

Abstract
Objective. We evaluated the effect of sarilumab on patient-perceived impact of rheumatoid arthritis (RA) using the 7-domain RA Impact of Disease (RAID) scale.
Methods. Two phase III, randomized, controlled trials of sarilumab in patients with active, longstanding RA were analyzed: (1) sarilumab 150 mg and 200 mg every 2 weeks plus conventional synthetic disease-modifying antirheumatic drugs (+csDMARD) versus placebo + csDMARD [TARGET (NCT01709578)]; and (2) sarilumab 200 mg versus adalimumab (ADA) 40 mg monotherapy [MONARCH (NCT02332590)]. Least-squares mean (LSM) differences in RAID total score (range 0–10) and 7 key RA symptoms, including pain and fatigue (baseline to Weeks 12 and 24), were compared. “Responders” by RAID total score were defined by improvements from baseline ≥ minimal clinically important difference (MCID), and ≥ patient-acceptable symptom-state (PASS) at endpoint.
Results. Sarilumab 150 mg and 200 mg + csDMARD were nominally superior (p < 0.05) versus placebo + csDMARD and 200 mg sarilumab versus ADA 40 mg in LSM differences for RAID total score at weeks 12 (−0.93 and −1.13; −0.49, respectively) and 24 (−0.75 and −1.01; −0.78), and all effects of RA (except functional impairment in MONARCH Week 12). Effects were greater in physical domains (e.g., pain) than mental domains (e.g., emotional well-being). More patients receiving sarilumab versus placebo or ADA reported improvements ≥ MCID and PASS in total RAID scores at both assessments.
Conclusion. Based on the RAID, sarilumab + csDMARD or as monotherapy reduced the effect of RA on patients’ lives to a greater extent than placebo + csDMARD or ADA monotherapy. (ClinicalTrials.gov: NCT01709578 and NCT02332590)
- RHEUMATOID ARTHRITIS
- RHEUMATOID ARTHRITIS IMPACT OF DISEASE SCALE
- DISEASE-MODIFYING ANTIRHEUMATIC DRUGS
Patients with rheumatoid arthritis (RA) experience a variety of signs and symptoms, and report significant physical and psychological effects with this condition1,2,3. Quantifying key clinical symptoms and effects of RA from the patient perspective, in addition to evaluating clinical markers, is therefore vital to comprehensively understand the disease and evaluate treatment, in accord with current international consensuses and guidelines4,5,6,7.
The patient perspective can be systematically collected through administration of patient-reported outcomes (PRO). In addition to physician-reported and laboratory data, use of well-defined and reliable PRO is essential for drawing comprehensive conclusions for RA treatment outcomes. The RA Impact of Disease (RAID) scale is an internationally validated, composite PRO measure specifically designed for use in RA8,9,10,11,12. RAID evaluates 7 domains, each containing a single item, including 2 key symptoms (severity of pain and fatigue), and 5 primary impacts (coping, emotional and physical well-being, functional impairment, and sleep). It also provides additional information for assessment of RA, such as coping and emotional well-being, compared with the traditionally evaluated PRO of patient global assessment of disease activity, pain, and physical functioning8,13,14,15.
Sarilumab is a recently approved human monoclonal antibody directed against both soluble and membrane-bound interleukin 6 receptor-α (anti-IL-6Rα). The RAID scale was administered to patients in 2 phase III randomized controlled trials (RCT) of sarilumab: TARGET (NCT01709578)16 and MONARCH (NCT02332590)17. Change from baseline in the RAID score was a secondary endpoint in both the TARGET and MONARCH RCT.
TARGET compared the efficacy and safety of subcutaneous (SC) sarilumab 150 mg and 200 mg every 2 weeks (q2w) versus placebo plus conventional synthetic disease-modifying antirheumatic drugs (csDMARD) in patients with moderate to severely active RA who were intolerant of or had an inadequate response to ≥ 1 tumor necrosis factor inhibitor (TNF-IR)16. The co-primary endpoints in TARGET were the proportion of patients achieving American College of Rheumatology ≥ 20% (ACR20) responses7 at Week 24, and change from baseline in physical function assessed by the Health Assessment Questionnaire-Disability Index (HAQ-DI)18 at Week 12.
