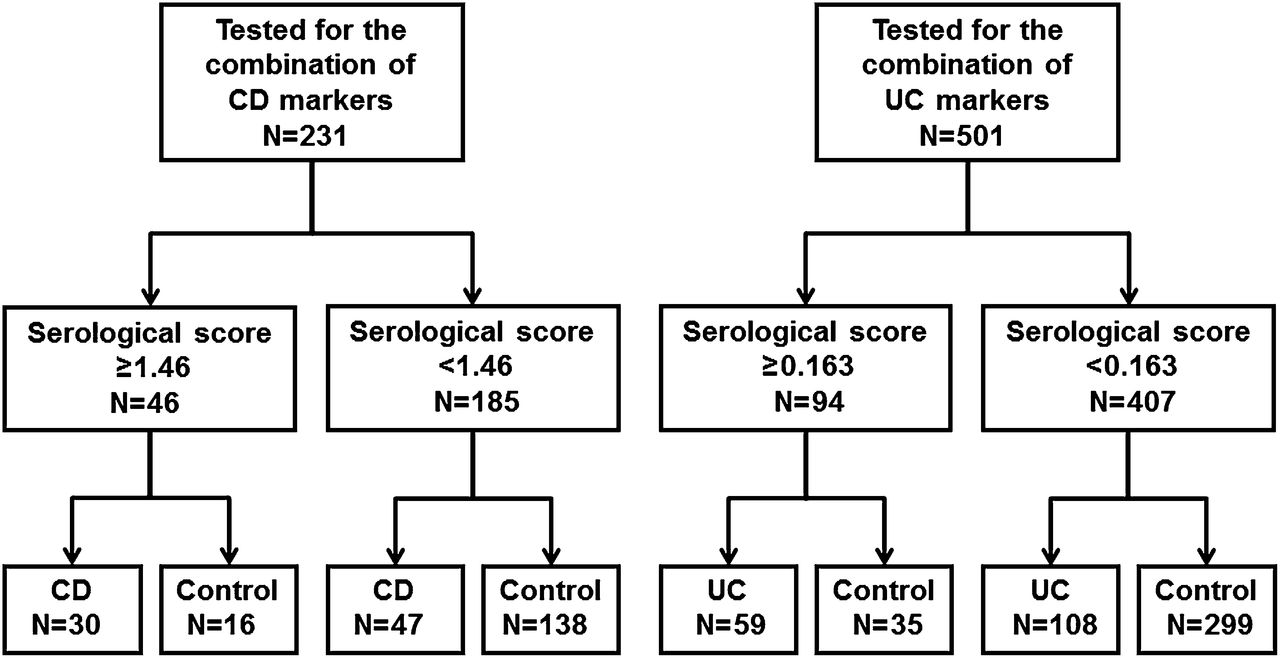
The ROC curves of both the individual markers and the combination of markers for differentiating between incident CD and controls are shown in figure 1A. The combination of pANCA, ASCA IgG, anti-CBir1 and anti-OmpC (the relative contribution being reflected by the regression coefficient of each individual marker) resulted in a higher predictive accuracy (area under the curve (AUC) 0.678) than that of each individual marker (AUC ranging from 0.534 to 0.651). A serological score of 1.46 as cut-off value for a CD diagnosis was associated with a specificity and positive predictive value (PPV) of 90% and 64%, respectively, and a sensitivity of 39%. The numbers of seropositive individuals according to this cut-off value are shown in figure 2. A higher serological score yielded a lower sensitivity and higher specificity. A score of 2.41 was associated with a specificity and PPV of 100%.

Receiver operating charcteristic (ROC) curves of individual markers and a combination of markers in Crohn's disease (A) and ulcerative colitis (B). ASCA, anti-Saccharomyces cerevisiae mannan antibodies; AUC, area under curve; pANCA, perinuclear anti-neutrophil cytoplasmic antibody.

Flowchart of test results in individuals with incident Crohn's disease (CD) and ulcerative colitis (UC) and controls.
The ROC curves of the individual and combination of markers for differentiating incident UC from controls are shown in figure 1B. Although pANCA was the strongest predictor, the addition of anti-CBir1, anti-OmpC and ASCA IgA increased the predictive accuracy compared with pANCA alone (AUC 0.657 vs 0.621). The addition of ASCA IgG did not increase the accuracy of the model (AUC 0.657). With a serological score of 0.163 as cut-off value for the UC diagnosis, sensitivity, specificity and PPV were 35%, 90% and 63%, respectively. The numbers of seropositive individuals according to this cut-off value are shown in figure 2. A serological score of 5.62 was associated with a specificity of 100% and a PPV of 100%.
