Article Text

Abstract
Objective Antitumour necrosis factor (anti-TNF) drugs impair protective immunity following pneumococcal, influenza and viral hepatitis vaccination and increase the risk of serious respiratory infections. We sought to determine whether infliximab-treated patients with IBD have attenuated serological responses to SARS-CoV-2 infections.
Design Antibody responses in participants treated with infliximab were compared with a reference cohort treated with vedolizumab, a gut-selective anti-integrin α4β7 monoclonal antibody that is not associated with impaired vaccine responses or increased susceptibility to systemic infections. 6935 patients were recruited from 92 UK hospitals between 22 September and 23 December 2020.
Results Rates of symptomatic and proven SARS-CoV-2 infection were similar between groups. Seroprevalence was lower in infliximab-treated than vedolizumab-treated patients (3.4% (161/4685) vs 6.0% (134/2250), p<0.0001). Multivariable logistic regression analyses confirmed that infliximab (vs vedolizumab; OR 0.66 (95% CI 0.51 to 0.87), p=0.0027) and immunomodulator use (OR 0.70 (95% CI 0.53 to 0.92), p=0.012) were independently associated with lower seropositivity. In patients with confirmed SARS-CoV-2 infection, seroconversion was observed in fewer infliximab-treated than vedolizumab-treated patients (48% (39/81) vs 83% (30/36), p=0.00044) and the magnitude of anti-SARS-CoV-2 reactivity was lower (median 0.8 cut-off index (0.2–5.6) vs 37.0 (15.2–76.1), p<0.0001).
Conclusions Infliximab is associated with attenuated serological responses to SARS-CoV-2 that were further blunted by immunomodulators used as concomitant therapy. Impaired serological responses to SARS-CoV-2 infection might have important implications for global public health policy and individual anti-TNF-treated patients. Serological testing and virus surveillance should be considered to detect suboptimal vaccine responses, persistent infection and viral evolution to inform public health policy.
Trial registration number ISRCTN45176516.
- inflammatory bowel disease
- autoimmune disease
- COVID-19
- inflammatory diseases
- infliximab
- vedoluzimab
- clarity
Data availability statement
Data are available on reasonable request. The study protocol including the statistical analysis plan is available at www.clarityibd.org. Individual participant deidentified data that underlie the results reported in this article will be available immediately after publication for a period of 5 years. The data will be made available to investigators whose proposed use of the data has been approved by an independent review committee. Analyses will be restricted to the aims in the approved proposal. Proposals should be directed to tariq.ahmad1@nhs.net; to gain access, data requestors will need to sign a data access agreement.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
- inflammatory bowel disease
- autoimmune disease
- COVID-19
- inflammatory diseases
- infliximab
- vedoluzimab
- clarity
Significance of this study
What is already known on this subject?
Antitumour necrosis factor (anti-TNF) drugs are effective treatments for immune-mediated inflammatory diseases (IMIDs); however, by suppressing immune responses, they impair vaccine effectiveness and increase susceptibility to serious infection.
In the early phase of the COVID-19 pandemic, patients with IMIDs treated with anti-TNF drugs were subject to the most restrictive public health measures.
Registry studies have not reported an increased risk of adverse outcomes from SARS-CoV-2 in patients treated with anti-TNF therapies. However, the impact of these therapies on serological responses and subsequent immunity to SARS-CoV-2 infection remains unknown.
What are the new findings?
Rates of symptomatic and proven SARS-CoV-2 infection were similar between infliximab-treated and vedolizumab-treated patients with IBD.
Seroprevalence, seroconversion and the magnitude of anti-SARS-CoV-2 antibody reactivity was significantly attenuated in infliximab-treated patients compared with vedolizumab-treated patients.
Concomitant immunomodulator use with a thiopurine or methotrexate further blunted serological responses to SARS-CoV-2 infection in infliximab-treated patients, with only a third of patients having detectable anti-SARS-CoV-2 antibodies.
Significance of this study
How might it impact on clinical practice in the foreseeable future?
For the individual anti-TNF-treated patient, lower rates of seroconversion and reduced anti-SARS-CoV-2 antibody reactivity levels may increase their susceptibility to recurrent COVID-19.
Impaired serological responses might lead to chronic nasopharyngeal colonisation that may act as a reservoir to drive persistent transmission and the evolution of new SARS-CoV-2 variants.
Serological testing and virus surveillance should be considered to detect suboptimal vaccine responses, persistent infection and viral evolution to inform public health policy.
If attenuated serological responses following vaccination are also observed, then modified immunisation strategies will need to be designed for millions of patients worldwide.
Introduction
Induction of protective immunity following SARS-CoV-2 infection and/or vaccination is critical to suppress transmission. By suppressing immune responses, biological and immunosuppression therapies may lead to chronic SARS-CoV-2 infection and have recently been implicated in the evolution and emergence of novel variants.1–3
Immune-mediated inflammatory diseases (IMIDs) including IBD, the inflammatory arthritides and psoriasis affect about 3%–7% of Western populations.4 5 Drugs targeting tumour necrosis factor (TNF) are the most frequently prescribed biological therapies used in the treatment of IMIDs with over 2 million patients receiving treatment worldwide.6 However, anti-TNF drugs impair protective immunity following pneumococcal,7 influenza8 and viral hepatitis9 vaccinations and increase the risk of serious infection, most notably with respiratory pathogens.10 Consequently, in the early phase of the COVID-19 pandemic, patients with IMIDs treated with anti-TNF drugs were advised to follow strict social distancing measures, and some, depending on the severity of their condition, were advised to shield.11 Data from disease-specific registries are reassuring, however, citing similar rates and risk factors for SARS-CoV-2 infection, hospitalisation and outcomes to background populations.12–14 Whether anti-TNF drugs impair serological responses and subsequent immunity to SARS-CoV-2 infection is unknown.
We hypothesised that anti-SARS-CoV-2 antibody responses would be impaired following SARS-CoV-2 infection in patients with IBD treated with infliximab, a commonly prescribed anti-TNF drug. To test this hypothesis, we compared antibody responses in patients with IBD treated with infliximab with a reference cohort treated with vedolizumab. Vedolizumab is a gut-selective anti-integrin α4β7 monoclonal antibody, administered in hospital with the same dosing schedule as infliximab and is not associated with increased susceptibility to systemic infection or attenuated serological responses to vaccination.15
Objectives
We aimed to define, in patients with IBD, whether biological class, concomitant use of an immunomodulator and/or social distancing measures impact:
Seroprevalence of SARS-CoV-2.
Subsequent seroconversion in patients with infection confirmed by prior PCR testing.
Magnitude of anti-SARS-CoV-2 reactivity.
Methods
Patient and settings
ImpaCt of bioLogic therApy on saRs-cov-2 Infection and immuniTY (CLARITY) IBD is a UK wide, multicentre, prospective observational cohort study investigating the impact of infliximab and vedolizumab and/or concomitant immunomodulators (thiopurines or methotrexate) on SARS-CoV-2 acquisition, illness and immunity in patients with IBD.
Consecutive patients were recruited at the time of attendance at infusion units from 92 National Health Service (NHS) hospitals across the UK (see online supplemental table S1) between 22 September 2020 and 23 December 2020.
Supplemental material
The eligibility criteria were:
Age 5 years and over.
Diagnosis of IBD.
Current treatment with infliximab or vedolizumab for 6 weeks or more, with at least one dose of drug received in the past 16 weeks.
Patients were excluded if they had participated in a SARS-CoV-2 vaccine trial.