MONARCH compared the efficacy and safety of sarilumab SC 200 mg q2w monotherapy versus adalimumab (ADA) SC 40 mg q2w monotherapy in patients with active RA who discontinued treatment with methotrexate (MTX)17. The primary efficacy endpoint in MONARCH was change from baseline in the 28-joint Disease Activity Score using erythrocyte sedimentation rate at Week 24. In both these RCT, sarilumab showed superiority over placebo or ADA in reducing signs and symptoms of RA and improving physical function, and its safety profile was consistent with IL-6R blockade16.
The RAID is recognized by researchers, patients, and organizations such as the European League Against Rheumatism (EULAR)19 and OMERACT20 as a promising instrument, because it was developed with patient input and addresses all the key issues for patients with RA. However, as a relatively new scale, the RAID has to date been applied in few clinical trials15,21 other than TARGET16 and MONARCH17, with publications for these trials describing only high-level data on the RAID.
Our report contributes to further validating the RAID score. Our objective was to assess the effects of sarilumab treatment in combination with csDMARD or as monotherapy on the patient-reported impact of RA using the RAID scale.
MATERIALS AND METHODS
Data were collected from 2 phase III RCT of sarilumab, TARGET and MONARCH, as described16,17. Both trials enrolled adult patients fulfilling the 2010 ACR/EULAR classification criteria for RA22. In TARGET, TNF-IR patients with moderate to severely active RA were included if disease duration was ≥ 6 months. Patients with uncontrolled concomitant diseases, significant extraarticular manifestations of RA, functional class IV RA, other inflammatory diseases, or current/recurrent infections or those receiving prednisone were excluded.
In MONARCH, patients with moderate to severely active RA with ACR class I–III functional status23 were enrolled if they had disease duration ≥ 3 months, and no prior use of biologic DMARD. Eligible patients were randomized to sarilumab SC 200 mg plus placebo q2w or ADA SC 40 mg plus placebo q2w for 24 weeks. After 16 weeks, patients who did not achieve ≥ 20% improvement in tender and swollen joint counts in the sarilumab group were switched to once-weekly ADA or matching placebo17.
RAID scale
The RAID scale consists of 7 single-item domains, each rated by patients on an 11-point numerical rating scale from 0 (best) to 10 (worst)8. There are 2 symptom domains, pain and fatigue, and 5 impact domains, consisting of functional impairment, emotional well-being, physical well-being, quality of sleep, and ability to cope. The domains can be reported separately14 and as a total score, which is a continuous variable ranging from 0 (best) to 10 (worst); lower scores are indicative of less impact of disease. In the total RAID score, each domain is given a specific weight reflecting its importance to patients (e.g., more given to pain, fatigue, and functional impairment). Weights were obtained from international studies, as follows: pain 0.21; functional disability 0.16; fatigue 0.15; and sleep problems, emotional well-being, physical well-being, and coping all 0.128,10. The RAID scale has been psychometrically validated at an international level8,10,12,24.
Statistical analyses
Least-squares mean (LSM) differences from baseline in total RAID and domain scores were analyzed with a mixed model for repeated measures, including treatment, region, visit, and treatment-by-visit interaction (and number of prior TNF inhibitors in TARGET) as fixed effects and baseline as a covariate.
Posthoc analyses were conducted to identify responders in the total RAID score. Three “responder” definitions were used. Two were based on an established minimal clinically important difference (MCID) from baseline. This was previously defined by different techniques using data from 108 patients receiving TNF inhibitor treatment for active RA, who were evaluated at screening and baseline, then after 4 and 12 weeks of treatment11. The reliability of the overall RAID score, and various possible improvement thresholds proposed in the rheumatology scientific literature [e.g., improvements of at least 1, 2, or 3 points in total RAID score (total range 0–10 points), and relative changes ≥ 20%, 30%, and 50% from baseline]24,25 were evaluated. The reliability of the RAID score between screening and baseline was found to be high [intraclass correlation coefficient of 0.85 (95% CI 0.79–0.90)], with smallest detectable difference of 1.8 and smallest detectable change of 1.3. The 2 optimal MCID thresholds were identified as a 3-point reduction in total RAID score from baseline, or a relative improvement of 50% in total RAID score. A patient was defined as a responder if they reported improvements from baseline ≥ MCID. A third responder definition was based on a patient acceptable symptom state (PASS), defined as a score ≤ 311. Patients who discontinued therapy or required rescue medication prior to achieving responder endpoints were classified as nonresponders26,27,28,29.