Association between serological score and time to diagnosis
There was no specific pattern in the appearance of individual antibodies in relation to time to diagnosis in both incident CD and incident UC.
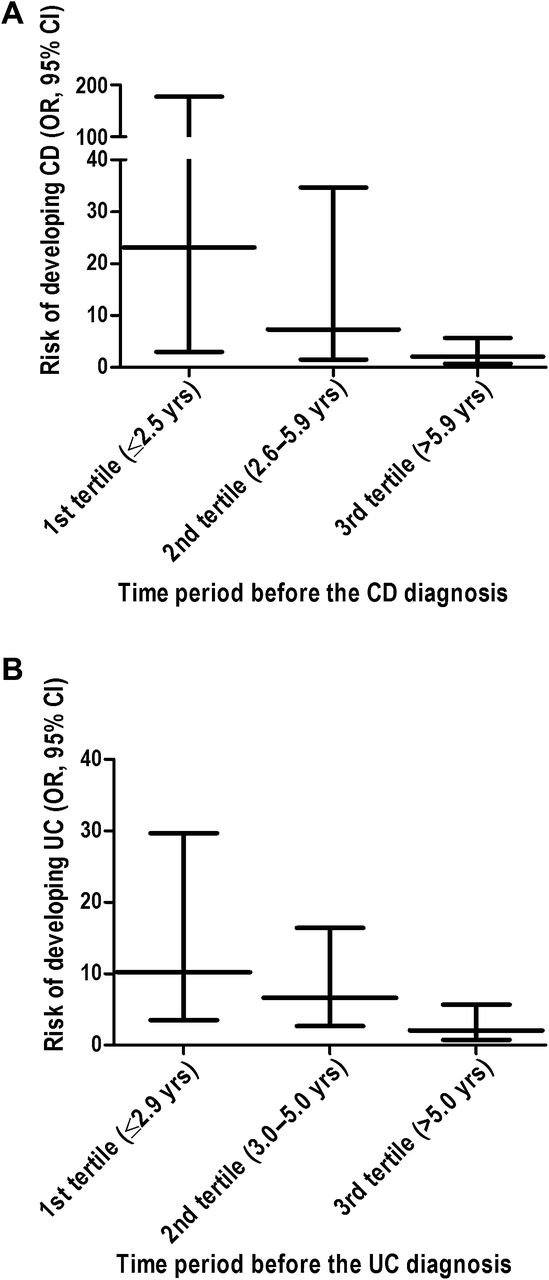
Figure 3A shows the risk of CD in three time frames according to the time to diagnosis, using 1.46 as cut-off value of the serological score for the CD diagnosis. The overall OR for developing CD according to this cut-off value was 5.18 (95% CI 2.51 to 10.7). The risk of developing CD was twenty-three times greater (OR 23.1, 95% CI 3.00 to 177) among participants with a positive serological score who were diagnosed with CD in the first 2.5 years of follow-up. This association was smaller among individuals who were diagnosed within 2.6–5.9 years (OR 7.30, 95% CI 1.53 to 34.7) and among participants diagnosed more than 5.9 years after baseline (OR 2.05, 95% CI 0.774 to 5.67).
{kind=link}
{kind=link}
{kind=link}
Risk of developing Crohn's disease (CD) or ulcerative colitis (UC) in three different time periods before the clinical and histopathological diagnosis using 1.46 as cut-off value in Crohn's disease (A) and 0.163 as cut-off value in ulcerative colitis (B). Crohn's disease: 1st tertile OR 23.1, 95% CI 3.00 to 177; 2nd tertile OR 7.30, 95% CI 1.53 to 34.7; 3rd tertile: OR 2.05, 95% CI 0.774 to 5.67. Ulcerative colitis: 1st tertile OR 10.2, 95% CI 3.51 to 29.7; 2nd tertile OR 6.61, 95% CI 2.67 to 16.4; 3rd tertile 2.05, 95% CI 0.774 to 5.67.
Figure 3B shows the risk of UC in three time frames before the UC diagnosis, using 0.163 as cut-off value of the serological score for the UC diagnosis. The overall OR for developing UC according to this cut-off value was 5.57 (95% CI 3.22 to 9.65). The risk of developing UC was 10 times greater (OR 10.2, 95% CI 3.51 to 29.7) among participants with a positive serological score who were diagnosed with UC in the first 2.9 years of follow-up. As for CD, this association was smaller among individuals who were diagnosed within 3.0–5.0 years (OR 6.61, 95% CI 2.67 to 16.4) and among participants diagnosed more than 5.0 years after baseline (OR 2.05, 95% CI 0.774 to 5.67).