Here we report the seroprevalence of anti-SARS-CoV-2 antibodies at entry to the CLARITY IBD study.
Outcome measures
The primary outcome was the proportion of participants with a positive anti-SARS-CoV-2 antibody test. Secondary outcomes were the proportion of participants with a positive anti-SARS-CoV-2 antibody following a positive PCR test to SARS-CoV-2 and the magnitude of the anti-SARS-CoV-2 antibody reactivity.
Variables
Variables recorded by participants included demographics (age, sex, ethnicity, comorbidities, height and weight, smoking status and postcode), IBD disease activity (PRO2),16 17 IBD-related quality of life (IBD control),18 mental well-being (Patient Health Questionnaire depression scale19 and General Anxiety Disorder Assessment),20 SARS-CoV-2 outcomes aligned to the COVID-19 symptoms study21 (symptoms, previous testing and hospital admissions for COVID-19) and social distancing behaviour during the lockdown periods. During lockdown, the population of the UK was instructed to adhere to restrictions on social and professional activities with specific advice to vulnerable groups to undertake more extreme social exclusion measures referred to as shielding.11
Study sites completed data relating to IBD history (age at diagnosis, disease duration and phenotype according to the Montreal classifications,22 previous surgeries and duration of current biological and immunomodulator therapy).
Wherever possible, data were entered electronically into a purpose-designed REDCap database hosted at the Royal Devon and Exeter NHS Foundation Trust.23 At sites without access to electronic devices or the internet, participants completed their questionnaires on paper case record forms that were subsequently entered by local research teams.
Case definition
Cases were defined according to the recently published WHO framework.24 In brief, this framework uses symptoms and the results of nucleic acid amplification testing to determine whether patients are suspected, probable or confirmed cases of COVID-19. Participants who reported fever and cough, or anosmia/ageusia or any three or more of the following symptoms: fever, cough, general weakness/fatigue, myalgia, sore throat, coryza, dyspnoea, and altered mental status were considered suspected/probable COVID-19 cases. We omitted the GI symptoms because patients with active IBD may suffer anorexia, nausea, vomiting and diarrhoea. We linked our data by NHS number or Community Health Index to Public Health England, Scotland and Wales who archive dates and results of all SARS-CoV-2 PCR tests undertaken in the UK. Confirmed cases were those participants with a positive PCR test to SARS CoV-2.
Laboratory methods
Laboratory analyses were performed at the Academic Department of Blood Sciences at the Royal Devon and Exeter NHS Foundation Trust. We used the Roche Elecsys Anti-SARS-CoV-2 immunoassay to detect antibodies to SARS-CoV-2 in serum samples.25 This sandwich electrochemiluminescence immunoassay uses a recombinant protein of the nucleocapsid antigen for the determination of antibodies against SARS-CoV-2. The electrochemiluminescence signal from a negative and positive calibrator is assigned a value of 0.8 and 1.2, respectively, and a cut-off is set at a signal equivalent to 1. The electrochemiluminescence signal from the reaction product of the sample is compared with the cut-off signal and expressed as positive when ≥1.0 or negative when <1, as well as quantitatively in the form of a cut-off index (COI; calculated by sample signal/cut-off signal).
In house assay validation experiments demonstrated the intra-assay and interassay coefficient of variation were 2.2% and 7.0%, respectively. No effect was observed on recovery of anti-SARS-CoV-2 antibodies following four freeze/thaw cycles. SARS-CoV-2 antibodies were stable in uncentrifuged blood and serum at ambient temperature for up to 7 days permitting postal transport from research sites to the central laboratory. No analytical interference was observed for the detection of anti-SARS-CoV-2 with infliximab or vedolizumab up to 10 000 mg/L and 60 000 mg/L, respectively, or with antidrug antibodies to infliximab or vedolizumab up to 400 AU/mL and 38 AU/mL, respectively.
Study size
Limited data are available regarding the risk of SARS-CoV-2 in patients with IBD to inform sample size calculations.
The following assumptions were made to determine our sample size:
Proportion of patients treated with each drug(s): vedolizumab: 30% (20% with concomitant immunomodulator), infliximab: 70% (60% with concomitant immunomodulator).
Seroprevalence of SARS-CoV-2 in the background population: 0.05.
OR for SARS-CoV-2 seropositivity with immunomodulator use: 0.8.
OR SARS-CoV-2 seropositivity for infliximab versus vedolizumab:≤0.7.
Attrition rate: 20%.
We calculated that a sample size of 6970 patients would provide 80% power for the comparison of infliximab versus vedolizumab, controlling for immunosuppressant status in a multivariable logistic regression model at the 0.05 significance level.
Ethical consideration and roles of funders
CLARITY IBD is an investigator-led, UK National Institute for Health Research COVID-19 urgent public health study funded by the Royal Devon and Exeter NHS Foundation Trust, Hull University Teaching Hospital NHS Trust and by unrestricted educational grants from F. Hoffmann-La Roche AG (Switzerland), Biogen GmbH(Switzerland), Celltrion Healthcare (South Korea) and Galapagos NV (Belgium).
None of our funding bodies had any role in study design, data collection or analysis, writing or decision to submit for publication. Patients were included after providing informed, written consent. The sponsor was the Royal Devon and Exeter NHS Foundation Trust. The protocol is available online at https//www.clarityibd.org. The study was registered with the ISRCTN registry.
Statistics
Statistical analyses were undertaken in R V.4.0.3 (R Foundation for Statistical Computing, Vienna, Austria). All tests were two tailed, and p values<0.05 were considered significant. We included participants in the primary analysis if they had completed the patient questionnaire and had an anti-SARS-CoV-2 serology result at visit 1. We included patients with missing clinical data in analyses for which they had data and have specified the denominator for each variable. Continuous data were reported as median and IQR, and discrete data as numbers and percentages, unless otherwise stated. We used patients’ postcodes to assign them to one of the ten UK administrative regions and present seroprevalence rates mapped to these regions. We also used postcodes to derive participants’ income and employment deprivation scores using combined English and Welsh data from 201926 and Scottish data from 2020.27 Univariable analyses, using Fisher’s exact and Mann-Whitney U tests were used to identify demographic, disease and treatment related factors associated with SARS-CoV-2 seropositivity. A priori, we included age, sex, ethnicity, region, income deprivation score, comorbidity, body mass index and social distancing measures that are known to affect SARS-CoV-2 acquisition and COVID-19 outcomes28 alongside IBD diagnosis, biological therapies, immunomodulator and 5-aminosalicylate use. We used multivariable logistic regression models to identify factors independently associated with seropositivity.
We undertook Fisher’s exact and Mann-Whitney U tests to compare the rates of, and time to, seroconversion in infliximab-treated and vedolizumab-treated patients with confirmed COVID-19 and to identify factors associated with failure of seroconversion in infliximab-treated patients. We explored the magnitude of antibody reactivity using density plots, stratified by drug exposure among participants with a positive PCR to anti-SARS-CoV-2 at least 2 weeks prior to measurement of serology.
We conducted sensitivity analyses using propensity matching to account for significant differences in baseline variables between infliximab-treated and vedolizumab-treated patients using the MatchIt package.29 Patients were matched exactly on diagnosis, immunomodulator use and cancer and then using optimal matching, on age, comorbidities, ethnicity and presence of active disease.
Results
Patient characteristics
Between 22 September 2020 and 23 December 2020, 7226 patients were recruited from 92 UK hospitals. Serum samples and completed questionnaires were available in 96.0% (6935/7226) patients. Of these, 67.6% (4685/6935) were treated with infliximab and 32.4% (2250/6935) were treated with vedolizumab. Participant characteristics are shown in table 1.
