

Abstract
Objective. Reduced work participation (WP) is a common problem for patients with rheumatoid arthritis (RA) and generates high costs for society. Therefore, it is important to explore determinants of WP at the start of tumor necrosis factor inhibitor (TNFi) treatment, and for changes in WP after 2 years of TNFi treatment.
Methods. Within the Dutch Rheumatoid Arthritis Monitoring (DREAM) biologic register, WP data were available from 508 patients with RA younger than 65 years and without an (early) retirement pension. WP was registered at start of TNFi treatment and after 2 years of followup and was measured by single patient-reported binary questions whether they had work, paid or voluntary, or had a disability allowance or a retirement pension. Determinants measured at baseline were age, sex, disease duration, functional status [through Health Assessment Questionnaire-Disability Index (HAQ-DI)], 28-joint Disease Activity Score (DAS28), rheumatoid factor, presence of erosions, number of previous disease-modifying antirheumatic drugs, and number of comorbidities. During the 2 years of followup, HAQ-DI response and European League Against Rheumatism response were measured. Univariate analyses (excluded if p value was > 0.2) and multivariate (excluded if p value was > 0.1) logistic regression analyses were used.
Results. Determinants associated with WP at baseline were having a better HAQ-DI (OR 0.32, p = 0.000) and male sex (OR 0.65, p = 0.065). After 2 years of TNFi therapy, 11.8% (n = 60) started to work and 13.6% (n = 69) stopped working. Determinants associated with starting to work were better baseline HAQ-DI (OR 0.58), positive RF (OR 2.73), and young age (OR 0.96); and for stopping work, worse baseline HAQ-DI (OR 2.74), low HAQ-DI response (OR 0.31), and comorbidity (OR 2.67), all with p < 0.1.
Conclusion. Young patients with RA and a high functional status without any comorbidity will have a better chance of working. This supports the main goal in the management of RA: to suppress disease activity as soon and as completely as possible to prevent irreversible destruction of the joints, and thus maintain a good functional status of the patient. Because of the low proportion of variance explained by the models in this study, other factors besides the ones studied are associated with WP.
Work disability is common in patients with rheumatoid arthritis (RA) because of pain, functional impairment, and fatigue1,2,3. Work disability occurs frequently in both early and longstanding RA, 40% and 60%, respectively4,5. This is not only an economic loss for society, but also a burden for patients. Paid work is associated with better health-related quality of life (HRQoL) in patients with RA6 and could therefore lead to better cost-effectiveness outcomes. Better HRQoL is also related to the use of tumor necrosis factor inhibitors (TNFi)7,8,9. TNFi have proven to be very efficacious (decreasing disease activity, preventing damage progression, and reducing functional disability) in several clinical trials10,11,12. Without doubt, there are remarkable advantages using these drugs. However, there is a notable disadvantage: TNFi are expensive drugs compared to the traditional disease-modifying antirheumatic drugs (DMARD). Therefore, direct RA-related medication costs have increased substantially since the introduction of TNFi13,14. However, the positive effects of TNFi may lead to a reduction in the number of hospitalizations and increase the work participation (WP) of patients with RA. Because WP is an important cost driver, it would support the cost-effectiveness of TNFi treatment if TNFi improves WP.
A systematic review of controlled and uncontrolled studies on WP showed that TNFi have a positive effect on sick leave and productivity, but effects on employment status are still unclear, especially in patients with established RA15. In daily clinical practice TNFi are often prescribed to patients with established RA and it remains uncertain whether TNFi can have a positive effect on WP in established RA and which determinants can influence this positive effect. Functionality [as measured by Health Assessment Questionnaire-Disability Index (HAQ-DI)]16,17,18,19,20,21,22,23,24,25,26, age19,20,21,22,24,25,26,27,28, education level18,19,20,22,23,25,27, and physical job demands19,20,21,22,24,26,28,29,30 have shown to be associated determinants in WP in previous studies. However, most of the previous studies about determinants are from the prebiologic era and have commonly been carried out on small patient cohorts; most often on patients with early RA. Within the medical field, knowledge about clinical predictors for work participation and for changes thereof can help to determine whether it is possible to influence WP with treatment. Therefore, the objectives of this study were (1) to establish clinical and social demographic determinants of WP at the start of TNFi treatment, and (2) to establish the determinants for changes in WP after 2 years of treatment with TNFi.
