

Abstract
Objective. To investigate muscle impairment (isometric and dynamic) and disease activity during the first year after diagnosis of polymyositis (PM) and dermatomyositis (DM), and to study the relationship between muscle impairment, patient-reported health, and disease activity.
Methods. Seventy-two patients enrolled in the Swedish Myositis Register, 2003–2010, were followed prospectively. The Manual Muscle test (MMT-8; isometric muscle strength), the Functional Index of myositis test (FI-2; dynamic, repetitive muscle function), and disease activity (6-item core set) were retrieved at the time of diagnosis, and after 6 and 12 months. Self-reported health (Medical Outcomes Study Short Form-36; SF-36) was retrieved at 12 months.
Results. At the time of diagnosis, median (Q1–Q3) for the FI-2 was 27.2% (7.9–60.5%) of maximal score compared to 93.8% (92.5–98.8%) of maximal MMT-8. At 12 months, the FI-2 and the MMT-8 improved to 29.4% (16.5–60.7%; p < 0.05) and 96.1% (88.1–99.4%), respectively (p < 0.01). At 12 months, 45% of patients improved ≥ 20%, and 27% worsened ≥ 20% in FI-2 score, while 10% improved ≥ 20% in MMT-8. Physician’s global visual analog scale (VAS), Health Assessment Questionnaire, and creatine phosphokinase levels improved significantly at 12 months (p < 0.05–0.001) while patient’s global and extramuscular VAS remained unchanged. The SF-36 physical function correlated strongly with the FI-2 (rs = 0.74; CI 0.55–0.85) and moderately with the MMT (rs = 0.54; CI 0.27–0.73), with lower correlations between muscle function and other SF-36 domains.
Conclusion. Patients with PM/DM were characterized by impaired dynamic repetitive muscle function (DRMF) that correlated well with patient-reported physical function. Assessment of DRMF adds information regarding muscle impairment in these patients.
Adult dermatomyositis (DM) and polymyositis (PM) are rare chronic inflammatory autoimmune diseases primarily affecting skeletal muscle1, and a majority of patients also develop lung fibrosis2. Muscle impairment mainly affects proximal muscles, with hip flexors being the most affected muscle group overall3; however, patients also have reduced grip strength4. Medical treatment is based on high-dose glucocorticoids in combination with immunosuppressive drugs1. Although most patients respond favorably to this medical treatment, the majority develop sustained disability4,5,6,7,8. Exercise has become a valuable complement to medical treatment to improve muscle function and perceived health9,10 as well as muscle health11.
Standardized and validated outcome measures including measures of muscle impairment are important in clinical practice to adjust treatment as well as in clinical trials. The Medical Research Council (MRC) scale and different versions of the Manual Muscle Test (MMT) have been widely used in adults and children with IIM12. The International Myositis Assessment Clinical Study group (IMACS), on the basis of a consensual process, has proposed that the MMT-813, which assesses isometric muscle strength in 8 muscle groups, should be included in the 6-item core set of measures of disease activity used in myositis clinical trials. This 6-item core set also includes a physician’s/patient’s global assessment of disease activity visual analog scale (VAS), the Health Assessment Questionnaire (HAQ), extramuscular assessments, and analysis of muscle enzymes14,15. Clinical experience and a few publications suggest that patients with PM and DM have reduced muscle endurance relative to healthy individuals16,17. No study has evaluated the differences in assessed isometric muscle strength using the MMT-8, or dynamic repetitive muscle function (DRMF; as a proxy for muscle endurance) tested by the Functional Index of myositis (FI)-218, or how DRMF develops over time or responds to treatment in men and women with recent-onset PM or DM. Further, the relationships between muscle function and perceived health and clinical disease activity have not been assessed in prospective fashion for the early disease stage.
The purpose of our study was to investigate muscle impairment in relation to isometric muscle strength and DRMF as assessed by 2 commonly used instruments in men and women with recent-onset PM and DM, and to evaluate muscle impairment and disease activity during the first year following PM or DM diagnosis. A further aim was to investigate the relationship between muscle impairment and patient-reported health and between muscle impairment and disease activity.