Baseline characteristics stratified by biological therapy
Adherence to social distancing measures during the UK lockdown period between April and July 2020 and exposure to COVID-19 cases were similar between infliximab and vedolizumab treated patients (table 1). Fewer infliximab-treated patients were tested by PCR for SARS-CoV-2 (36.5% (1712/4685) vs 39.0% (877/2250), p=0.050). There were no differences between the proportions of infliximab-treated and vedolizumab-treated patients who: reported symptoms of suspected or probable COVID-19 (8.3% (389/4685) vs 8.9% (201/2250), p=0.38); tested positive by PCR for SARS-CoV-2 (5.2% (89/1712) vs 4.3% (38/877), p=0.39); or were hospitalised with confirmed COVID-19 (0.2% (8/4685) vs 0.2% (5/2250), p=0.77).
Seroprevalence of anti-SARS-CoV-2 antibodies in anti-TNF and vedolizumab-treated patients
Overall, the seroprevalence of anti-SARS-CoV-2 antibodies was 4.3% (295/6935, 95% CI 3.8% to 4.8%). The proportion of patients with a positive anti-SARS-CoV-2 antibody test was lower in infliximab-treated than vedolizumab-treated patients (3.4% (161/4685) vs 6.0% (134/2250), p<0.0001) (table 2).
Seroprevalence to anti-SARS-CoV-2, stratified by baseline characteristics
Seropositivity was also associated with younger age, non-white ethnicity, UK region, higher income deprivation score, having never smoked, UC, no concomitant immunomodulator use, recent steroid use, exposure to confirmed cases of COVID-19, reported symptoms of suspected or probable COVID-19, and social distancing measures during the UK government’s lockdown period (tables 2 and 3, See online supplemental figure S1).
Baseline characteristics, stratified by baseline anti-SARS-CoV-2 antibody status
Multivariable logistic regression analyses confirmed that infliximab (vs vedolizumab; OR 0.66 (95% CI 0.51 to 0.87), p=0.0027) and immunomodulator use (OR 0.70 (95% CI 0.53 to 0.92), p=0.012) were independently associated with lower seropositivity (figure 1). Conversely, non-white ethnicity, several UK regions, higher income deprivation score and non-adherence to social distancing measures were independently associated with an increased risk of SARS-CoV-2 seropositivity. There was no significant interaction between the effect of infliximab (vs vedolizumab) and immunomodulator use (OR for interaction term 1.03 (95% CI 0.57 to 1.92), p=0.92). In our propensity matched analysis, we confirmed lower seroprevalence in infliximab-treated compared with vedolizumab-treated patients 3.9% (67/1704) versus 6.2% (105/1707) p=0.0037 (online supplemental table S2).

Forest plot showing the coefficients from a multivariable logistic regression model of associations with a positive anti-SARS-CoV-2 antibody. abbreviations: 5-ASA, 5-aminosalicylates; IBDU, IBD unclassified.
Seroconversion in patients with confirmed SARS-CoV-2 infection
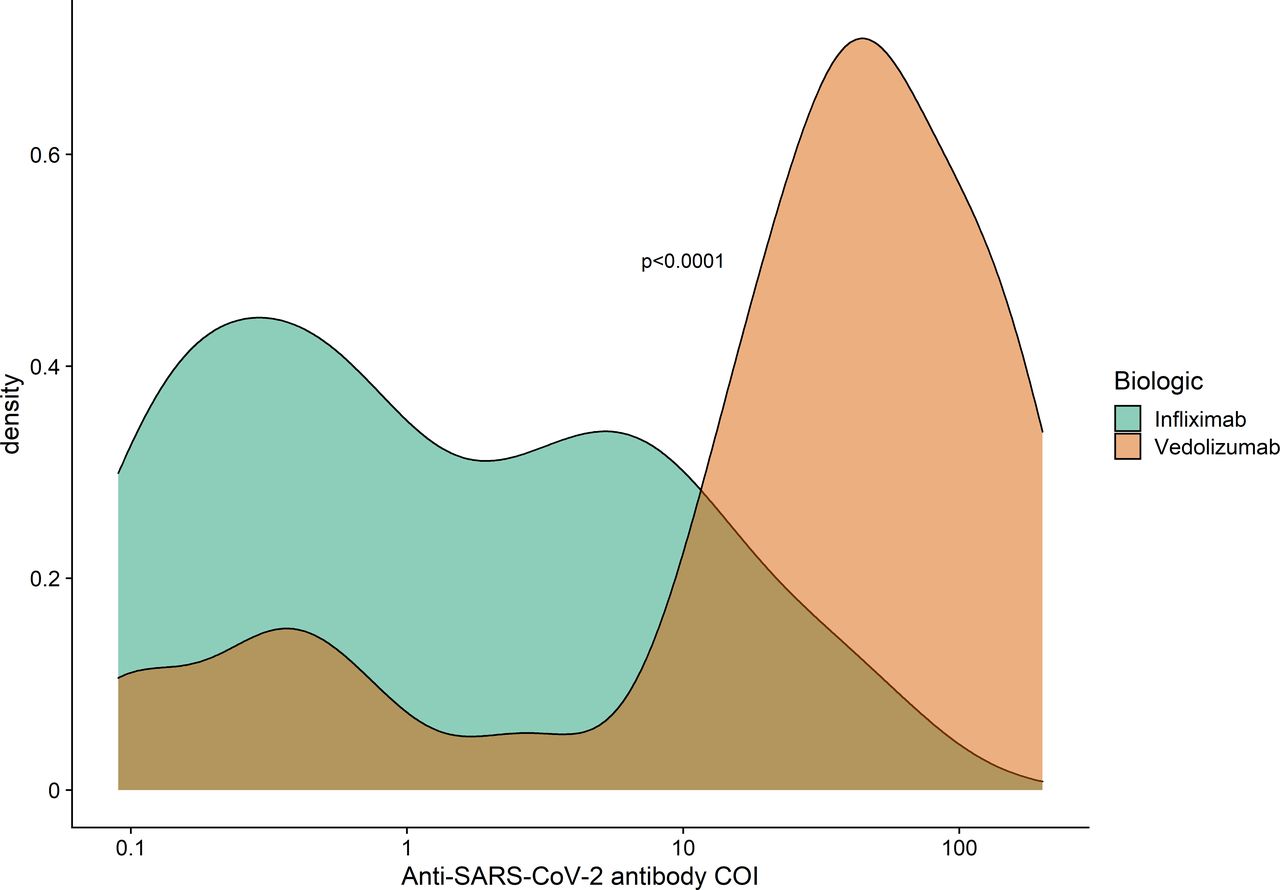
Sensitivity analyses in participants with confirmed SARS-CoV-2 infection demonstrated that fewer infliximab-treated than vedolizumab-treated patients had seroconverted (48% (39/81) vs 83% (30/36), p=0.00044). The magnitude of anti-SARS-CoV-2 reactivity was lower in patients with previous PCR-confirmed SARS-CoV-2 infection treated with infliximab than with vedolizumab (median 0.8 COI (0.2–5.6) vs 37.0 (15.2–76.1), p<0.0001; figure 2). This difference was also seen restricting our analyses to participants whose antibody reactivity results were above the threshold (1 COI) for seropositivity (p<0.0001; see online supplemental figure S2).