MATERIALS AND METHODS
Design
This is a cohort study using data from the biologic register of the Dutch Rheumatoid Arthritis Monitoring (DREAM) project31. The DREAM biologic register includes patients with RA who began taking TNFi in one of 13 participating centers in the Netherlands since February 2003. Data collection continues if patients change or stop using biologic agents. According to the Dutch regulations, this register does not need ethical approval because it is an observational study. However, patients included in the study have signed informed consent for the use of their data for scientific purposes.
Inclusion/exclusion criteria
All patients included were diagnosed with RA according to the 1987 American College of Rheumatology classification criteria32, had moderate to high disease activity [28-joint Disease Activity Score (DAS28) > 3.2], received prior treatment with at least 2 other DMARD, including methotrexate, and had no absolute contraindication for TNFi (e.g., pregnancy, presence of a serious infection). The inclusion criteria for the DREAM biologic registry are based on the Dutch regulations for reimbursement. In the Netherlands, all patients with RA have access to TNFi through the Dutch health insurance system and all out-patient rheumatology care is hospital based.
For these specific analyses, patients had to have WP data available at baseline and after 2 years of followup. Moreover, patients older than 65 years of age after 2 years of followup were excluded because 65 is the legal age at which people are entitled to a retirement pension in the Netherlands. Patients with an (early) retirement pension were also excluded from the analyses. After retirement, it is uncommon to keep or start working.
Assessments
Patients were assessed at the start of TNFi treatment (baseline) and every 3 months thereafter for the first 2 years. Baseline assessments included age, sex, rheumatoid factor (RF) positivity, disease duration, presence of erosive disease, previous and current antirheumatic treatment, comorbidities [cardiovascular disease, diabetes mellitus, chronic obstructive pulmonary disease (COPD), and malignancy], DAS2833, and the HAQ-DI34. The DAS28 is a reliable and valid instrument to measure disease activity of patients with RA by using 4 components: the tender joint count of 28 joints, the swollen joint count of 28 joints, the erythrocyte sedimentation rate (ESR), and the visual analog scale of general health35. The tender and swollen joints were assessed by trained nurses. The HAQ-DI is a self-reported questionnaire to measure the functionality of patients. The questionnaire is proven to be reliable and valid for patients with RA36. DAS28, HAQ-DI, medication use, and the presence of comorbidities were reassessed at the scheduled clinic visits. Further, at the start and after 2 years, patients indicated whether they had paid work, did voluntary work, received a retirement pension, or received a work disability allowance, by responding to a precoded question on work status (more than 1 answer allowed). Patients who had paid work or did voluntary work were defined as working. Voluntary work, as well as paid work, is valuable to the individual and to the societal and economic environment37,38. All data were prospectively entered in a computerized database.
Statistical analyses
Clinical determinants of WP at the start of TNFi treatment were analyzed by comparing the group of patients who worked (paid or voluntary work) with the group of patients who did not work (no paid work or voluntary work). Change in WP after 2 years of treatment with TNFi was analyzed by comparing the WP at baseline with the WP after 2 years using cross tabulation.
Determinants for WP at baseline were analyzed using logistic regression in all patients using work status (working and not working) as the dependent variable. Determinants for starting work were analyzed using logistic regression for all patients not working at baseline and using work status at 2 years as the dependent variable. Determinants for stopping work were analyzed by using logistic regression for patients working at baseline and using work status at 2 years as the dependent variable. For all analyses, these factors were considered as possible determinants: age, sex, HAQ-DI at baseline, DAS28 at baseline, number of previous DMARD, RF, disease duration, presence of erosions, and number of comorbidities (cardiovascular disease, diabetes mellitus, COPD, and malignancy). For the analyses of change in WP, the European League Against Rheumatism response, based on the DAS28 at 6 months, and the HAQ-DI difference at 6 months compared to baseline were also considered possible determinants. To study which clinical determinants were associated with (change in) work participation, first univariate analyses were performed using Student’s t test, Mann Whitney U test, and chi-square tests as appropriate. The variables that appeared to be different with a p < 0.2 in the univariate analysis were included in a full multivariate logistic regression model. Using backward selection, all variables with a p > 0.10 were removed stepwise.