MATERIALS AND METHODS
Patients
Patients were eligible for the study who were diagnosed with definite or probable PM or DM19,20 during 2003–2010 and who were registered in the national Swedish Myositis Network (SweMyoNet) register at the rheumatology clinic at Karolinska University Hospital. Inclusion criteria were being enrolled in the SweMyoNet register, and having performed both the MMT-8 and the FI-2 at the time of diagnosis. Exclusion criteria were the diagnosis of inclusion body myositis or a second diagnosis of rheumatoid arthritis, systemic lupus erythematosus, or systemic sclerosis. Ninety-two patients were identified, of whom 72 fulfilled the criteria and were included in the study. Twenty patients were excluded, 11 because they did not perform both the MMT and the FI-2 at the time of diagnosis and 9 because they had a secondary rheumatic diagnosis. Demographic data are presented in Table 1. All patients were treated with conventional immunosuppressive drugs according to the decision of the treating physician. Generally, they were treated with prednisolone (PSL) in combination with methotrexate or azathioprine. In addition, patients were given an easy to moderate home exercise program to follow during the first 12 weeks and thereafter were encouraged to exercise regularly. Data for myositis-specific autoantibodies were available for 64 patients, tested using RNA immunoprecipitation for antisynthetase antibodies, anti-SRP (signal recognition particle), anti-U1RNP, and anti-SS-A/Ro, and by protein immunoprecipitation for anti-MDA5 (melanoma differentiation-associated protein 5), anti-Mi-2 (nucleosome-remodeling deacetylase complex), anti-TIF1g (transcription inhibitory factor–1g), anti-PM-Scl, and anti-Ku (peltz factor).
Demographic data at diagnosis and at 6- and 12-month followup.
Assessments
Patients were followed by a standardized protocol at the rheumatology myositis clinic at Karolinska University Hospital since 2003. Assessments were performed at the time of diagnosis and before the introduction of immunosuppressive treatment, and again after 6 months and 12 months. The variables are registered in the SweMyoNet register. The self-reported Medical Outcomes Study Short Form-36 (SF-36) data were gathered after 12 months of treatment. The standardized protocol includes the 6-item disease activity core set, including MMT-8, determined by the IMACS14,21 and the FI-218.
The MMT-8 muscle group test was performed on the dominant body side. The MMT-8 includes neck flexors, deltoids, biceps brachii, dorsi flexors of the wrist, gluteus maximus and medius, quadriceps, and dorsi flexors of the ankle. The total score varies between 0 and 80, where 80 indicates normal isometric muscular strength12.
The FI-2 is a disease-specific, valid, and reliable instrument that assesses DRMF in 7 muscle groups: shoulder flexion, shoulder abduction, neck flexion, hip flexion, knee extension (maximal no. repetitions = 60), and dorsal flexors and plantar flexors (maximal no. repetitions = 120)18. Each muscle group is scored as the number of correctly executed repetitions.
To measure disease activity, the 6-item core set according to IMACS was used, as contained in the Myositis Disease Activity Assessment Tool21. This comprises both the physician’s and patient’s global assessment of disease activity (VAS), the MMT-8, the HAQ, muscle enzymes (creatine phosphokinase, CK), as well as extramuscular disease activity on VAS (0–10).
The SF-36, as recommended by IMACS to assess self-reported perceived health, contains 8 domains: Physical Function, Role-Physical, Bodily Pain, General Health, Vitality, Social Function, Role-Emotional, and Mental Health, all scored from 0–100 (100 = good health)22.
Procedures
The FI-2 was assessed by any of 3 well-trained physical therapists. The disease activity assessments including the MMT-8 were performed by any of 3 rheumatology specialists. The SF-36 was distributed by a registered nurse and then entered into the SweMyoNet. The SF-36 data from the 12-month examination following diagnosis were retrieved from the SweMyoNet to investigate the association between the objectively observed muscle impairments and patient-reported health. In most cases, the FI-2 was assessed about 1 week prior to the MMT-8.
Data were retrieved from the SweMyoNet and validated according to each patient’s medical records, and missing data were completed where possible.