Adjustment for smoking at recruitment into EPIC had no influence on ORs for each time period before the CD and UC diagnosis (data not shown).
Discussion
The present study assessed the value of serological markers as predictors of IBD. We were able to assemble a unique cohort of 77 individuals with incident CD and 167 individuals with incident UC in whom five serological markers were tested. We analysed the predictive accuracy using the titres of the individual markers and combined these into an equation. The predictive accuracy of a combination of markers was found to be higher than the accuracy of each marker alone, with high specificities and PPVs.
Interestingly, the risk of developing either CD or UC among individuals with a positive serological score for either CD or UC was found to be highly dependent on time to diagnosis of IBD. This finding, together with the high specificity and PPV suggests that these serological scores can be used as screening tests for CD and UC in apparent healthy individuals.
The only other study that assessed the presence of serological markers before a clinical diagnosis of IBD examined ASCA and pANCA in recruits of the Israeli military corps of whom 32 developed CD and 8 UC.12 The investigators reported ASCA positivity in 10 of 32 incident CD patients (31%) 3.2 years before the clinical diagnosis, and pANCA positivity in 2 of 8 subjects (25%) with incident UC. The panel of serological markers used in our study performed better: 30 of 77 (39%) CD patients and 58 of 167 (35%) UC patients tested positive years before the clinical diagnosis. In contrast to Israeli et al, we did not employ the cut-off values as proposed by the producers of the kit. These values were determined in patients with established IBD and could therefore not be used in the apparent healthy individuals in our cohort. The mean interval between serum sampling and time of diagnosis was longer in our study as compared with the Israeli study. The latter study reported an increase in ASCA levels and frequency of positivity in asymptomatic subjects when intervals between serum sampling and time of diagnosis decreased. A shorter mean interval between serum sampling and time of diagnosis might therefore have resulted in higher positivity rates for ASCA and the other antibodies in our study. This is highlighted by our observation that risk of CD or UC was higher among individuals with a positive serological score when the interval between recruitment in the study and diagnosis of IBD was shorter. However, based on individual antibody levels in three different time frames before the clinical diagnosis, we found no specific patterns in antibody levels.
Furthermore, in CD patients ASCAs have been associated with ileal and pANCAs with colonic disease.6 ,18 Therefore, the predictive values of these serological markers might be higher in these specific subgroups. However, the relative small number of patients with these phenotypes in our study precludes a meaningful analysis.
Another striking difference to the Israeli study relates to the higher mean age at diagnosis of our IBD cohort, which resulted from the inclusion of predominantly middle-aged and older individuals in the EPIC study. In CD, ASCA positivity is more frequently encountered in patients diagnosed at a young age,6 ,19 while pANCA positivity seems to be observed more frequently in CD patients diagnosed at an age of 40 years or older.18 ,20 In addition, our cohort included more women than men. Whether these patient characteristics had a major impact on our results is a matter of speculation.
In the present study, we did not have the date of onset of symptoms attributable to IBD at our disposal. Although cases were excluded if symptoms were noted before inclusion into the EPIC cohort, disease duration might have been longer than assessed in this study. However, since the mean interval between blood collection and time of diagnosis was 4.5 years in both cohorts, and the mean diagnostic delay of CD and UC is approximately 9 and 4 months,21 we do not think that this had a major impact on our results. Furthermore, no information was available on the presence of other diseases affecting antibody production, among others coeliac disease and Behcet's disease.22 ,23 These disorders can present with similar symptomatology and are associated with the presence of serological markers as well. However, we feel that we can safely assume that the risk of confounding by other diseases is low. The IBD diagnosis was confirmed by local gastroenterologists, thereby minimising the chance of misdiagnosis. The prevalence of Behçet's disease in Western Europe is too low to consider as a source of bias, but we cannot exclude co-existence of coeliac disease in our cohort. Since this would have occurred in both the IBD group and controls, the impact on our results is probably small, even though coeliac disease might be associated with a modest increased risk of developing IBD.