RESULTS
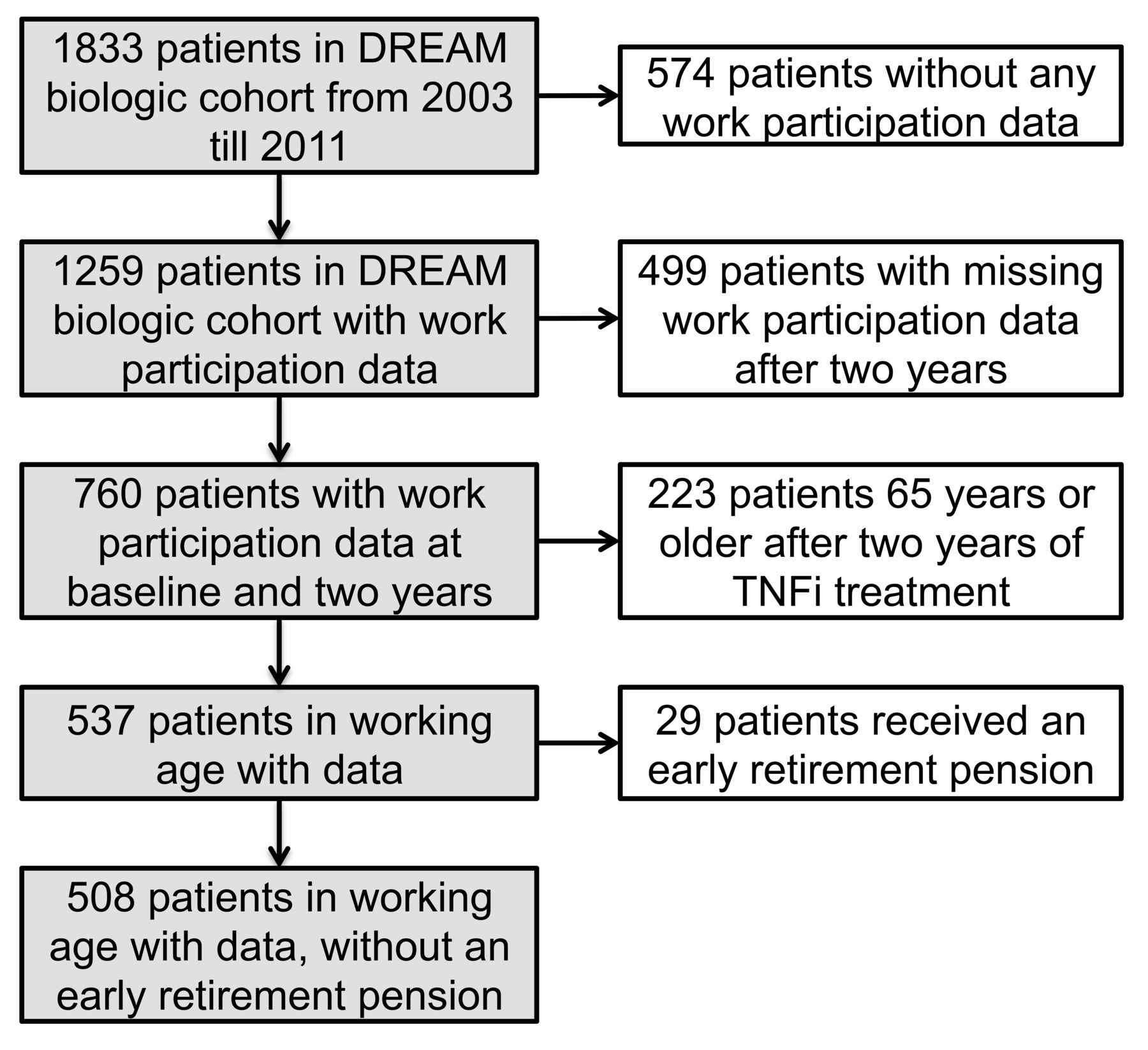
Between February 2003 and June 2011, a total of 1833 patients started on one of the TNFi: etanercept, adalimumab, or infliximab. During this period, 1259 patients filled in a questionnaire about their WP. For 760 patients, the WP questionnaire was available at baseline and after 2 years of followup; 537 were eligible because they were < 65 years old after 2 years of TNFi treatment, and 508 of those patients did not receive any (early) retirement pension (Figure 1). Patients with available WP data did not differ significantly in age, sex, disease duration, RF, erosions, DAS28, or HAQ-DI from the patients not included in the study because of missing data on WP (not shown). Further, only 10.2% of the patients stopped TNFi treatment within 2 years after start and did not start a second TNFi within 6 months after stopping. Of the study population, 89.8% were treated with TNFi for 2 years.

