

Abstract
Objective. To explore the relationship between rheumatoid arthritis (RA) disease activity and functional disability over time, considering indirect (predictive) and direct (concurrent) associations as well as the influence of radiographic joint damage and treatment strategy.
Methods. Functional disability [Health Assessment Questionnaire (HAQ)], disease activity [28-joint Disease Activity Score (DAS28)], and radiographic joint damage [Sharp/van der Heijde score (SHS)] were measured in 4 consecutive randomized controlled trials with increasingly intensive (tight control) treatment strategies. Average followup time for the 3 cohorts was 97, 53, and 50 months, respectively. Next to current DAS28, the previous DAS28 was used to study the predictive effect of a change in DAS28 on progression of functional disability (HAQ). Finally, it was investigated whether SHS mediated the predictive effect of DAS28.
Results. In patients treated with intensive treatment strategies, the progression of HAQ over time was statistically significantly less (p < 0.0001). The predictive influence of DAS28 on HAQ progression increased over the duration of the disease. SHS was not found to influence HAQ progression and did not mediate the predictive effect of DAS28. In the less intensively treated patients, the direct effect of disease activity decreased with disease duration, and contrarily, SHS did influence HAQ progression, but was not found to (fully) mediate the predictive effect of DAS28.
Conclusion. In patients with RA treated with modern treatment strategies, there is less functional decline over time. Further, disease activity does predict functional decline but joint damage does not. This might indicate that factors associated with cumulative disease activity but not visible on radiographs can influence functional decline in patients with RA. This further underlines the importance of disease activity as a treatment target in early RA and in established RA.
It is generally acknowledged that inflammatory disease activity over time leads to joint damage, both of which result in functional disability in patients with rheumatoid arthritis (RA)1,2,3,4,5,6. This is the rationale behind current “tight control” or “treat to target” strategies, directed at obtaining low disease activity in patients. Secondary, radiographic signs of the disease are used as treatment target5.
Functional disability has been found to be related to several longterm outcomes as well as patient quality of life, medical costs, and work disability7,8,9 and is therefore a patient-important outcome. The relationship between disease activity and functional disability constitutes a direct effect (through signs and symptoms of current disease activity) and an indirect (or predictive) effect of disease activity over time on joint damage leading to functional disability10,11,12,13. The direct effect was found to be dependent on the phase of the disease, with the influence of current disease activity on functional disability decreasing over time10,14,15. However, it has been suggested that with more intensive disease activity-driven treatment, this decrease is not seen16. Moreover, the predictive effect of disease activity for functional disability has not been studied longitudinally or explicitly reported to date, especially regarding the intensity of treatment strategy and the role of radiographic joint damage.
These relationships are important for the interpretation of disease activity in tight control treatment strategies that aim to limit functional disability.
Over recent decades, RA treatment has advanced to a more intensive (tight control) treatment strategy with (combination) disease-modifying antirheumatic drugs (DMARD), and more recently, biological therapy17,18,19,20.
We hypothesized that the effect of current disease activity on functional disability decreases over time, especially in less intensively treated patients, and further, that disease activity also predicts progression of functional disability. We also addressed the following questions: (1) are these relations influenced by treatment strategy? (2) are these relations influenced by disease duration? and (3) is the predictive effect of disease activity mediated by radiographic joint damage?
MATERIALS AND METHODS
Study population
The followup data were used from 4 randomized clinical trials (RCT) as performed consecutively by the Utrecht Rheumatoid Arthritis Cohort study group (The Netherlands). The first study consisted of 2 parts; the first part included 238 patients between 1990 and 1994 and compared treatment according to the Pyramid approach and DMARD treatment. In the DMARD group, patients were treated with methotrexate (MTX), hydroxychloroquine, or intramuscular gold. The Pyramid approach constituted treatment with nonsteroidal antiinflammatory drugs (NSAID) initially to control inflammation and pain, and if not effective, DMARD treatment was started. From 1994 until 1998, 313 patients were randomized to one of the DMARD arms only to compare the efficacy and safety of these different DMARD17,20. Because these 2 studies used the same DMARD treatment arms and the same design, we combined them and referred to the result as the Pyramid study. The second study is the Computer Assisted Management in Early Rheumatoid Arthritis (CAMERA I) trial, conducted between 1999 and 2003. In it, 299 patients were randomized to an intensive (tight control) MTX-based treatment strategy or to a conventional MTX-based strategy. Finally, in the third study, CAMERA II, between 2003 and 2008, 236 patients were included to investigate whether adding 10 mg/day prednisone to an MTX-based tight control strategy increased effectiveness19.