In TARGET, RAID was positioned after the break in the hierarchy used to control for multiple testing, and therefore statistical significance cannot be determined; other analyses were conducted posthoc. In MONARCH, RAID was not included in the hierarchy. Thus, to aid interpretation, statistical comparisons between treatment groups (to test for nominal significance) were supplemented by between-group effect size analyses (standardized mean differences) using Cohen’s d Rule for Change Interpretation, as follows: important: d ≤ −0.8; moderate: −0.8 < d ≤ −0.5; and small: −0.5 < d ≤ −0.230.
RAID scores were separately evaluated in each trial at baseline and at Week 12 and Week 24. For missing data at the item level, an imputation using the mean of the 6 other items was used.
Analyses in this study were conducted on data from 2 previous RCT of sarilumab, TARGET (NCT01709578) and MONARCH (NCT02332590)16,17. The protocols for both these studies were approved by the appropriate ethics committees/institutional review boards, and each patient provided written informed consent before participation in the studies. The studies were conducted in compliance with the International Conference on Harmonization Guidelines for Good Clinical Practice and the Declaration of Helsinki16,17.
RESULTS
Overall, 546 patients from TARGET and 369 from MONARCH were included in the analysis (Table 1). Between-group baseline demographics were generally comparable within each study; however, in MONARCH, disease duration was longer in the sarilumab group versus the ADA group [mean 8.1 yrs (SD 8.1) vs mean 6.6 yrs (SD 7.8), respectively]. Between studies, mean disease duration in MONARCH was shorter than in TARGET (mean 7.3 yrs vs mean 12.1 yrs). Baseline RAID scores were generally comparable across all groups within the individual RCT, ranging from a mean of 6.5 (SD 2.0) to 6.8 (SD 1.8) in TARGET31 and 6.4 (SD 2.0) to 6.7 (SD 1.7) in MONARCH17 (Table 1). All other demographics, including age, sex, and race, were relatively comparable among the patients in the 2 studies.