Composition of the study population. DREAM: Dutch Rheumatoid Arthritis Monitoring biologic register; TNFi: tumor necrosis factor inhibitor.
Characteristics of the patients studied are described in Table 1. Change in WP is described in Table 2. All determinants at baseline, except age, RF positivity, number of previous DMARD, and the number of comedications were significantly different (p < 0.2) between the patients who did work and those who did not work at baseline. The significantly different variables were all included in the multivariate analyses. Multivariate analysis showed that higher HAQ-DI scores (lower functional status) and female sex resulted in a lower probability of having work at the initiation of TNFi (Table 3). With the final model, 13.6% of work status at baseline can be explained.
Patients’ characteristics at baseline.
Change in work participation over 2 years.
Logistic regression analysis of determinants for work participation before TNFi treatment (n = 508).
WP change
At baseline, 291 of the patients worked (57.3%): 257 (50.6%) had paid work, 34 (6.7%) did voluntary work, and 4 (0.8%) had a paid job and did voluntary work. Thus, 217 (42.7%) patients did not work. After 2 years of TNFi therapy, some changes were found in the WP of patients with RA: 60 (11.8%) started working and 69 (13.6%) stopped working. Nevertheless, most patients had no changes in work participation: 222 (43.7%) worked at baseline and after 2 years, and 157 (30.9%) did not work at baseline or after 2 years followup. The distributions of different values across WP at baseline and WP after 2 years of TNFi treatment are equally likely (McNemar p = 0.481). Table 2 describes the change in WP in more detail than the division of work and no work.
Multivariate analysis showed that lower HAQ-DI scores at baseline (better functional status), being RF-positive, and younger age result in an increased chance of gaining work (Table 4). In the final model, the variance of 14.3% can be explained by patients starting to work within 2 years of followup. When focusing on patients who had work at start of TNFi (n = 291), multivariate analysis showed that higher HAQ-DI scores at baseline (lower functional status), comorbidities, and worse HAQ-DI response increased the chances of stopping work. With the presented model, 12.5% can be explained if patients stop working within the 2 years of followup.
Logistic regression analysis of determinants for changing (starting and stopping) work participation after 2 years of tumor necrosis factor inhibitor (TNFi) treatment.
DISCUSSION
The objectives of our study were to establish the determinants of WP at the start of TNFi treatment, and determinants of starting and stopping work after 2 years of treatment with TNFi. The results show that better functionality and male sex were positively associated with WP at the start of TNFi treatment. Starting work was associated with a better functionality, as well as being RF-positive and of younger age. Further, a worse functionality at baseline, comorbidities, and less improvement in the HAQ-DI score are positively associated with stopping work.