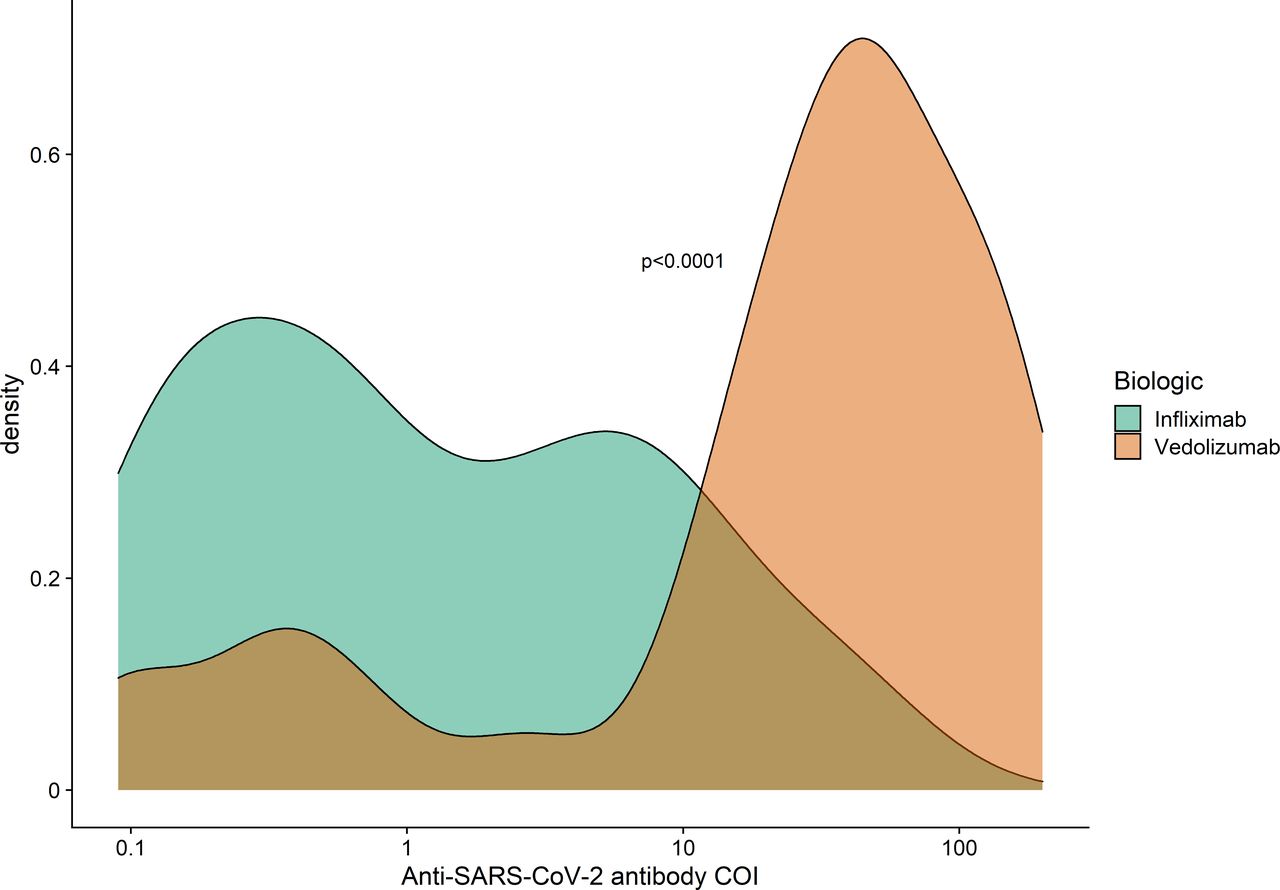
Density plot of the magnitude of anti-SARS-CoV-2 antibody reactivity stratified by biological therapy among participants who had a positive PCR to anti-SARS-CoV-2 at least 2 weeks prior to their serology sample. COI, cut-off index.
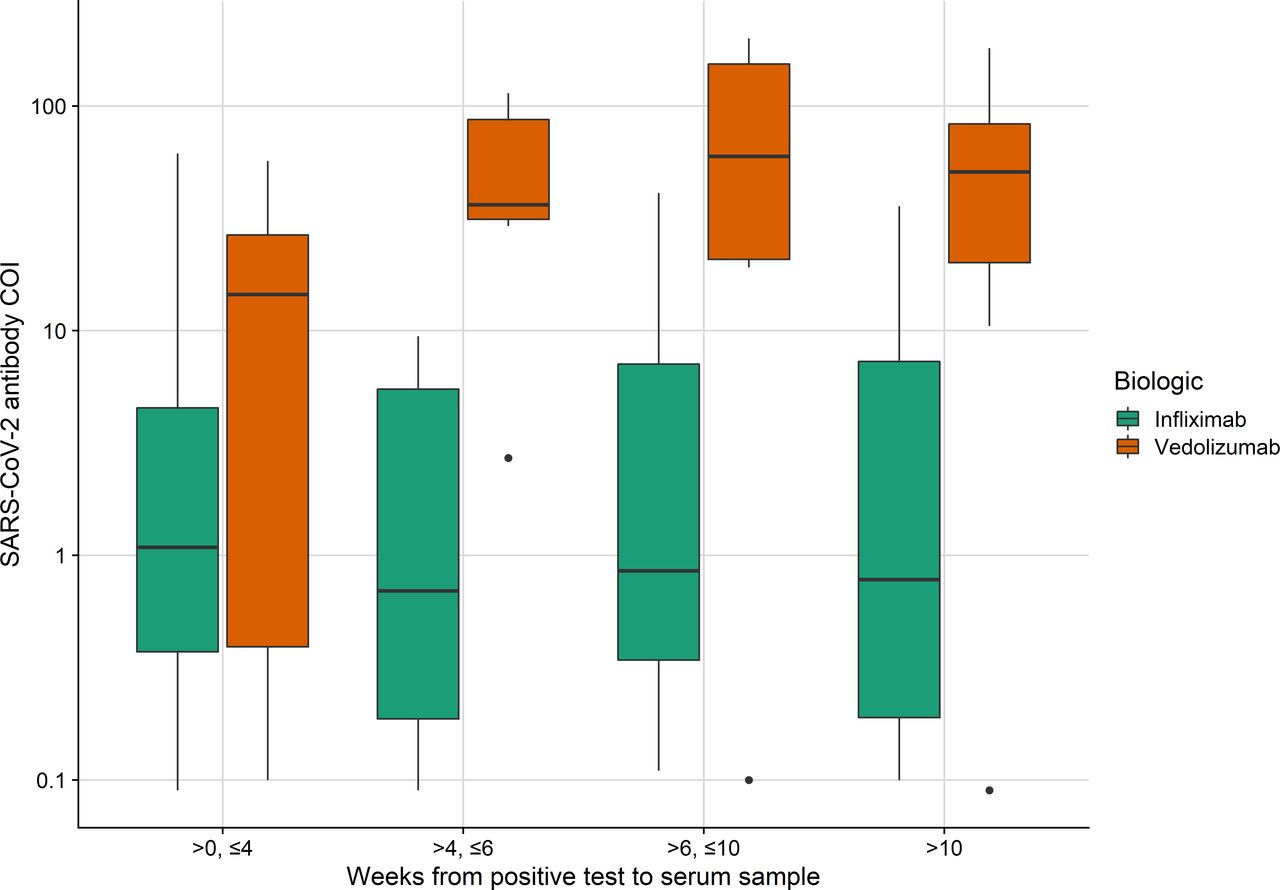
Failure of seroconversion was associated with concomitant immunomodulator use. In patients treated with infliximab alone, the seroconversion rate was 60% (24/40) and in patients treated with infliximab and immunomodulator combination therapy, the rate was 37% (15/41, p=0.046). There was also a significant difference in the magnitude of anti-SARS-CoV-2 reactivity (p=0.035; see online supplemental figure S3). The median interval from a positive PCR test to serological testing at recruitment in infliximab-treated patients was 32 days (IQR 20–54) and for vedolizumab-treated patients was 40 days (IQR 24–83) (p=0.082). An increase in anti-SARS-CoV-2 antibody reactivity was observed 4 weeks after a positive PCR test in vedolizumab-treated patients (47.2 COI (IQR 24.1–113.0) vs 14.5 COI (IQR 0.4–30.7), p=0.0079) but not infliximab-treated patients (0.7 COI (IQR 0.2–7.5) vs 1.1 COI (IQR 0.4–4.5), p=0.70) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Boxplot of the magnitude of anti-SARS-CoV-2 antibody reactivity stratified by biological therapy and time since prior positive PCR test. COI, cut-off index.