Statistical analyses
The FI-2 produces ratio data; however, because this is not normally distributed, all data are presented in median values and quartiles. To enable a comparison between the scores from the FI-2 and the MMT-8, data are presented as percentages of total score. To analyze the difference in MMT-8 and FI-2 and the VAS physician/patient and the VAS extramuscular after 6 and 12 months followup compared to baseline, the Friedman’s ANOVA was used, with the Wilcoxon signed-rank test as the after-test. The Mann-Whitney U unpaired test was used to compare muscle function between sexes and against diagnosis. The level of significance was set to p < 0.05. Data are also presented as the number of responders in DRMF and muscle strength, where responders are defined as those who have improved ≥ 20% (relative percentage change) in either the MMT-8 or the FI-223. In our study, a change of ≥ 20% was considered clinically relevant. Absolute percentage change was also analyzed for MMT-8 and FI-2. Number of patients with a PSL dose of 10 mg/day or less at 12 months, regardless of baseline dose, was used as a measure of response in disease activity. The Spearman correlation coefficient was used to analyze the relationships between muscle impairment and disease activity, including PSL dose response, and between muscle impairment and patient-reported quality of life, as well as between percent response of the FI-2 and the MMT. Correlation coefficients between 0 and 0.25 were considered no or very low correlation, coefficients between 0.26 and 0.40 were considered low correlation, coefficients between 0.41 and 0.69 were considered moderate, coefficients between 0.70 and 0.89 as high, and coefficients between 0.90 and 1.00 as very high24. Analysis and figures were done in Statistica 12 and SPSS.
Ethical scrutiny
The use of the SweMyoNet was approved by the Regional Ethical Committee in Stockholm (2008/1457-31 and 2012/736-32), and patients signed informed consent for their registry data to be used in research.
RESULTS
Muscle function at the time of diagnosis
Patients had 27.2% (7.9–60.5) of maximal score in the FI-2 as compared to a MMT-8 total score of 93.8% (92.5–98.8); these scores were independent of sex or diagnosis of PM or DM (Table 2).
Muscle impairment at time of diagnosis and at 6- and 12-month followup.
Muscle function after 6 and 12 months of treatment
The whole group worsened in their FI-2 score at 6 months compared to their scores at time of diagnosis (p < 0.05; n = 51), but they had improved at 12 months relative to their score at the time of diagnosis (p < 0.05; Table 2). Men with PM and DM improved in their FI-2 score at both 6 and 12 months relative to their score at time of diagnosis (p < 0.05; n = 49) while women remained unchanged.