All these studies included patients with RA according to the 1987 revised American College of Rheumatology criteria, with a disease duration < 1 year and no prior disease-modifying treatment, in the same participating centers in the broader region of Utrecht. All trials had a duration of 2 years and were followed by an extension phase in which data on disease activity and functional disability of patients were collected yearly and treatment strategy was no longer defined by study protocol17,18,19,21.
Clinical variables
Disease activity was measured with the 28-joint Disease Activity Score (DAS28), calculated using the erythrocyte sedimentation rate, joint counts for swelling (SJC28) and tenderness (TJC28) based on 28 joints, and a visual analog scale (VAS) for general well-being22,23.
Functional disability was measured using the Health Assessment Questionnaire (HAQ)24 as validated for the Dutch population25. Radiographic damage was measured using radiographs of hands and feet evaluated according to the Sharp/van der Heijde score (SHS) using the total score26.
For the current analysis, the annual DAS28, HAQ, and SHS measurements were used.
To evaluate the predictive influence of disease activity, a previous DAS28 (DAS28T-1yr) was defined as the DAS28 measurement taken 1 year earlier. Apart from these measurements, data on age, sex, and body mass index (BMI) were also available.
Statistical analyses
Standard descriptive statistics were used for the different populations.
To test the effect of treatment strategy on progression of functional disability, a linear mixed model analysis with a random intercept was used. In this analysis, the repeated measures of the outcome (HAQ) within individual patients and between subjects are taken into account, as well as within-subject variables. To focus on a longitudinal interpretation (i.e., progression of functional disability), a so-called autoregressive model analysis was performed by adding the HAQ measurement 1 timepoint earlier to the model. The variable time (i.e., disease duration) and treatment strategy were added to the model as independent variables. Treatment strategy was divided into 4 groups based on the overlapping arms of the consecutive studies: Pyramid approach, DMARD treatment, MTX-based tight control treatment, and finally the most intensive MTX-based tight control with glucocorticoid treatment. Other independent variables studied in the model were SHS, HAQ, DAS28, BMI, age at disease onset, sex, and rheumatoid factor (RF) positivity.
We also investigated whether the (possible) influence of treatment strategy on progression of HAQ was stable over time by testing an interaction term (time*treatment strategy) in the model.
Because damage and disease activity were scored slightly differently for the Pyramid study and the CAMERA I and II studies, 2 separate analyses were done for these studies and the results compared. For the first study, the Thompson score27, which scores and weighs 38 joints [the sum of the score varies between 0 (no inflammation) and 534 (maximum inflammation)] only when they are swollen and tender, was used instead of the SJC28/TJC28, therefore the DAS28 score was estimated using a regression function based on an external cohort (Appendix 1). Although in both cohorts SHS were used to quantify radiographic joint damage, observers were different and instructions slightly different (i.e., cumulative vs “random”). To study the direct and predictive influence of DAS28 on progression of functional disability, the above analysis was used, also adding current as well as previous DAS28 (DAS28T-1yr) to the model.
Modification of the effect of DAS28 and DAS28T-1yr by disease duration was studied by including interaction terms between time and DAS28 variables in the model.
All variables were added to the model and removed stepwise to arrive at a final model with variables that were statistically significantly related to outcome, adjusting for age and sex. The results of the regression coefficients of time-varying variables can be interpreted as the association between changes in the predictor variables (e.g., a change in DAS28) in relation to changes in the outcome variable.
To further understand the predictive association of DAS28 with HAQ progression and investigate whether it can be regarded as a proxy for progression of joint damage (i.e., whether radiographic joint damage is a mediator of this predictive association), we performed a mediation analysis. First, it was investigated whether DAS28T-1yr was associated with SHS (if not, SHS cannot be a mediator). In the next step we tested the association of SHS with HAQ (leaving out the DAS28T-1yr terms in the model). In the last step, the relation between DAS28T-1yr and HAQ was tested, correcting for SHS.