Discussion
We have shown that infliximab-treated patients have attenuated serological responses to SARS-CoV-2 infection with lower seroprevalence, seroconversion and antibody reactivity. Similar rates of symptomatic and proven SARS-CoV-2 infection and hospitalisations between infliximab-treated and vedolizumab-treated patients suggest that our findings cannot be explained by differences in acquisition or severity of infection alone. Rather, infliximab seems to be directly influencing the serological response to infection. Concomitant immunomodulator use with a thiopurine or methotrexate further blunted serological responses to both drugs with fewer than half of patients (37%) having detectable anti-SARS-CoV-2 antibodies after a median of 5.4 weeks following PCR confirmed infection.
Infliximab may directly impede the immune mechanisms responsible for generating antibody responses. This is biologically plausible, since the proinflammatory actions of TNF include stimulation of B cell immunoglobulin synthesis, induction of germinal centre formation, costimulation of antigen-activated T cells and maturation of antigen presenting cells.30–32
Impaired serological responses to SARS-CoV-2 infection might have important implications for global public health policy and individual anti-TNF treated patients. From a public health perspective, impaired serological responses might lead to chronic nasopharyngeal colonisation that may act as a reservoir to drive persistent transmission and the evolution of new SARS-CoV-2 variants.2 Virus surveillance will define if persistent infection and viral evolution occurs in this patient group.3
For the individual anti-TNF treated patient, lower rates of seroconversion and reduced anti-SARS-CoV-2 antibody reactivity levels may ultimately increase their susceptibility to recurrent COVID-19.
Accepting that vaccination is critical to suppress transmission, serology testing should be considered to detect suboptimal vaccine responses to inform the need for the most restrictive social distancing measures to protect patients and public health. If attenuated serological responses following vaccination are observed, then modified vaccination schedules given in combination might need to be considered in these patients.
Any negative impact on seroconversion following infection or vaccination needs to be balanced against theoretical benefits for the individual patient of reducing the excessive cytokine production that characterises severe COVID-19 disease. Indeed, this is the rationale behind the proposals for trials of anti-TNF therapy in severe COVID-19 (ISRCTN40580903 and ISRCTN33260034).33
Our study has other important findings. We have identified associations of SARS-CoV-2 seropositivity with non-white ancestry and non-adherence to social distancing guidance. These findings are consistent with observations reported in general non-immunosuppressed populations.28 The mechanisms underlying these associations are complex and multifactorial and likely include multigenerational living, at-risk employment, inability to work from home, socioeconomic deprivation and religious congregation.
The region-specific seroprevalence rates for vedolizumab-treated patients are consistent with those reported in the general UK population. While direct comparisons with other datasets are limited, confounded in part by differences in the time of testing during the pandemic and the diagnostic accuracies of the anti-SARS-CoV-2 assays used, this adds to the evidence that patients with IBD are at a similar risk of SARS-CoV-2 infection as the general population.34
The main strength of this study was our recruitment of over 7000 consecutive patients within a narrow window mitigating against the potential for time during the pandemic course to be a significant covariate. Other strengths include comprehensive electronic collection of patient-reported outcomes, linkage with SARS-CoV-2 public health testing data, case ascertainment aligned with the WHO criteria, inclusion of social distancing behaviours and the use of a sensitive and specific serological assay.35
Limitations
We acknowledge, however, the following limitations. First, it is not known whether attenuated immune responses in infliximab-treated patients translates into increased risk of infection. Moreover, we only assessed humoral responses to infection, and it is likely that protective immunity additionally requires induction of memory T cell responses. Second, our patient-reported data are subject to recall bias that may have underestimated the prevalence of possible COVID-19 symptoms. Third, the only anti-TNF drug investigated in this study was infliximab. However, we suspect that our key findings apply to other anti-TNF monoclonal antibodies used to treat IMIDs, including adalimumab, certolizumab and golimumab.
Conclusions
In summary, infliximab therapy is associated with attenuated serological responses to SARS-CoV-2 infection. Poor antibody responses in infliximab-treated patients were observed despite similar rates of symptomatic and proven SARS-CoV-2 infection as vedolizumab-treated patients. Anti-SARS-CoV-2 antibody responses were further attenuated in infliximab recipients concomitantly treated with immunomodulators, including thiopurines and methotrexate.
Impaired serological responses to SARS-CoV-2 infection might have important implications for global public health policy and millions of anti-TNF treated patients. Serological testing and virus surveillance should be considered to detect suboptimal vaccine responses, persistent infection and viral evolution to inform public health policy.
Data availability statement
Data are available on reasonable request. The study protocol including the statistical analysis plan is available at www.clarityibd.org. Individual participant deidentified data that underlie the results reported in this article will be available immediately after publication for a period of 5 years. The data will be made available to investigators whose proposed use of the data has been approved by an independent review committee. Analyses will be restricted to the aims in the approved proposal. Proposals should be directed to tariq.ahmad1@nhs.net; to gain access, data requestors will need to sign a data access agreement.
Ethics statements
Ethics approval
The Surrey Borders Research Ethics committee approved the study (REC reference: REC 20/HRA/3114) in September 2020.
Acknowledgments
CLARITY IBD is a UK National Institute for Health Research (NIHR) Urgent Public Health Study. The NIHR Clinical Research Network supported study set-up, site identification and delivery of this study. This was facilitated by Professor Mark Hull, the national specialty lead for gastroenterology. We acknowledge the contribution of our Patient Advisory Group who helped shape the trial design around patient priorities. Our partner, Crohn’s and Colitis UK (CCUK), continues to support this group and participate in study management team meetings. Laboratory tests were undertaken by the Exeter Blood Sciences Laboratory at the Royal Devon and Exeter NHS Foundation Trust. The Exeter NIHR Clinical Research Facility coordinated sample storage and management. Tariq Malik and James Thomas from Public Health England; Guy Stevens, Katie Donelon and Elen de Lacy from Public Health Wales; and Johanna Bruce from Public Health Scotland supported linkage of central SARS-CoV-2 PCR test results with study data. Roche Diagnostics Limited provided the Elecsys Anti-SARS-CoV-2 immunoassay for the study. SL is supported by a Wellcome GW4-CAT fellowship. NC acknowledges support from CCUK. CAL acknowledges support from the NIHR Newcastle Biomedical Research Centre and the support of the Programmed Investigation Unit at Royal Victoria Infirmary, Newcastle on Tyne. TR acknowledges support with recruitment from the NIHR Cambridge Biomedical Research Centre (BRC). RKR is supported by an NHS Research Scotland Senior Research Fellowship. NP is supported by the NIHR Imperial BRC. We acknowledge the study coordinators of the Exeter Inflammatory Bowel Disease and Pharmacogenetics Research Group: Marian Parkinson and Helen Gardner-Thorpe for their ongoing administrative support to the study. The sponsor of the study was the Royal Devon and Exeter NHS Foundation Trust.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrNickKennedy, @JamesGoodhand, @clairebewshea, @rachelnice3, @SimengLin, @nchanchlani1, @jrbutterworth1, @rachelcooney7, @nickcrofty, @DrAilsaHart, @klaartjekok, @DrChrisLamb, @jklimdi, @j0nnymac1, @doc_ibd, @CharlieMuz, @RichardPollok, @DrPhilipJSmith, @jack_bowdenjack, @T_J_McDonald, @charlie_lees, @NhsSeb, @NickPowellLab, @tariqahmadIBD
NP and TA contributed equally.