The whole group improved in their MMT-8 score at 6 and 12 months (p < 0.01). The men already had 98.8% of maximal score at the time of diagnosis and had not improved at the followup assessments. There were no differences in either MMT-8 or FI-2 scores between patients with PM and DM at any measurement point.
Responders and nonresponders in muscle function
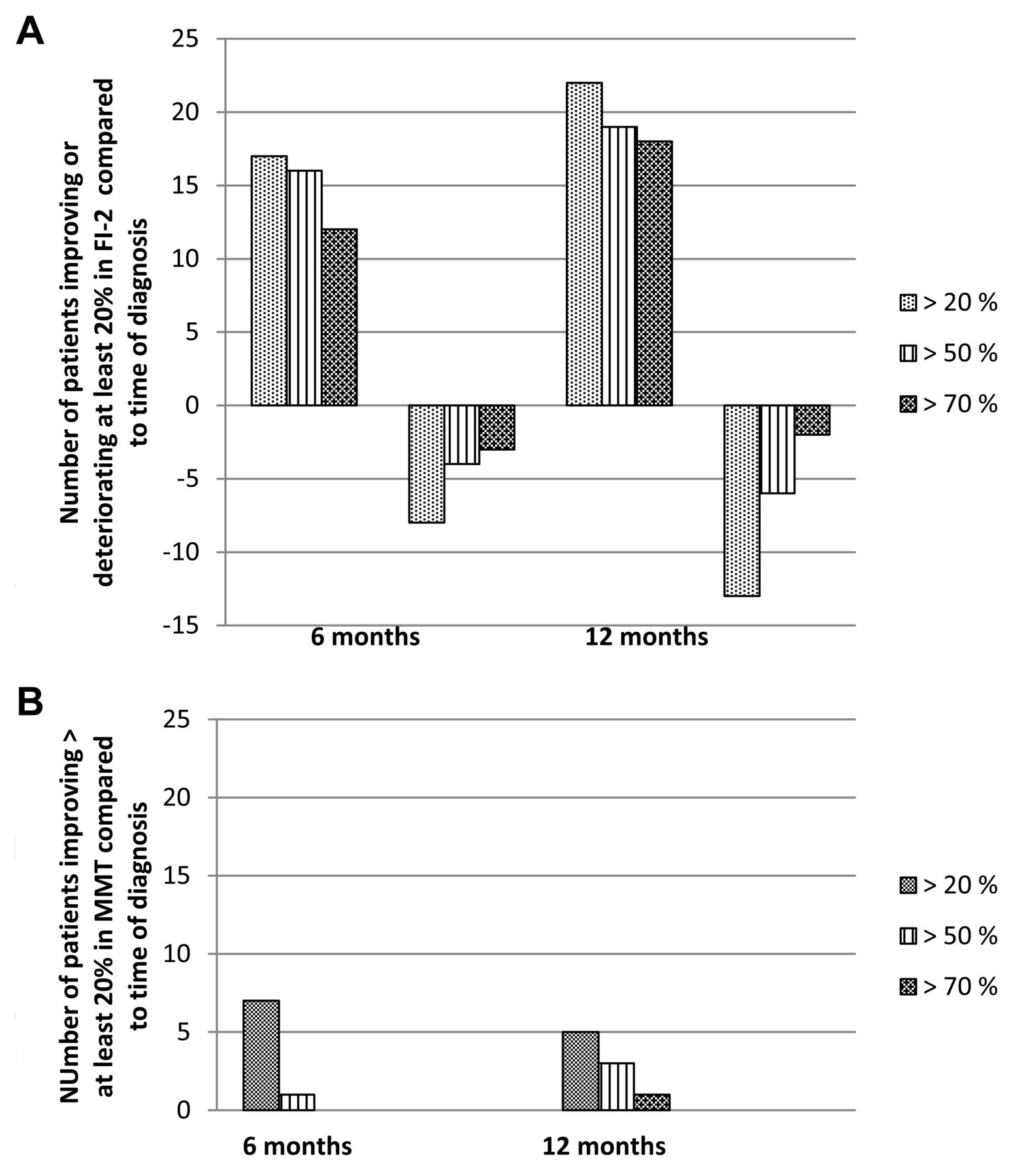
Relative percent change at 6-month followup: 17 patients were responders improving ≥ 20% (defined as a clinically relevant change) in FI-2 and 22 had improved ≥ 20% at 12 months compared to the time to diagnosis. A majority of the responders improved ≥ 70% (Figure 1A). In addition, 8 patients and 13 had worsened ≥ 20% in the FI-2 at 6- and 12-month followup, respectively (Figure 1A). Absolute percent change: 8 and 12 patients improved ≥ 20% at 6 and 12 months, respectively, while 5 patients worsened at 12 months.

(A) No. responders and patients worsening in muscle endurance at 6- and 12-month followup assessed by the Functional Index of myositis (FI)-2. At 6 months, 17 patients had improved ≥ 20%, a majority of them had improved ≥ 50%. Eight patients had worsened ≥ 20%, 4 and 3 of them worsened ≥ 50% and 70%, respectively. At 12 months 22 patients had improved > 20%, of whom a majority improved ≥ 50% or ≥ 70%, and 13 patients deteriorated ≥ 20% of whom 6 and 3 deteriorated ≥ 50% and ≥ 70%, respectively. (B) No. responders in muscle strength at 6- and 12-month followup assessed by the manual muscle test (MMT)-8. At 6 months, 7 patients improved ≥ 20%, of whom 1 improved ≥ 50%. At 12 months, 5 patients improved ≥ 20%, of whom 4 improved ≥ 50% or ≥ 70%. No patient worsened ≥ 20% in MMT.
Regarding relative percent change, at 6 months, 7 patients had improved ≥ 20% in MMT-8 and 5 were improved at 12 months compared to time of diagnosis and no patients worsened ≥ 20% at any timepoint (Figure 1B). In the absolute percent change, 4 patients improved ≥ 20% both at 6 and 12 months followup.
Disease activity
The group improved significantly in disease activity assessed by physician’s global VAS (PGA), the HAQ, and CK levels at 6 and 12 months compared to baseline (p < 0.01–0.001; Table 3). Extramuscular VAS and patient’s global assessment were unchanged, although there was a tendency toward decreased activity at all measurement points (p = 0.05–0.06). Data on PSL dose was used as a measure of response in disease activity at 12 months. Of 49 patients, information was available for 46, and 33 (72%) were responders with a PSL dose of 10 mg/day or less.
Disease activity and patient-reported health. Data are median (quartiles).