All the analyses were done using SAS version 9.1.3, and p values < 0.05 were considered statistically significant.
RESULTS
Patient characteristics
Table 1 describes baseline characteristics of the 1034 patients, overall and per study. Baseline demographic characteristics were comparable between the 3 studies, with two-thirds of the patients being women and a mean age around 54 years. The DAS28 and HAQ at disease onset were observed to decrease slightly from the earlier trials to the more recent trials (Figure 1). Around 65.6% of all patients were RF-positive. No statistically significant differences were observed.
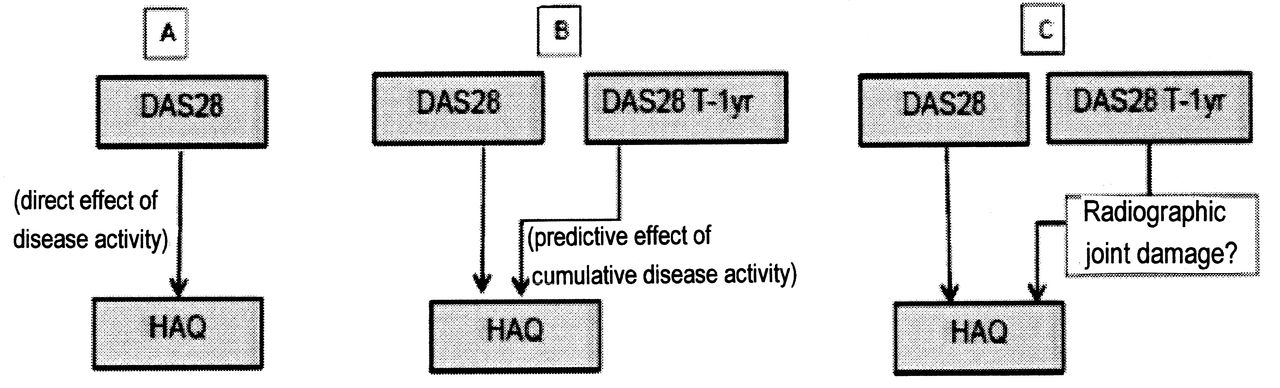
Direct and indirect relation between 28-joint Disease Activity Score (DAS28) and Health Assessment Questionnaire (HAQ). A. A direct effect of disease activity exists. B. Cumulative disease activity predicts the progression of functional disability over time (DAS28 T-1 yr). C. This association might be mediated by radiographic joint damage. It is not clear how and whether these associations change over the duration of the disease. Another question is the influence of the treatment intensity.
Baseline characteristics of the 3 cohorts. Values are mean (SD) unless otherwise indicated.
Course of functional ability and disease activity over time
In general, disease activity remained about 1 point higher in the Pyramid study and functional disability and radiographic damage progressed more over time as compared to CAMERA I/II (Figure 2A, 2B, 2C).