Some results of our study are comparable to other studies that focus on determinants of WP in patients with RA. Our results were in accordance with the results of Young, et al26. They concluded that manual work, the HAQ-DI, ESR, sex, age, and radiological erosions are predictors of work disability, although the study by Young, et al26 was performed among patients with early RA. The study by Eberhardt, et al17 reports HAQ-DI as the single prognostic factor with strong predictive value of work disability in patients with early RA followed for 15 years. Also, the studies of Sokka, et al16 and Puolakka, et al25 concluded that functionality was a significant determinant. In contrast to our finding, the study by Wallenius, et al39 concludes that females with RA have a 4-fold increased risk of work disability compared to men. But it should be mentioned that the study was performed on patients younger than 45 years, while our study describes a substantially older population. Previous studies show that the disease activity of patients with RA taking TNFi treatment decreases most in the first 6 months of the treatment. After that, on average, the disease activity stays at the same level40. Therefore, it is plausible that the WP results are also sustainable in the long term. However, if other, non-disease-related aspects change, such as the economy and thus the unemployment rates, WP in patients with RA will likely change too. Like the study by Rantalaiho, et al41, the general unemployment percentages in the Netherlands also decreased from 2005 until 2008. However, they increased from 2001 until 2005 and from 2008 until 201242. Our study contains data from 2003 until June 2012, which indicate the same trend as in the general population of the Netherlands. The economic situation is expected to be associated with the WP of patients with RA.
Consideration should be given to the limitations of our study. One is the low proportion of variance explained by the presented prediction models; there should be other determinants associated with WP than the clinical determinants that were measured in this study. Besides the effects of RA and the effectiveness of treatment, WP can be influenced by factors external to the medical field, such as changes in the economic environment, women’s expanded involvement in the workplace, and the availability of retirement and disability allowances. Also, working conditions, emotional challenges, interpersonal issues affecting work and family life, and the meaning of work influence the continuation of work43. In our study, the reasons given for stopping work were given only by the patients who receive a disability allowance (patients unable to work because of their disease), and who can get an early retirement pension. However, for the patients who were working at baseline but had no work or allowance at 2 years, the reason for stopping work is unknown. Therefore, reasons other than RA could cause someone to stop working, such as their economic situation. The kind of work patients do is also unknown. Logically, it is more difficult to keep working or start working if patients have a physical job than if they work in an office44,45. Because patients with RA in our study are expected to be the same as the general patients with RA who are treated with TNFi, it is plausible that these results are representative for other patients with RA of working age taking TNFi treatment. However, our results should be carefully generalized to other countries. The Netherlands is a Western country where the social security system provides disability allowance and retirement pensions, people have health insurance even if they have no paid job, and it is very common for women to work outside the home. These facts could be different in other countries, and so the motivation or opportunities to work would be different16,46. In countries with low gross domestic product, TNF treatment is not always available and patients keep working with worse clinical status measures than in countries with high gross domestic product, like the Netherlands. It would be expected that the WP rate in countries with low gross domestic is somewhat higher.
The only determinant in our study as well as in many other studies16,17,18,23,25 that has an effect on WP and can be influenced is the HAQ-DI. Disease-related factors that influence patients’ functionality are inflammation and damage of the joints. Therefore, patients should be treated early to prevent permanent destruction to the joints and consequently to have better functionality at the start of the TNFi treatment. This can also lead to small improvements in WP outcomes, which can positively influence the cost-effectiveness ratio of TNFi. Age and comorbidities are more difficult to influence, although if RA care will be more treat-to-target, patients receive TNFi treatments earlier and thus at a younger age. Educating patients about a healthy lifestyle and screening for cardiovascular disease could prevent its occurrence and that of comorbidities such as diabetes. The chances of starting work can be improved and the chances of stopping work can be decreased.
Acknowledgments
The authors thank all of the research nurses and rheumatologists from the 13 departments of rheumatology from the Netherlands for their participation in the data collection. We acknowledge Thea van Gaalen, Lia Schalkwijk, and Marjon de Lange-Brandt for data processing.
Footnotes
-
Funding for the data collection for the DREAM cohort was obtained from the Dutch affiliates of Pfizer Pharmaceuticals, Abbott Pharmaceuticals, Roche Pharmaceuticals, UCB Pharma, and Bristol-Myers Squibb. Funding for these specific analyses was obtained from the Dutch affiliate of Abbott Pharmaceuticals.
- Accepted for publication February 20, 2014.








{kind=link}