Correlations between assessment of muscle function and patient-reported health
At 12 months, there was a high correlation between the FI-2 and the SF-36 domain Physical Function and a moderate correlation between MMT-8 and SF-36 Physical Function (Table 4).
Correlations between the FI-2 and MMT in relation to patient-reported health and the 6-item core set of disease activity measured at 12 months after diagnosis.
Correlations between assessment of muscle impairment and disease activity
At 12 months, there was a moderate to high correlation between the FI-2 and the MMT-8 (Figure 2A) and between FI-2 and the HAQ, with moderate to low correlations with other 6-item core set measures of disease activity (Table 4). Correlations were moderate to low between the MMT-8 and the other 6-item core set measures. There was a low correlation between percent change in the FI-2 and in the MMT-8 (Figure 2B), and no or moderate correlations between the FI-2 and the MMT-8, respectively, and response in disease activity (PSL dose ≤ 10 mg/day; Figure 2C and 2D). There were no or very low correlations between muscle function scores and nonresponders in PSL doses (> 10 mg/day; Figure 2E and 2F).
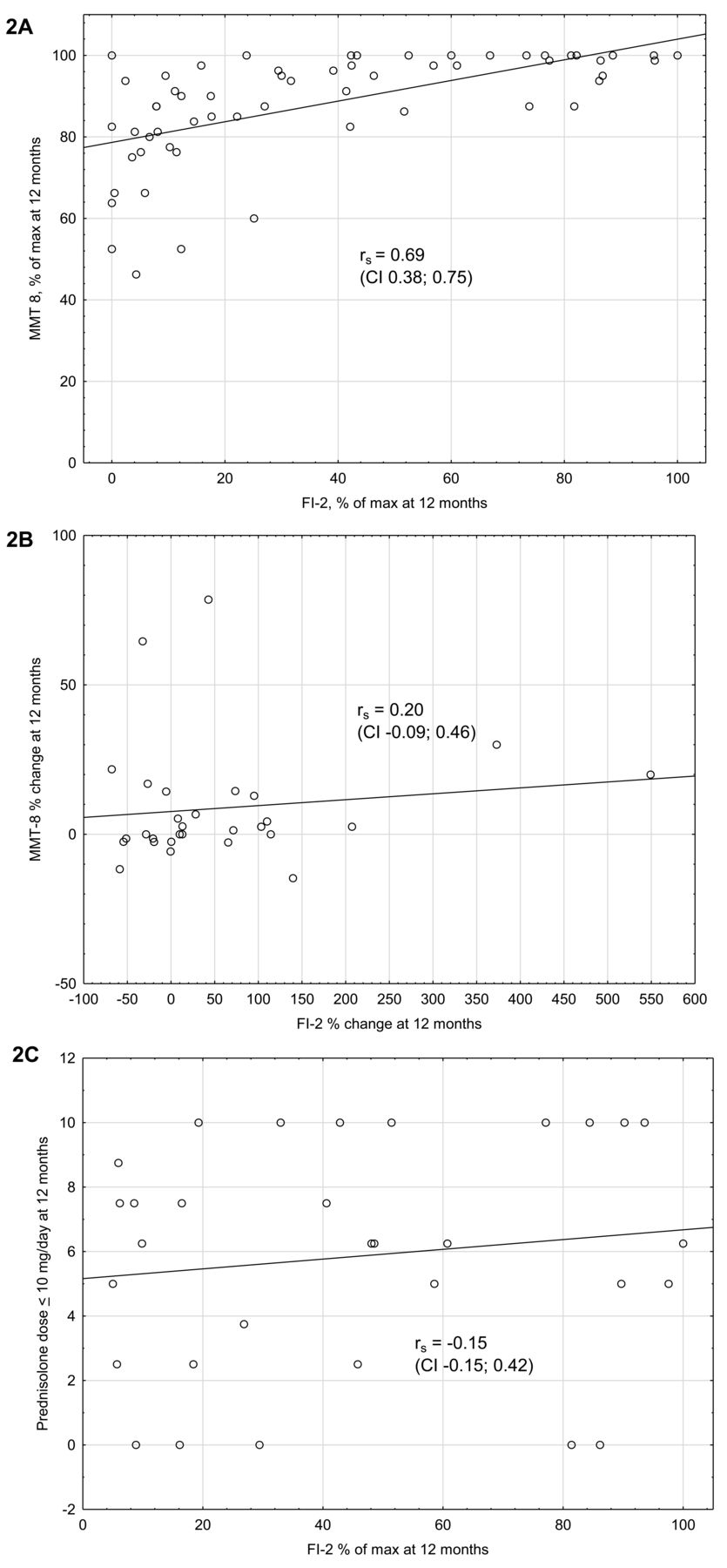

Correlations between the Functional Index of myositis (FI)-2 and the manual muscle test (MMT)-8 and between muscle function and PSL dose at the 12-month followup. (A) There was a moderate to strong correlation between the FI-2 and the MMT-8. (B) There was a low correlation between percent change in the FI-2 and the MMT-8. (C) There was a very low correlation between FI-2 scores and disease activity response, defined as PSL dose < 10 mg/day. (D) There was a moderate correlation between the MMT-8 and PSL dose response. (E–F) There were very low to low correlations between FI-2 and the MMT-8 and nonresponse in PSL dose (> 10 mg/day). PSL: prednisolone.