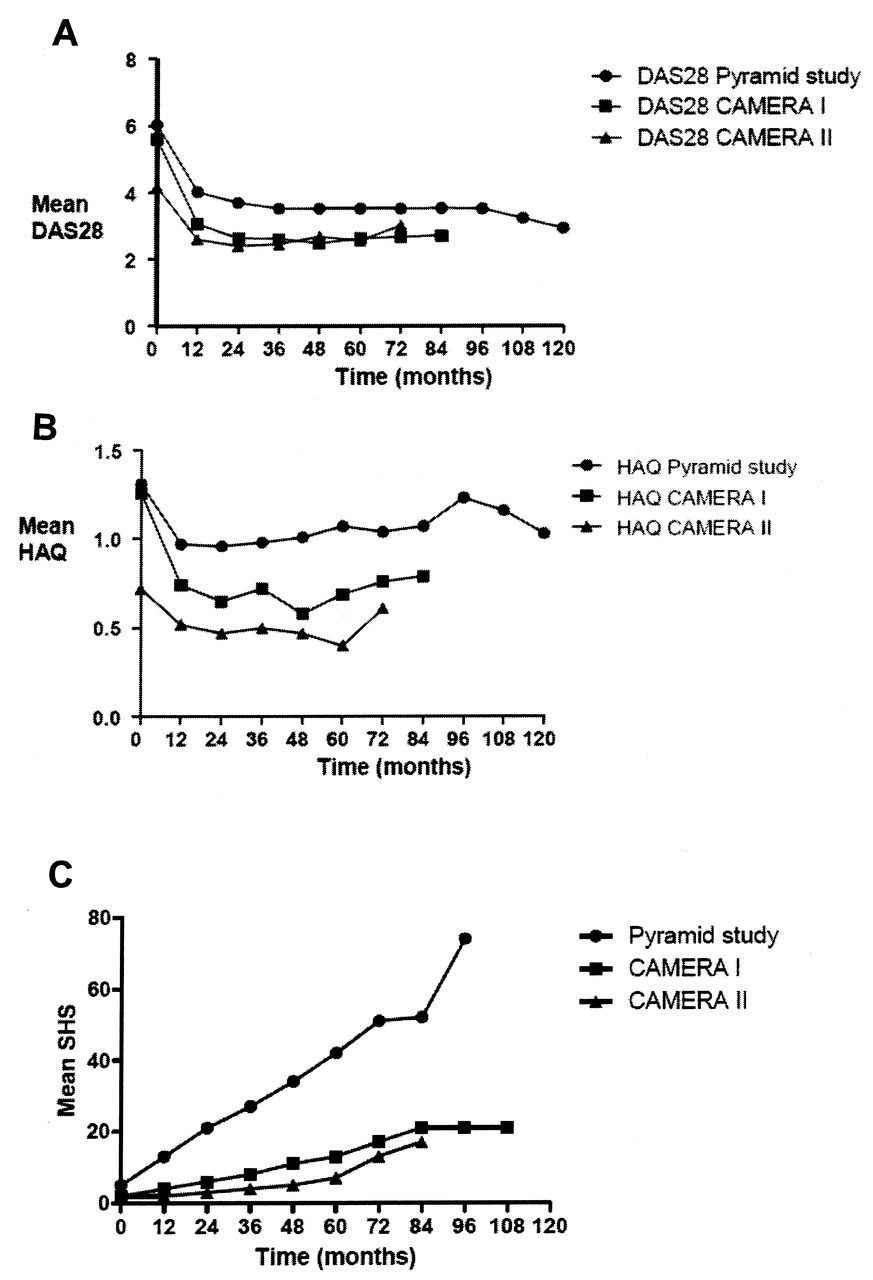
A. Course of the disease activity score in the 3 cohorts. B. Course of functional disability over time, as measured by the Health Assessment Questionnaire (HAQ) in 3 cohorts. C. Course of Sharp/van der Heijde Score (SHS) over time in the 3 cohorts. DAS28: 28-joint Disease Activity Score.
Effect of treatment strategy on progression of functional disability
In the combined analysis, HAQ was (as expected) found to progress over time with a decreasing rate. Treatment strategy was associated to the progression of functional disability with more intensive treatment strategies having less progression of functional disability over time. The Pyramid approach showed higher progression of HAQ as compared to all the other treatment strategies (p < 0.0001 for all comparisons). Over time, HAQ progression was lower (p < 0.02) for both the MTX-based tight control strategies as compared to the DMARD strategy. Other differences between the strategies were not statistically significant.
The influence of treatment was not found to be statistically significantly modified by disease duration (i.e., the effect of treatment strategy remained constant over time).
Direct and predictive effect of disease activity on progression of functional disability
In the CAMERA I and II and Pyramid study, current DAS28 and DAS28T-1yr were positively associated with HAQ.
The influence of a change in current DAS28 on HAQ was found to decrease with time (disease duration); however, in CAMERA I and II, this was not statistically significant (p = 0.3354; Table 2).
Final regression model for Pyramid study and CAMERA I and II.