Patient demographics and disease characteristics.
Changes in RAID score from baseline
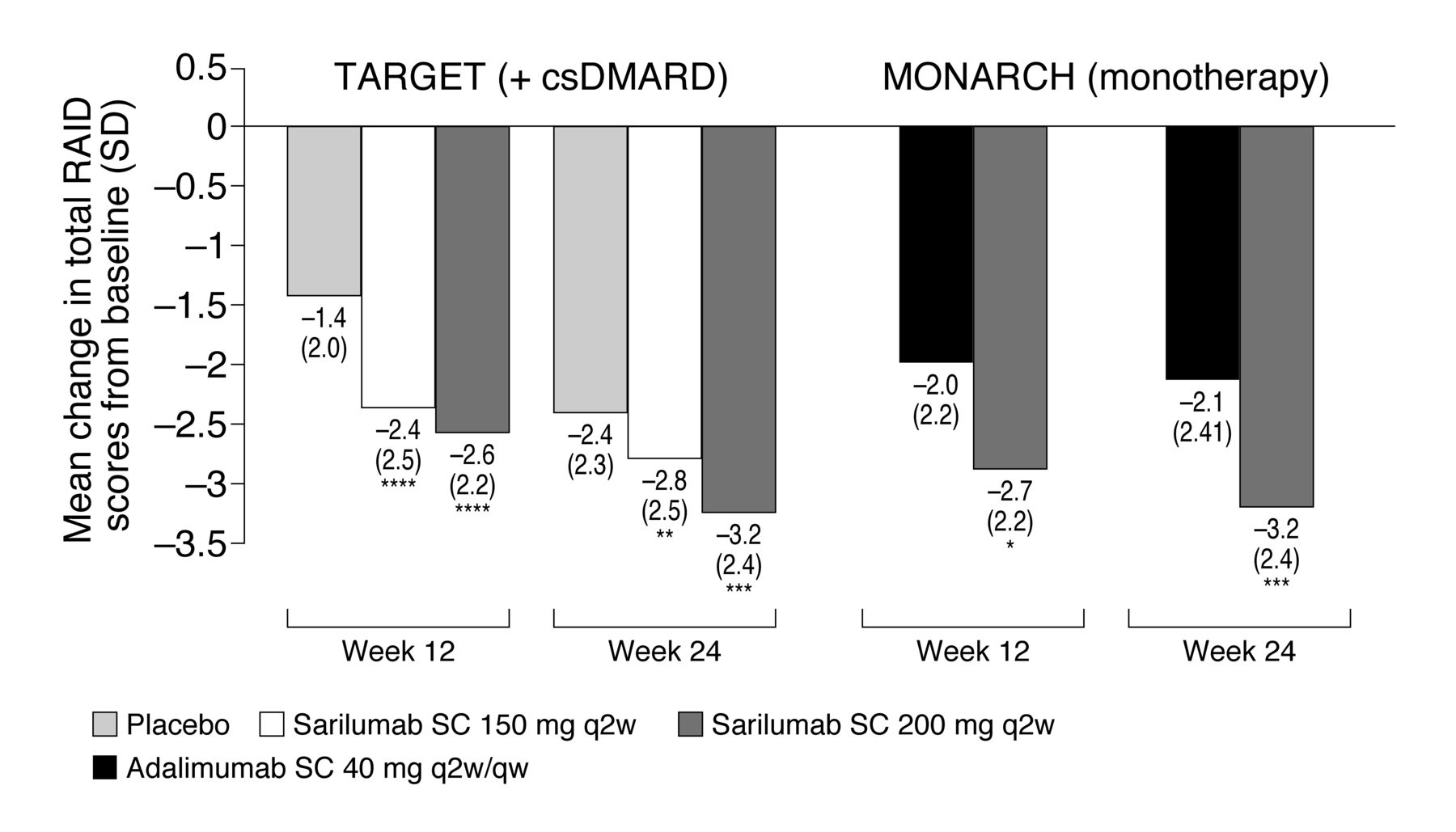
LSM differences in RAID total scores were greater with sarilumab compared to placebo in the TARGET study at Week 12 (−0.93 and −1.13, respectively, for sarilumab 150 mg and 200 mg vs placebo; nominal p < 0.0001) and Week 24 (−0.75 and −1.01, respectively, for sarilumab 150 mg and 200 mg vs placebo; nominal p < 0.01). LSM differences in RAID total score were also greater with sarilumab versus ADA in MONARCH at Week 12 (−0.49 for sarilumab 200 mg vs ADA; nominal p < 0.05) and Week 24 (−0.78 for sarilumab 200 mg vs ADA; nominal p < 0.001; Figure 1). Between-group effect sizes for RAID total scores (Figure 2) met thresholds for small to moderate levels of importance by Cohen’s d Rule for Change Interpretation in both sarilumab dose groups versus placebo at Weeks 12 and 24 (TARGET), and in the sarilumab 200 mg group versus ADA at Week 24 (MONARCH)30.

Mean change in total Rheumatoid Arthritis Impact of Disease (RAID) scores from baseline in TARGET (+ csDMARD) and MONARCH (monotherapy). * Nominal p ≤ 0.05; ** nominal p ≤ 0.01; *** nominal p ≤ 0.001; **** nominal p ≤ 0.0001 all versus placebo (TARGET) or adalimumab (MONARCH). csDMARD: conventional synthetic disease-modifying antirheumatic drug; qw: once weekly; q2w: every 2 weeks; SC: subcutaneous.

Between-group effect sizes on Rheumatoid Arthritis Impact of Disease total score, sarilumab 150 mg or 200 mg versus placebo (TARGET: + csDMARD) or adalimumab (MONARCH: monotherapy). Cohen’s d Rule for Change Interpretation: important: d ≤ −0.8; moderate: −0.8 < d ≤ −0.5; and small: −0.5 < d ≤ −0.225. * Nominal p ≤ 0.05; ** nominal p ≤ 0.01; versus placebo (TARGET) or adalimumab (MONARCH) for the difference between groups in the least-squares mean change from baseline. csDMARD: conventional synthetic disease-modifying antirheumatic drug; qw: once weekly; q2w: every 2 weeks; SC: subcutaneous.