The reason for antibody generation in future IBD patients is still largely unclear. It has previously been postulated that ASCAs are detectable due to increased intestinal permeability in CD patients leading to an increased exposure to antigens. However, several studies could not link intestinal permeability to ASCA levels in CD patients.24–27 In more recent studies, mannan-binding lectin (MBL) has been associated with ASCA generation. MBL plays an important role in human innate immunity by binding to mannan epitopes on the surfaces of microorganisms.28 Lack of MBL was found to promote a systemic adaptive immune response in mice treated with Candida albicans and was associated with higher ASCA levels in both mice and patients with CD.29 ,30 Candida albicans has been shown to generate ASCAs due to the expression of similar cell wall mannan epitopes as the yeast Saccharomyces cerevisiae.31 ,32 Standaert-Vitse et al reported an increased colonisation by Candida albicans in CD patients and their healthy relatives. However, when Candida albicans colonisation was investigated in relation to ASCAs in CD patients and their healthy relatives, increased Candida albicans colonisation was found to correlate with ASCA levels in healthy relatives, but not in patients with established CD.33 It thus seems that ASCAs are generated as a result of a deficiency in MBL in the presence of specific intestinal microorganisms. However, the exact contribution of both immunological and microbiological factors still needs to be further unravelled.
ANCAs have been found in both patients with vasculitis and in patients with IBD. IBD patients show an atypical perinuclear staining by indirect immunofluorescence, that is DNAse sensitive. This pattern is different from the perinuclear, myeloperoxidase-reactive staining pattern found in patients with vasculitis.17 Although various antigens have been suggested to be detected by atypical pANCAs in patients with IBD, including a nuclear histone (H1) and high-mobility group (HMG) non-histone chromosomal proteins (HMG1 and HMG2),34 ,35 the main antigen for atypical perinuclear pANCA staining is still unknown. Newer serological markers include anti-CBir 1 and anti-OmpC. Flagellins are principal components of bacterial flagella that are recognised by Toll-like receptor 5.36 The flagellin CBir1 was identified as a dominant target antigen that elicits strong B-cell and CD4 T-cell reactions in mice with colitis. Moreover, CD4 T-cells specific for CBir1 were found to induce colitis when transferred to severe immune deficient mice. CBir 1 was found to induce IgG antibody responses in approximately 50% of CD patients.15 OmpC, a transport protein in the membrane of Escherichia coli, was first identified as bacterial antigen in pANCA-positive UC patients, and was then found to elicit antibody responses in up to 55% of CD patients.3 ,14 ,37 Although knowledge on all these antigens is rapidly emerging, the specific role in the pathogenesis of IBD remains to be further investigated.
A major finding of our study is an increase of the predictive value of our panel of serological markers when time to diagnosis of CD or UC becomes shorter. We assume that in a significant number of individuals subclinical disease, and consequently, aberrant mucosal immune responses to microbiota antigens, is already present at an early stage. It can be envisioned that these abnormalities are more distinct if time to diagnosis decreases, thereby explaining a better performance of our serological scores. The clinical consequences of these findings are presently unclear.
In conclusion, this study demonstrates the value of a combination of serological markers in predicting CD and UC years before these diseases are being clinically overt. The predictive value of this combination of markers increases when time to diagnosis of CD or UC is shorter. The identification of individuals at risk of CD or UC using a combination of the present serological markers opens new avenues for pathogenetic studies in the ‘prediagnostic IBD phase’ and thereby introduces a window of opportunity for early intervention.
Acknowledgments
The authors thank Prometheus Laboratories, San Diego, California, USA, for performing the serological analyses at no cost to the investigators of this study.
References
Footnotes
-
Funding The coordination of EPIC is financially supported by the European Commission (DG-SANCO) and the International Agency for Research on Cancer. The national cohorts are supported by the Dutch Ministry of Health, Welfare and Sports, Dutch Prevention Funds, LK Research Funds, Dutch ZON (Zorg Onderzoek Nederland), World Cancer Research Fund (WCRF), Statistics Netherlands (the Netherlands); Ligue contre le Cancer, Institut Gustave Roussy, Mutuelle Générale de l'Education Nationale, Institut National de la Santé et de la Recherche Médicale (INSERM; France); German Cancer Aid, Federal Ministry of Education and Research (Germany); Danish Cancer Society (Denmark); Cancer Research UK, Medical Research Council, Stroke Association, British Heart Foundation, Department of Health, Food Standards Agency, the Wellcome Trust (UK); Swedish Cancer Society, Swedish Scientific Council and Regional Government of Skåne (Sweden).
-
Competing interests None.
-
Patient consent This study was carried out with the approval of the International Agency for Research and Cancer Institutional Review Board and of all participating local ethics committees. At recruitment, all participants gave written informed consent for future use of their data and material. Due to the large number of participants included into the EPIC study and the large number of studies being performed with this cohort, control over the informed consents is managed by the local ethics committees. We are therefore unable to submit the individual written informed consents.
-
Ethics approval This study was carried out with the approval of the International Agency for Research and Cancer Institutional Review Board and that of local ethics committees in each center.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement There are no supplementary or underlying data related to this paper available for data sharing.
Linked Articles
- Commentary