NAK and JRG contributed equally.
Collaborators Contributors to the CLARITY IBD study: Barts Health NHS Trust Klaartje Kok, Farjhana Bokth, Bessie Cipriano, Caroline Francia, Nosheen Khalid, Hafiza Khatun, Ashley Kingston, Irish Lee, Anouk Lehmann, Kinnari Naik, Elise Pabriaga, Nicolene Plaatjies, Kevin Samuels. Barts Health NHS Trust (paediatric): Bessie Cipriano, Kevin Samuels, Nicolene Plaatjies, Hafiza Khatun, Farjana Bokth, Elise Pabriaga, Caroline Francia. Basingstoke and North Hampshire Hospital: Rebecca Saich, Hayley Cousins, Wendy Fraser, Rachel Thomas, Matthew Brown, Benjamin White. Birmingham Women's and Children's NHS Foundation Trust: Rafeeq Muhammed, Rehana Bi, Catherine Cotter, Jayne Grove, Kate Hong, Ruth Howman, Monica Mitchell, Sugrah Sultan. Bolton NHS Foundation Trust: Salil Singh, Chris Dawe, Robert Hull, Natalie Silva. Borders General Hospital: Manning Jansen, Lauren Jansen. Calderdale and Huddersfield NHS Foundation Trust: Sunil Sonwalkar, Naomi Chambers, Andrew Haigh, Lear Matapure Cambridge University Hospitals NHS Foundation Trust: Tim Raine, Varun George, Christina Kapizioni, Konstantina Strongili. Chelsea and Westminster Hospital NHS Foundation Trust: Tina Thompson, Philip Hendy, Rhian Bull, Patricia Costa, Lisa Davey, Hayley Hannington, Kribashnie Nundlall, Catarina Martins, Laura Avanzi, Jaime Carungcong, Sabrina Barr. Chesterfield Royal Hospital: Kath Phillis, Rachel Gascoyne. Countess Of Chester Hospital NHS Foundation Trust: Ian London, Jenny Grounds, Emmeline Martin, Susie Pajak. Dartford and Gravesham NHS Trust: Ben Warner, Carmel Stuart, Louise Lacey. Darlington Memorial Hospital: Anjan Dhar, Ellen Brown, Amanda Cowton, Kimberley Stamp. The Dudley Group NHS Foundation Trust: Shanika de Silva, Clare Allcock, Philip Harvey. East and North Hertfordshire NHS Trust: Johanne Brooks, Pearl Baker, Hannah Beadle, Carina Cruz, Debbie Potter. East Lancashire Hospitals NHS Trust: Joe Collum, Farzana Masters. East Suffolk and North Essex NHS Foundation Trust: Achuth Shenoy, Alison O'Kelly. Glangwili Hospital: Aashish Kumar, Samantha Coetzee, Mihaela Peiu. Great Ormond Street Hospital: Edward Gaynor, Sibongile Chadokufa, Bonita Huggett, Hamza Meghari, Sara El-Khouly, Fevronia Kiparissi, Waffa Girshab. Great Western Hospitals NHS Foundation Trust: Andrew Claridge, Emily Fowler, Laura McCafferty. Guy's and St Thomas' NHS Foundation Trust: Peter Irving, Karolina Christodoulides, Angela Clifford, Patrick Dawson, Sailish Honap, Samuel Lim, Raphael Luber, Karina Mahiouz, Susanna Meade, Parizade Raymode, Rebecca Reynolds, Anna Stanton, Sherill Tripoli, Naomi Hare. The Hillingdon Hospitals NHS Foundation Trust: Yih Harn Siaw, Lane Manzano, Jonathan Segal, Ibrahim Al-Bakir, Imran Khakoo. Homerton University Hospital Foundation Trust: Nora Thoua, Katherine Davidson, Jagrul Miah, Alex Hall. Hull University Teaching Hospitals NHS Trust: Shaji Sebastian, Melony Hayes, Sally Myers, Alison Talbot, Jack Turnbull, Emma Whitehead, Katie Stamp, Alison Pattinson, Verghese Mathew, Leanne Sherris. Imperial College Healthcare NHS Trust: Lucy Hicks, Tara-Marie Byrne, Leilani Cabreros, Hannah Downing-Wood, Sophie Hunter, Mohammad Aamir Saifuddin, Hemanth Prabhudev, Sharmili Balarajah. James Paget University Hospitals NHS Foundation Trust: Helen Sutherland. Kettering General Hospital: Ajay M Verma, Juliemol Sebastian, Mohammad Farhad Peerally. King's College Hospital NHS Foundation Trust: Alexandra Kent, Lee Meng Choong, Benedetta Pantaloni, Pantelis Ravdas. King's College Hospital NHS Foundation Trust (paediatric): Babu Vadamalayan. King’s Mill Hospital: Stephen Foley, Becky Arnold, Cheryl Heeley, Wayne Lovegrove. Liverpool University Hospitals NHS Foundation Trust: Philip J Smith, Giovanna Bretland, Sarah King, Martina Lofthouse, Lindsey Rigby, Sreedhar Subramanian, David Tyrer, Kate Martin, Christopher Probert. London North West University Healthcare NHS Trust: Nik Kamperidis, Temi Adedoyin, Manisha Baden, Jeannette Brown, Feba Chacko, Michela Cicchetti, Mohammad Saifuddin, Priya Yesupatham. Maidstone and Tunbridge Wells NHS Trust: Rohit Gowda, Maureen Williams. Manchester University NHS Foundation Trust: Karen Kemp, Rima Akhand, Glaxy Gray, Anu John, Maya John, Diamond Sathe, Jennifer Soren. The Mid Yorkshire Hospitals NHS Trust: Michael Sprakes, Julie Burton, Patricia Kane, Stephanie Lupton Milton Keynes University Hospital: George MacFaul, Diane Scaletta, Loria Siamia. Newcastle Hospitals NHS Foundation Trust: Chris Lamb, Mary Doona, Ashleigh Hogg, Lesley Jeffrey, Andrew King, R Alexander Speight. Ninewells Hospital & Medical School: Craig Mowat, Debbie Rice, Susan MacFarlane, Anne MacLeod, Samera Mohammed. Norfolk and Norwich University Hospitals NHS Foundation Trust: Mary Anne Morris, Louise Coke, Grace Hindle, Eirini Kolokouri, Catherine Wright. North Bristol NHS Trust: Melanie Lockett, Charlotte Cranfield, Louise Jennings, Ankur Srivastava, Lana Ward, Nouf Jeynes. North Tyneside General Hospital: Praveen Rajasekhar, Lisa Gallagher, Linda Patterson, Jill Ward, Rae Basnett, Judy Murphy, Lauren Parking, Emma Lawson. Nottingham University Hospitals NHS Trust: David Devadason, Gordon Moran, Neelam Khan, Lauren Tarr. The Pennine Acute Hospitals NHS Trust: Jimmy Limdi, Kay Goulden, Asad Javed, Lauren McKenzie. Portsmouth Hospitals NHS Trust: Pradeep Bhandari, Michelle Baker-Moffatt, Joanne Dash. The Queen Elizabeth Hospital Kings Lynn NHS Trust: Alan Wiles, Hannah Bloxham, Jose Dias, Ellie Graham. Queen Elizabeth University Hospital, Glasgow: Jonathan