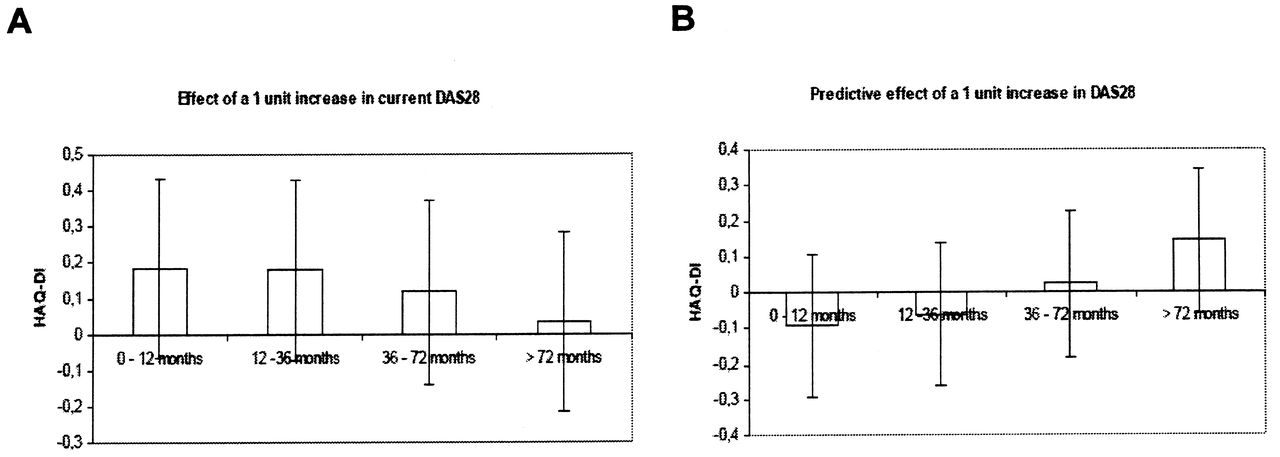
In both groups, the predictive relation between disease activity (DAS28T-1yr) and HAQ progression increased over time (p < 0.0001), suggesting that the influence of preceding disease activity on the progression of functional disability becomes more pronounced over the course of the disease. To further represent the direct and predictive influence of disease activity, the model results for the CAMERA I and II data were presented in a graphical manner. For this purpose the variable time was categorized (Figure 3).

Progression of Health Assessment Questionnaire-Disability Index (HAQ-DI) as a result of 28-joint Disease Activity Score (DAS28) over time. A. Increase in HAQ with a unit increase in DAS28 in different time intervals. B. Progression of HAQ 1 year after a 1-unit increase in DAS28.
Mediation analysis
In the CAMERA I and II data, a clear association between disease activity (DAS28T-1yr) and SHS was observed (β = 0.492; p = 0.0005). However, the relation between SHS and HAQ could not be established (β = 0.002; p = 0.331). After correcting for SHS, the relation between DAS28T-1yr and HAQ did not change and SHS remained nonsignificant. Hence mediation by SHS could not be established.
In the Pyramid study the relation between DAS28T-1yr and SHS was also observed (β = 0.680; p = 0.005). Contrary to CAMERA I and II, there was an association between SHS and HAQ (β = 0.001; p = 0.0004). Finally, when both DAS28T-1yr and SHS were added to the model, both coefficients were slightly lower but still statistically significant (borderline for SHS, p = 0.06). Hence only partial mediation was observed.
The above results might indicate that disease activity influences progression of functional disability at least partly, separately from causing radiographic joint damage. To test this hypothesis, an analysis was performed only in patients in the CAMERA I and II data who had no or minimal radiographic joint damage (i.e., followup data were used for patients with no radiographic damage or an SHS score < 5) and the relation between DAS28T-1yr and progression of HAQ over time was still significant (β = 0.0022; p = 0.003). This indicates that even in the absence of visible radiographic joint damage (on hand and foot radiographs), disease activity influences the progression of functional disability.