DISCUSSION
This prospectively followed cohort of patients with PM and DM seemed to have lower percentages for their maximum score on the DRMF measure, FI-2, relative to the percentage of maximum score on the isometric strength measure MMT-8, both at the time of diagnosis and after 1 year of treatment. The majority of patients were nonresponders in FI-2 scores, and some patients had worse FI-2 scores at 12 months after their diagnosis, despite an observed reduction in disease activity. Further, there was a high correlation between patient-reported physical function and FI-2, with a moderate correlation between patient-reported physical function and MMT-8.
Both the FI-2 and the MMT-8 assess similar muscle groups, with the exception that only the FI-2 includes hip flexion. Our results indicate that patients with adult PM and DM might be more limited in DRMF than in isometric muscle strength, pointing out the importance of assessing dynamic muscle function in addition to the recommended MMT-8 in adult PM and DM. The FI-2 probably measures dynamic muscle endurance in patients who are able to perform > 20 repetitions, but more likely measures dynamic muscle strength in patients who are able to perform fewer repetitions. Patients with established PM and DM have reduced muscle endurance relative to healthy controls16, supporting reduced muscle endurance in these patients. The reason for the possible differences in muscle function as assessed by the FI-2 and the MMT are not clear, and further studies evaluating both isometric and dynamic strength and endurance are needed to fully understand muscle impairment in patients with adult PM and DM.
Our results also suggest that impairment in DRMF is potentially more clinically relevant than the impairment in isometric muscle strength in adult PM and DM, both at the time of diagnosis and during the first year subsequent to diagnosis. Studies show that patients with myositis seem to primarily experience limitations in activities requiring muscle endurance, such as walking, biking, climbing stairs, and jogging/running25,26. After 6 and 12 months there was a higher frequency of responders defined as having ≥ 20% improvement when assessed by the FI-2 relative to assessments by MMT-8, which could explain the low correlation between percent improvement between these 2 measures. This indicates that there is a ceiling effect of the MMT-8 with limited room for improvement, which has also been described for some of the scale steps in the MRC scale and other versions of the MMT12.
These patients were treated with conventional immunosuppressive treatment according to the decision of the treating physician in the routine clinic, thus no study protocol was followed. According to Swedish clinical practice, since 1998 patients have been advised to exercise regularly, starting with a home exercise program for the first 3 months, then progressing to other types of aerobic or resistance training during the first year following diagnosis. It was therefore disappointing that in this cohort, the 12-month followup showed that the majority of patients with PM or DM had not improved to an extent considered clinically relevant, whether measured by the FI-2 or the MMT-8. For MMT-8, this could again be explained by a ceiling effect because the median level of MMT at diagnosis was 93.8% of maximal score, which does not permit a 20% improvement. Of greater concern is that about one-third of patients worsened during the first year of their disease relative to their assessment by FI-2 at the time of diagnosis. This is probably not due to disease activity, because most measures of the 6-item core set already showed improvement at 6 months and remained improved at 12 months. There were very low to moderate correlations between FI-2, MMT-8, and PSL dose at 12 months. The reason for the discrepancy between improved disease activity and persistent muscle impairment is not clear, but it does confirm earlier studies that indicated that patients may develop sustained disability despite reduction in disease activity4,5,6,7,8, perhaps more associated to damage than disease activity. There was a high and a moderate correlation, respectively, between self-reported physical function and measures of DRMF and muscle strength, indicating that the impaired DRMF is also reflected in self-reported physical function.