Macdonald, Shona Finan, Faye McMeeken, Stephanie Shields, John Paul Seenan. Royal Berkshire NHS Foundation Trust: Des DeSilva, Ofori Boateng, Holly Lawrence, Susanna Malkakorpi. The Royal Bournemouth and Christchurch Hospitals NHS Foundation Trust: Simon Whiteoak, Kelli Edger-Earley. Royal Cornwall Hospitals NHS Trust: Sarah Ingram, Sharon Botfield, Fiona Hammonds, Clare James. Royal Devon and Exeter NHS Foundation Trust: Tariq Ahmad, Gemma Aspinall, Sarah Hawkins, Suzie Marriott, Clare Redstone, Halina Windak. Royal Free London NHS Foundation Trust: Charles Murray, Cynthia Diaba, Fexy Joseph, Glykeria Pakou. Royal Glamorgan Hospital: James Berrill, Natalie Stroud, Carla Pothecary, Lisa Roche, Keri Turner, Lisa Deering, Lynda Israel. Royal Gwent Hospital: Evelyn Baker, Sean Cutler, Rina Mardania Evans, Maxine Nash. Royal Hampshire County Hospital: John Gordon, Emma Levell, Silvia Zagalo. Royal Hospital for Sick Children, Edinburgh: Richard Russell, Paul Henderson, Margaret Millar. Royal Manchester Children's Hospital: Andrew Fagbemi, Felicia Jennings, Imelda Mayor, Jill Wilson. Royal Surrey County Hospital: Christopher Alexakis, Natalia Michalak. Royal United Hospitals Bath: John Saunders, Helen Burton, Vanessa Cambridge, Tonia Clark, Charlotte Ekblad, Sarah Hierons, Joyce Katebe, Emma Saunsbury, Rachel Perry. The Royal Wolverhampton NHS Trust: Matthew Brookes, Kathryn Davies, Marie Green, Ann Plumbe. Salford Royal NHS Foundation Trust: Clare Ormerod, Helen Christensen, Anne Keen, Jonathan Ogor. Salisbury District Hospital: Alpha Anthony, Emily Newitt. Sandwell and West Birmingham NHS Trust: Edward Fogden, Kalisha Russell. Sheffield Teaching Hospitals NHS Foundation Trust: Anne Phillips, Muaad Abdulla. Shrewsbury and Telford Hospital NHS Trust: Jeff Butterworth, Colene Adams, Elizabeth Buckingham, Danielle Childs, Alison Magness, Jo Stickley. Singleton Hospital: Caradog Thomas, Elaine Brinkworth, Lynda Connor, Amanda Cook, Tabitha Rees. Somerset NHS Foundation Trust: Emma Wesley, Alison Moss. South Tees Hospitals NHS Foundation Trust: Arvind Ramadas, Julie Tregonning. Southend University Hospital NHS Foundation Trust: Ioannis Koumoutsos, Viji George, Swapna Kunhunny, Sophie Laverick. St George's University Hospitals NHS Foundation Trust: Kamal Patel, Mariam Ali, Hilda Mhandu, Aleem Rana, Katherine Spears, Joana Teixeira, Richard Pollok, Mark Mencias, Abigail Seaward. St George's University Hospitals NHS Foundation Trust (paediatric): Nicholas Reps, Rebecca Martin. St James’s University Hospital: Christian Selinger, Jenelyn Carbonell, Felicia Onovira, Doris Quartey. Stockport NHS Foundation Trust: Zahid Mahmood, Racheal Campbell, Liane Marsh. Surrey and Sussex Healthcare NHS Trust: Monira Rahman, Sarah Davies, Ruth Habibi, Ellen Jessup-Dunton, Teishel Joefield, Reina Layug. Tameside and Glossop Integrated Care NHS Foundation Trust: Vinod Patel, Joanne Vere. Torbay and South Devon NHS Foundation Trust: Gareth Walker, Stacey Atkins, Jasmine Growdon, Charlotte McNeill. University Hospitals Birmingham NHS Foundation Trust: Rachel Cooney, Lillie Bennett, Louise Bowlas, Sharafaath Shariff. University Hospitals Bristol NHS Foundation Trust: Aileen Fraser, Katherine Belfield. University Hospitals of Derby and Burton NHS Foundation Trust: Said Din, Catherine Addleton, Marie Appleby, Johanna Brown, Kathleen Holding. University Hospitals of Leicester NHS Trust: John deCaestecker, Olivia Watchorn. University Hospitals Plymouth NHS Trust: Chris Hayward, Susan Inniss, Lucy Pritchard. University Hospital Southampton NHS Foundation Trust: Fraser Cummings, Clare Harris, Amy Jones, Liga Krauze, Sohail Rahmany, Audrey Torokwa. United Lincolnshire Hospitals NHS Trust: Jervoise Andreyev, Caroline Hayhurst, Carol Lockwood, Lynn Osborne, Amanda Roper, Karen Warner, Julia Hindle. University College London Hospitals NHS Foundation Trust: Shameer Mehta, James Bell, William Blad, Lisa Whitley. University Hospital Llandough: Durai Dhamaraj, Mark Baker. University Hospital of Wales (paediatric): Amar Wahid, Zoe Morrison. West Hertfordshire Hospitals NHS Trust: Rakesh Chaudhary, Melanie Claridge, Chiara Ellis, Cheryl Kemp, Ogwa Tobi. West Middlesex University Hospital: Emma Johnston. Western General Hospital: Metod Oblak, Richard Appleby. West Suffolk NHS Foundation Trust: Marium Asghar, Charlie Lees, Debbie Alexander, Kate Covil, Lauranne Derikx, Sryros Siakavellas, Helen Baxter, Scott Robertson. Withybush General Hospital: Kerrie Johns, Rachel Hughes, Janet Phipps, Abigail Taylor. Yeovil District Hospital NHS Foundation Trust: Katie Smith, Linda Howard, Dianne Wood. York Teaching Hospital NHS Foundation Trust: Ajay Muddu, Laura Barman, Janine Mallinson. Ysbyty Gwynedd: Iona Thomas, Kelly Andrews, Caroline Mulvaney Jones, Julia Roberts.
Contributors NAK, JRG, CB, SS, NP and TA participated in the conception and design of this study. CB was the project manager and coordinated patient recruitment. RN and TM coordinated all biochemical analyses and central laboratory aspects of the project. NAK, JRG, DC, SL, NC, JB, RC, NMC, ALH, PMI, KBK, CAL, JKL, JM, DPBM, SJM, CDM, KVP, RCGP, TR, RKR, CPS, PJS, JB, TJM, CWL, SS, NP and TA were involved in the acquisition, analysis or interpretation of data. Data analysis was done by NAK. Drafting of the manuscript was done by NAK, JRG, DC, SL, NC, TR, CWL, SS, NP, TA and SS and TA obtained the funding for the study. All the authors contributed to the critical review and final approval of the manuscript. NAK and TA have verified the underlying data.