Domain scores
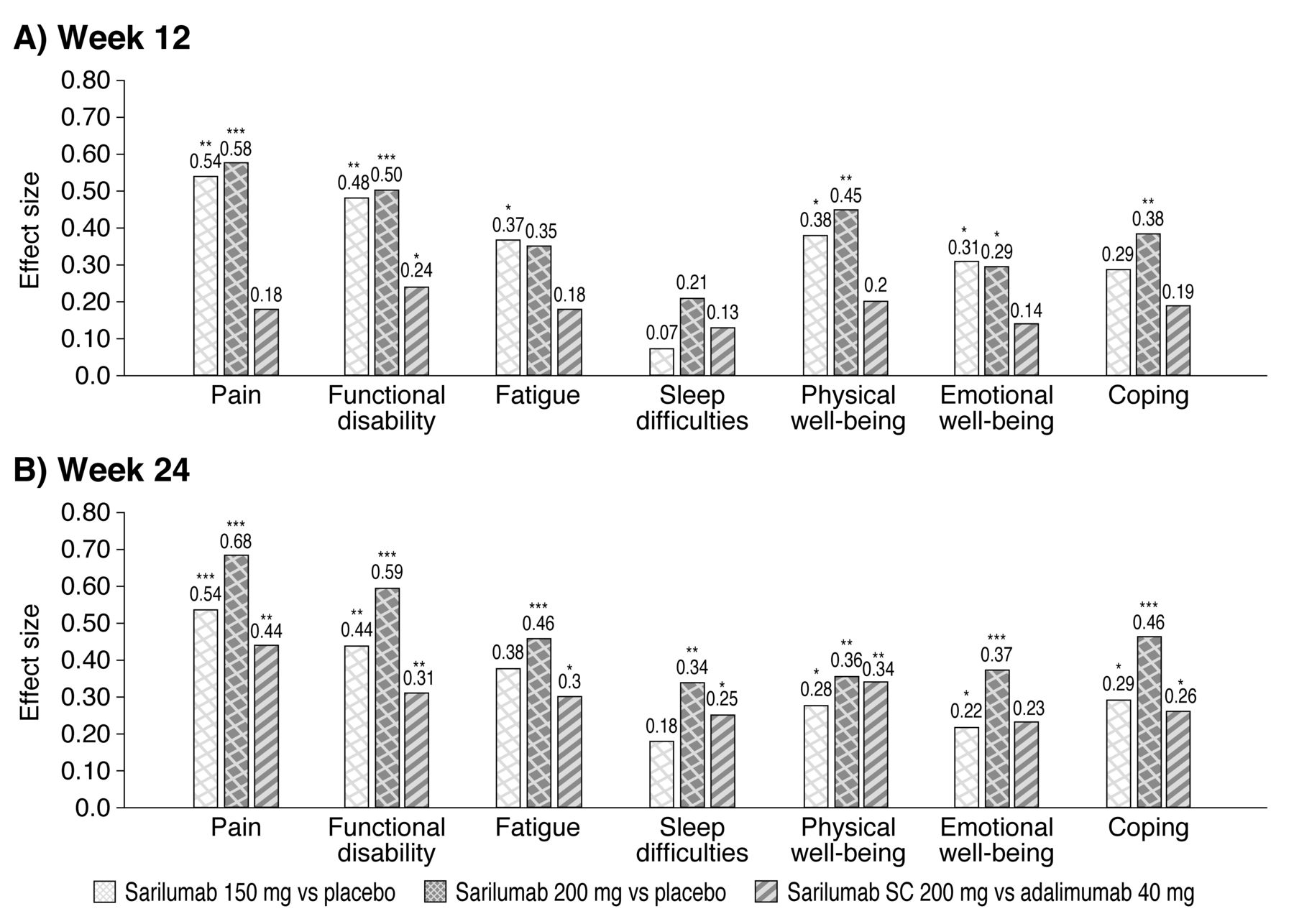
Changes from baseline in individual domain scores were significantly greater with sarilumab compared to placebo for differences between groups (all nominal p < 0.05 except sleep domain; Figure 3). In MONARCH, sarilumab treatment showed greater improvement compared with ADA only in the functional impairment domain at Week 12, and in all domains by Week 24. Moderate benefits were reported in the pain domain at Week 12 (effect sizes of 0.54 and 0.58 for sarilumab 150 mg and 200 mg, respectively, vs placebo) and at Week 24 in TARGET (effect sizes of 0.54 and 0.68 for sarilumab 150 mg and 200 mg vs placebo; all nominal p < 0.05). In addition, most other domains (other than sleep) met thresholds for small importance at Week 24 in both studies30.