DISCUSSION
We investigated the influence of disease activity on functional disability over the course of the disease in patients with RA. The direct (concurrent) effect as well as the predictive (indirect) effect on HAQ 1 year later were found to be important, independent of each other. However, the direct effect was observed to become less important over time (although nonstatistically significant for more intensively treated patients) and the indirect effect more important over time. With increasing intensity of treatment strategy, the progression of functional disability was also found to be lower. Our study showed that disease activity remains important regarding functional decline of individual patients over the course of the disease, although through different mechanisms. In the initial phase of the disease the direct effect of disease activity (through signs and symptoms of the disease) on functional disability is important; the later stage of the disease is marked by the indirect effect of disease activity through ongoing progression of functional disability over time (even without radiographic damage visible).
It has been reported that there is a strong relation between disease activity, structural damage, and functional disability throughout the disease course. Structural damage and functional disability are especially linked in later stages of the disease5,14,28,29. We found that radiographic joint damage was not related to progression of functional disability in the intensively treated patients (CAMERA I and II data), although a relation between disease activity and progression of damage was found. In the less intensively treated patients (Pyramid approach), we did observe joint damage to predict functional decline. This suggests that in early and established disease, disease activity and radiographic joint damage influence progression of functional disability through (partly) different mechanisms. It also indicates that joint damage is not a good indicator for functional decline and might be less important (in comparison with disease activity) as a treatment target for patients treated intensively.
Our results are also in line with findings of earlier studies on the relation between disease activity and functional disability over the course of RA1,10,30. Partly contrary to the result of van der Kooi, et al16, who found that DAS28 was associated with functional disability independent of disease duration, we observed this relationship to become weaker over the course of the disease, although nonsignificantly in intensively treated patients. Also, over time the functional ability of patients with RA worsens even in patients treated intensively, as seen in other studies6,11,31, and in line with the observation that functional disability increases with age in the general population32,33.
Our study had some limitations. Although our studies were comparable in design and inclusion/exclusion criteria and had a similar setting, they differed in followup (because of the different calendar time when they were started) and involved slightly different measurements. Duration of followup did not confound the relationship between DAS28 and HAQ: restricting the analysis to data with comparable followup did not change the results. Regarding the different measurements, we did subgroup analysis; the analyses can be compared because the concepts being measured are the same. Clearly all validated measurements of disease activity and radiographic joint damage are neither all-inclusive nor perfect.
HAQ has been described to have a ceiling effect that might (partly) explain the decreasing effect of current DAS2834. However, we found an increasing influence of previous DAS28, indicating that this ceiling effect is not influencing our results to a large extent. The increasing effect of DAS28 might be explained by existing damage, making patients more prone to the effects of the disease activity.
Treatment was defined only for the first 2 years and thereafter treatment was according to the treating physician in all studies. However, in the more recent studies, more intensive treatment strategies were probably also used after the trial period.
As reported, with a more intensive treatment strategy, less radiographic progression was observed35. Less radiographic progression might make it more difficult to show a (statistical) association. Indeed, we did not find this relation in the more intensively treated patients. However, we did observe a clear relation of disease activity with radiographic damage, which suggests that (variation in) the SHS score was sufficient to show associations. Even in patients without radiographic damage, HAQ progression was predicted by disease activity, indicating that this is not only age-related progression. It also supports our hypothesis of a (partly) different mechanism for the relation of disease activity with functional decline and radiographic damage with functional decline. The first mechanism might, for instance, be related to irreversible damage on structures not evaluated by SHS.
Our results suggest that more intensive (tight control) combination treatment strategies decrease the progression of functional disability in patients with RA. Disease activity influences the progression of functional disability; early in the disease, the direct effect due to signs and symptoms of inflammation is important, and later the indirect or predictive effect becomes more important. This predictive effect of disease activity seems to be partly independent of the influence of radiographic joint damage. This might indicate that factors associated with cumulative disease activity, but not visible on radiographs, can influence functional decline in patients with RA. This finding further supports the importance of disease activity as a treatment target for RA during the course of the disease, later as well as earlier.
Acknowledgment
We thank all the participating rheumatologists and research nurses of the Utrecht Rheumatoid Arthritis Cohort Study Group for their contribution.
APPENDIX 1. DAS28 score estimate using a regression function based on an external cohort.
Footnotes
-
Supported by the Center for Translational Molecular Medicine and the Reumafonds.
- Accepted for publication May 6, 2013.








{kind=link}
{kind=link}
{kind=link}