Funding This study was funded by F. Hoffmann-La Roche, Hull University Teaching Hospital NHS Trust, Biogen GmbH (Switzerland), Celltrion Healthcare, Galapagos NV, Royal Devon and Exeter NHS Foundation Trust.
Competing interests NAK reports grants from F. Hoffmann-La Roche AG, grants from Biogen Inc, grants from Celltrion Healthcare, grants from Galapagos NV, non-financial support from Immundiagnostik, during the conduct of the study; grants and non-financial support from AbbVie, grants and personal fees from Celltrion, personal fees and non-financial support from Janssen, personal fees from Takeda, personal fees and non-financial support from Dr Falk, outside the submitted work. JRG reports grants from F. Hoffmann-La Roche AG, grants from Biogen Inc, grants from Celltrion Healthcare, grants from Galapagos NV, non-financial support from Immundiagnostik, during the conduct of the study. DC reports non-financial support from Ferring, personal fees and non-financial support from Pfizer, outside the submitted work. SL reports non-financial support from Pfizer, non-financial support from Ferring, outside the submitted work. RC reports personal fees from Takeda, outside the submitted work. NMC reports trial funding, advisory board and speaker fees paid to his institution from AbbVie, Eli Lilly, Takeda, Shire, Pfizer and Janssen. ALH reports personal fees from Abbvie, personal fees from Allergan, personal fees from BMS, personal fees from Celltrion, personal fees from Falk, personal fees from GSK, personal fees from Takeda, personal fees from Pfizer, personal fees from Janssen, personal fees from Galapogos, personal fees from Astra Zeneca, outside the submitted work. PMI reports grants and personal fees from Takeda, grants from MSD, grants and personal fees from Pfizer, personal fees from Galapagos, personal fees from Gilead, personal fees from Abbvie, personal fees from Janssen, personal fees from Boehringer Ingelheim, personal fees from Topivert, personal fees from VH2, personal fees from Celgene, personal fees from Arena, personal fees from Samsung Bioepis, personal fees from Sandoz, personal fees from Procise, personal fees from Prometheus, outside the submitted work. KBK reports personal fees from Janssen, personal fees from Takeda, personal fees from PredictImmune, personal fees from Amgen, outside the submitted work. CAL reports grants from Genentech, grants and personal fees from Janssen, grants and personal fees from Takeda, grants from AbbVie, personal fees from Ferring, grants from Eli Lilly, grants from Pfizer, grants from Roche, grants from UCB Biopharma, grants from Sanofi Aventis, grants from Biogen IDEC, grants from Orion OYJ, personal fees from Dr Falk Pharma, grants from AstraZeneca, outside the submitted work. JKL reports personal fees from MSD, personal fees from Janssen, grants and personal fees from Takeda, grants and personal fees from Galapagos, personal fees from Tillotts, outside the submitted work. JM reports grants and personal fees from Takeda Pharmaceuticals, grants and personal fees from Biogen, personal fees and non-financial support from AbbVie, personal fees from Grifols, personal fees from Sandoz, personal fees from Celltrion, personal fees and non-financial support from Janssen, personal fees from Vifor Pharmaceuticals, personal fees from Predictimmune, personal fees from Bristol Myers Squibb, non-financial support from Ferring Pharmaceuticals, outside the submitted work. DPBM reports grants from the Leona M. and Harry B. Helmsley Charitable Trust, during the conduct of the study; personal fees from Takeda Pharmaceuticals, personal fees from Pfizer, personal fees from Bridge Biotherapeutics, personal fees from Palatin Technologies, personal fees from Boehringer-Ingelheim, personal fees and other from Prometheus Biosciences, personal fees from Gilead, outside the submitted work. KVP reports personal fees and non-financial support from Takeda, personal fees and non-financial support from Janssen, personal fees and non-financial support from Abbvie, personal fees from DrFalk, non-financial support from Ferring, outside the submitted work. RCGP reports acting as consultant, advisory board member, speaker or recipient of educational grant from Dr Falk, Ferring, Janssen, Pharmacosmos and Takeda. TR reports grants and personal fees from Abbvie, personal fees from BMS, personal fees from Celgene, personal fees from Ferring, personal fees from Gilead, personal fees from GSK, personal fees from LabGenius, personal fees from Janssen, personal fees from Mylan, personal fees from MSD, personal fees from Novartis, personal fees from Pfizer, personal fees from Sandoz, personal fees from Takeda, personal fees from Galapagos, personal fees from Arena, outside the submitted work. RKR reports grants from NHS Research Scotland Senior Research Fellowship, personal fees from Nestlé, personal fees from AbbVie, personal fees from Dr Falk, personal fees from Takeda, personal fees from Napp, personal fees from Mead Johnson, personal fees from Nutricia, personal fees from 4D Pharma, outside the submitted work. CPS reports grants and personal fees from AbbVie, grants and personal fees from Janssen, grants and personal fees from Takeda, personal fees from Dr Falk, personal fees from Pfizer, personal fees from Galapagos, personal fees from Arena, personal fees from Fresenius Kabi, outside the submitted work. PJS reports speaker fees and advisory board sponsorship from Janssen, Celltrion and Takeda outside the submitted work. CWL reports personal fees from Abbvie, personal fees from Janssen, personal fees from Pfizer, personal fees from Takeda, grants from Gilead, personal fees from Gilead, personal fees from Galapagos, personal fees from Iterative Scopes, personal fees from Trellus Health, personal fees from Celltion, personal fees from Ferring, personal fees from BMS, during the conduct of the study. SS reports grants from Takeda, Abbvie, AMGEN, Tillots Pharma, personal fees from Jaansen, Takeda, Galapagos, Celltrion, Falk Pharma, Tillots pharma, Cellgene, Pfizer, Phamrmacocosmos, outside the submitted work. NP reports personal fees from Takeda, personal fees from Janssen, personal fees from Pfizer, personal fees from Bristol-Myers Squibb, personal fees from Abbvie, personal fees from Roche, personal fees from Lilly, personal fees from Allergan, personal fees from Celgene, outside the submitted work; and NP has served as a speaker/advisory board member for Abbvie, Allergan, Bristol Myers Squibb, Celgene, Falk, Ferring, Janssen, Pfizer, Tillotts, Takeda and Vifor Pharma. TA reports grants and non-financial support from F. Hoffmann-La Roche AG, grants from Biogen Inc, grants from Celltrion Healthcare, grants from Galapagos NV, non-financial support from Immundiagnostik, during the conduct of the study; personal fees from Biogen Inc, grants and personal fees from Celltrion Healthcare, personal fees and non-financial support from Immundiagnostik, personal fees from Takeda, personal fees from ARENA, personal fees from Gilead, personal fees from Adcock Ingram Healthcare, personal fees from Pfizer, personal fees from Genentech, non-financial support from Tillotts, outside the submitted work.
Patient and public involvement statement We conducted an electronic survey to gauge the opinion of patients with IBD on the patient questionnaires to be delivered as part of the CLARITY IBD study. We surveyed 250 patients across 74 hospitals. All our proposed questions for study inclusion were rated as important or very important by at least 83% of participants. The Exeter IBD Patient Panel refined the questions included in the study questionnaire, reviewed the study protocol, supported the writing of the patient information sheet, and participated in testing of electronic consent form and patient questionnaire. A member of the Exeter IBD Patient Panel sits on the study management committee, ensuring patient involvement in all aspects of study delivery, data analysis and dissemination of findings.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.