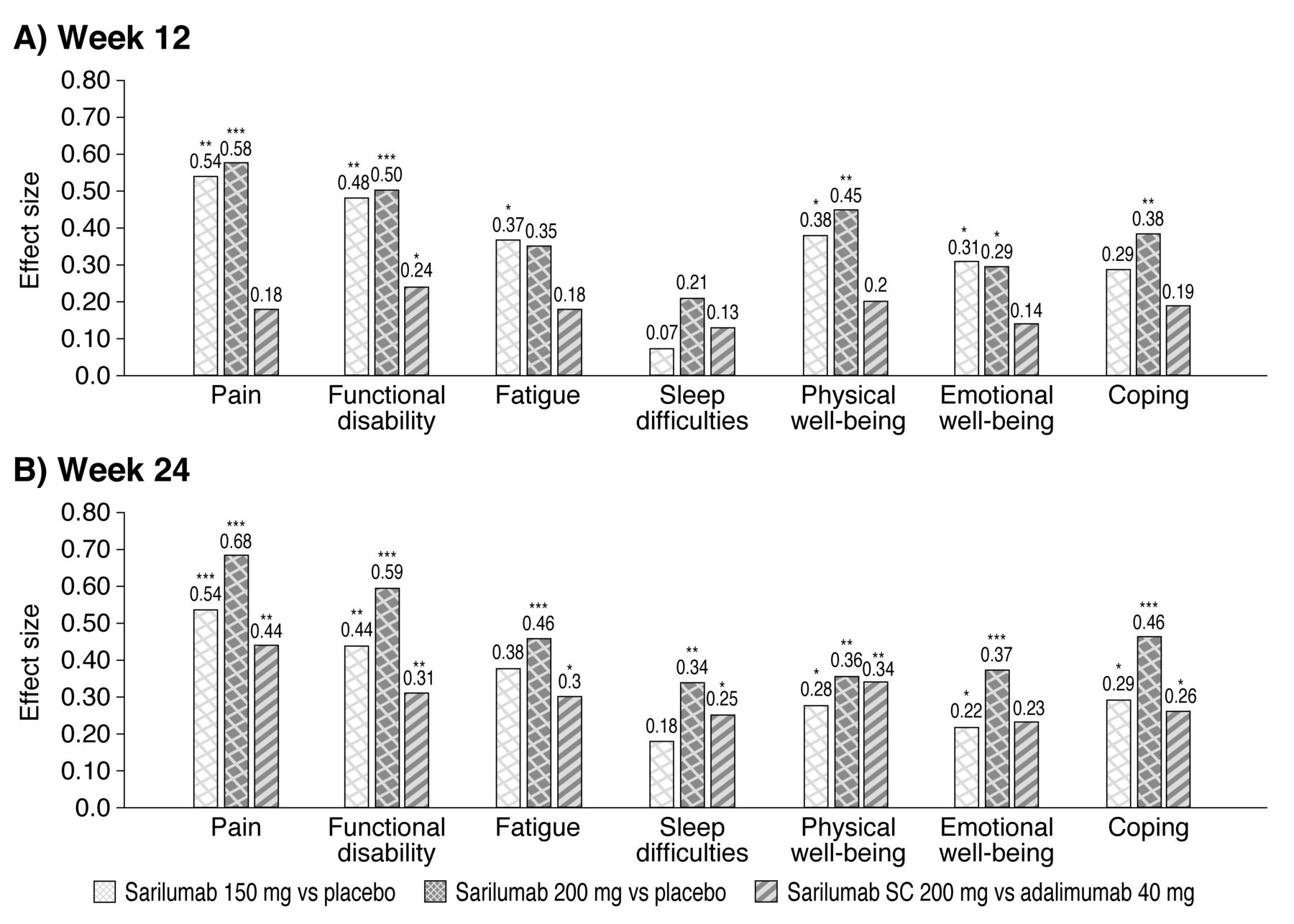
Between-group effect sizes on Rheumatoid Arthritis Impact of Disease domain scores in TARGET, sarilumab 150 mg + csDMARD or 200 mg + csDMARD versus placebo; and in MONARCH, monotherapy with sarilumab 200 mg versus adalimumab 40 mg: (A) Week 12, (B) Week 24. Cohen’s d Rule for Change Interpretation: important: d ≤ −0.8; moderate: −0.8 < d ≤ −0.5; and small: −0.5 < d ≤ −0.225. * Nominal p ≤ 0.05; ** nominal p ≤ 0.01; *** nominal p ≤ 0.001; all versus placebo for the difference between groups in the least-squares mean change from baseline. csDMARD: conventional synthetic disease-modifying antirheumatic drug; SC: subcutaneous.