The FI-2 was the first disease-specific validated and functional tool used to assess DRMF for adult PM and DM18. A limitation of its use in clinical practice is that it requires up to 30 min to perform. The development of a shorter version of the FI-2 is in progress. The MMT-8 has satisfactory reliability for 4 of the tasks, moderate for 2, and low for 2 tests. The assessor’s own strength and ability to apply resistance could be a limiting factor of the MMT-815. Another just recently published tool for measuring physical performance, the Adult Myositis Assessment Tool, includes measures of both function and endurance and was developed and validated for adults with PM and DM27. The timed-stands test is also validated for myositis28, but whether it measures muscle endurance is questionable because it only requires 10 sit-to-stands. Muscle endurance can also be assessed by the Biodex system, but this is costly and needs trained personnel18.
The majority of the patients who improved according to our criteria (relative percent change) improved by more than 70% on the FI-2, indicating a clinically relevant change. The responders who improved by ≥ 20% and the group who worsened by ≥ 20% all had equally low median FI-2 scores at the time of diagnosis. Thus, the FI-2 score at time of diagnosis did not predict response to treatment. Further, all responders to the FI-2 showed improvements exceeding the error of measurement, which varied between 5% and 16% for the different tasks21. Fewer patients were responders in the MMT-8, which could be explained by the already high scores at baseline. On the other hand, no patient deteriorated ≥ 20% in MMT-8. However, the error of measurement for the MMT has, to the best of our knowledge, not yet been established in adult myositis.
Sex, the myositis subgroup, autoantibody profile, and medication did not predict improvement or worsening. Although the women had only about 30% of maximal FI-2 score at baseline, they did not improve as a group. However, there was a large variation in FI-2 scores among the women, for which we have no explanation. It has been shown previously that the time from symptom onset to diagnosis and treatment is crucial to the regaining of muscle function29. This could not be assessed in our study because data on time from symptom onset to diagnosis and treatment were not available.
Our study has limitations. No published reference values are available for the FI-2; thus it is unclear whether patients with PM and DM have reduced DRMF relative to healthy individuals, but preliminary results from ongoing data collection of reference values indicate that most healthy individuals perform close to 100% on all the tasks except for neck flexion. This is a descriptive study based on register data collected in clinical practice, thus it is missing data related to muscle function and disease activity at followup. Data on self-reported health, disease activity, and antibodies were not available for all patients at baseline, limiting the power of the analysis. Further, the lack of information on physical activity or exercise habits for the included patients during their first year after diagnosis is a major limitation. Exercise is an important part of treatment for patients with myositis9,10 and it could have a substantial effect on the development of muscle impairment over time. Information regarding type of exercise, frequency, and intensity has not been registered systematically in the medical charts, and was at the time of the study not included in the SweMyoNet. However, questions on physical activity and exercise as well as a rehabilitation module enabling registration of exercise intensity and frequency have recently been added to the SweMyoNet. This will improve research on register-based treatment responses in the future.
Patients with recent-onset PM and DM were characterized by reduced DRMF, measured by FI-2, relative to isometric muscle strength measured by MMT-8. This indicates the need to also assess DRMF in addition to MMT to identify objective muscle impairment that is important to the patients. Although a number of patients responded to the medical treatment with improved DRMF, the majority of patients had unchanged or even lower DRMF 1 year after diagnosis, which was strongly associated with reduced patient-reported physical function, indicating that the treatment used today for these patients is far from optimal. There were low or moderate relationships between muscle function and clinical disease activity, indicating that other mechanisms are important contributors to the persistent low muscle function in patients with PM and DM.
Acknowledgment
To Jenny Bergegård and Anna Hallén for their assessments and the registration of FI-2 and other clinical data in SweMyoNet. We also thank Dr. Mimori, Kyoto University, Japan, for the antibody analysis.
Footnotes
Supported by the Centre for Care Science at Karolinska Institutet, Swedish Rheumatism Association, the Swedish Research Council, Funds of the Karolinska Institutet, Börje Dahlin Foundation, King Gustaf V 80-year Foundation, the “Regional Agreement on medical training and clinical research (ALF) between Stockholm City Council and Karolinska Institutet,” and the European Science Foundation.
- Accepted for publication November 3, 2017.








{kind=link}
{kind=link}
{kind=link}