Responder analyses, MCID ≥ 3
In TARGET, greater proportions of patients in the sarilumab 150 mg and 200 mg groups versus placebo were responders defined by an MCID ≥ 3 (nominal p ≤ 0.0001 at Week 12 for both doses; nominal p ≤ 0.01 and nominal p ≤ 0.0001 for sarilumab 150 mg and 200 mg, respectively, at Week 24; Figure 4A). In MONARCH, a greater proportion of the sarilumab 200 mg group versus ADA were responders (nominal p ≤ 0.01 at both Weeks 12 and 24; Figure 4A).

Proportion of patients in TARGET (+ csDMARD) and MONARCH (monotherapy) who (A and B) reported improvements in RAID scores ≥ MCID; or (C) reached a patient-acceptable symptom-state of 3 or lower. * Nominal p ≤ 0.05; ** nominal p ≤ 0.01; *** nominal p ≤ 0.001; **** nominal p ≤ 0.0001, all versus placebo (TARGET) or adalimumab (MONARCH). csDMARD: conventional synthetic disease-modifying antirheumatic drug; MCID: minimal clinically important differences; qw: once weekly; q2w: every 2 weeks; RAID: Rheumatoid Arthritis Impact of Disease; SC: subcutaneous.
MCID ≥ 50%
There were greater proportions of responders in both sarilumab dose groups in TARGET than in the placebo group (nominal p ≤ 0.001 at Week 12; nominal p ≤ 0.01 and nominal p ≤ 0.001 for sarilumab 150 mg and 200 mg, respectively, at Week 24). In MONARCH, greater improvement with sarilumab 200 mg versus ADA was reported at Week 24 (nominal p ≤ 0.05; Figure 4B).
PASS
Absolute total RAID scores ≤ 3 were reported by both sarilumab dose groups versus the placebo group in TARGET at Week 12 (sarilumab 150 mg, nominal p ≤ 0.01; sarilumab 200 mg, nominal p ≤ 0.001) and Week 24 (sarilumab 200 mg, nominal p ≤ 0.05; sarilumab 200 mg, nominal p ≤ 0.001). In MONARCH at Week 24, a greater proportion of patients receiving sarilumab 200 mg than ADA were defined as responders (nominal p ≤ 0.01; Figure 4C).
DISCUSSION
The benefits of sarilumab treatment as combination therapy with csDMARD or as monotherapy across a range of PRO have been reported in MTX-IR and TNF-IR populations, including patient global assessment of disease activity, pain, physical function, fatigue, and general health status. Based on the patient-reported RAID scale, data collected in the TARGET and MONARCH RCT indicate that sarilumab 150 mg or 200 mg q2w given as combination therapy with a csDMARD or as 200 mg monotherapy reduced the effects of RA on patients’ lives to a greater extent than placebo plus csDMARD or ADA SC 40 mg q2w or once weekly monotherapy. Mean baseline scores ranged from 6.4 to 6.8, indicating a high impact of disease in these trial populations. In both the TARGET and MONARCH RCT, the benefits of sarilumab treatment on symptoms and impact of disease were clinically meaningful when assessed by 2 definitions of MCID and by PASS, with differential effects compared with placebo or ADA across the majority of RAID domains (with the exception of sleep for sarilumab vs placebo in the TARGET study), with marked improvements in RAID total scores and domains of pain and functional impairment across all sarilumab treatment groups.
The relatively new RAID scale has to date been applied in only 1 other clinical trial15, a smaller, open-label, single-arm study of etanercept (ETN) 50 mg/wk. In that study, 56% of 120 patients with active RA reported total RAID scores ≤ 3.0 at Week 12, indicating reduced disease impact from baseline15. In comparison, patients in TARGET and MONARCH had longer disease duration and higher baseline RAID scores than in the ETN study15,16,17.
In these 2 larger RCT, 35% of sarilumab-treated patients in TARGET at Week 12 and 36% at Week 24 reported RAID scores ≤ 3; and in MONARCH it was 41% at Week 24.
Newer PRO measures such as the RAID scale are revealing the additional importance of evaluating multi-dimensional patient outcomes with content and construct validity, responsiveness, and precision. It is now widely recognized that PRO should reveal what is important for patients, and that they should be developed with patient input32,33. RAID was developed by a EULAR international task force of clinicians and patients to provide a single instrument that integrates all relevant patient domains, with relevance in different disease states, countries, and cultures, and it was designed to better quantify the experience of living with RA. Several studies have shown that the domains assessed in RAID are applicable and important for patients8,10,12,25,34. The advantage of sarilumab treatment over ADA and placebo for improving RAID domains in these trials offers important information for physicians to consider in the context of shared treatment decision making35.
Pain, fatigue, sleep disturbance, and ability to cope are all symptoms that are of importance to patients with RA, but not all (e.g., sleep and ability to cope) are routinely assessed in RA RCT, or even in clinical practice36. RAID is unique in that it not only assesses patient-reported symptoms such as pain, but also fatigue, sleep disturbance, and coping. Fatigue, frequently reported in RA, can severely affect all aspects of health-related quality of life (HRQOL), with a multifactorial origin, not just inflammation but personal factors and psychological distress as well37.
In this analysis, we noted some differences in responses to treatment: sleep and coping were less responsive than other domains, suggesting these may be less amenable to short-term treatment effects of DMARD and biologics than, for example, pain. It appears that sleep and coping, in particular, are less accessible to biologic treatment than other patient-reported domains of impact. This raises the question of whether these aspects of HRQOL are less directly linked to the inflammatory process than, for example, pain14. This is consistent with findings from other RCT of DMARD with other mechanisms of action, in which sleep responsiveness in particular has been reported as less than other PRO14,38.
Our findings must be considered in light of some study limitations. While the RAID data were included in the statistical hierarchy in MONARCH and TARGET, results were considered after the break in the hierarchy; therefore, p values were not controlled for multiplicity, and are nominal. Hence, we applied multiple approaches to assess the clinical relevance of the observed results, including Cohen’s d, responder analysis using 2 different MCID definitions, and PASS. All the approaches consistently indicated clinically meaningful improvements across the RAID domains. Further investigation of the relationships of the endpoints with RAID, and any added value of RAID within the context of a clinical trial, is warranted for a separate study. Nonetheless, despite the relative novelty of the RAID scale, a range of tests support our interpretation of the present results. In addition, because ADA is usually used as combination therapy, the added value of our findings should not be seen as a comparison with ADA only, but also as further validating a recent outcome measure, the RAID.
While the extreme burden on patients with RA caused by their joint damage is widely recognized39,40,41, other manifestations of this systemic disease including multiple comorbidities and psychosocial outcomes continue to be revealed42,43. Hence, in addition to the clinical markers of disease activity that are unequivocally necessary for informing treatment decisions in RA, assessing improvement on PRO including HRQOL reveals the ultimate benefit of treatment in reducing patient burden39,40,44. The objective of the RAID scale is to provide a comprehensive assessment of the effects of treatment on patient burden, and from their perspective.
As a relatively new measure, RAID has yet to be widely applied in either RA RCT or clinical practice settings. Although its use is increasing, its inclusion in large prospective studies will provide more evidence of its sensitivity8 and assessment of acceptable levels of missing data and MCID/PASS definitions, while data from clinical practice settings in diverse patient populations will indicate its generalizability.
Our analyses indicate that the RAID scale efficiently evaluated the benefits of sarilumab treatment on patient-reported effects of RA in both the TARGET and the MONARCH RCT.
Acknowledgment
The authors thank the patients, their families, and all investigators involved in the sarilumab studies.
Footnotes
Full Release Article. For details see Reprints and Permissions at jrheum.org
Supported by Sanofi and Regeneron Pharmaceuticals Inc., which developed sarilumab. L. Gossec has acted as a consultant for Sanofi. V. Strand has acted as a consultant for Regeneron Pharmaceuticals Inc. and Sanofi. C. Proudfoot is a former employee of and current shareholder in Sanofi and current employee and shareholder of Novartis. C. Chen, T. Kimura, and E. Mangan are employees of and shareholders in Regeneron Pharmaceuticals Inc. E. Mangan is also a shareholder in Pfizer. S. Guillonneau and H. van Hoogstraten are employees of and hold shares or options in Sanofi.
- Accepted for publication February 6, 2019.
Free online via JRheum Full Release option








{kind=link}
{kind=link}
{kind=link}
{kind=link}