

Abstract
Objective. To determine the risk factors for permanent visual loss (PVL) in patients with biopsy-proven giant cell arteritis (GCA) and the usefulness of the factors in clinical practice.
Methods. From 1976 through 2015, the clinical charts and laboratory results of 339 patients with biopsy-proven GCA were recorded prospectively at the time of diagnosis. We used multivariable logistic regression analysis to determine which of 24 pretreatment characteristics were associated with PVL.
Results. Visual ischemic manifestations occurred in 108 patients, including PVL in 53 (16%), bilaterally in 15 patients (28%). The independent predictors associated with an increased risk of PVL were age (OR 1.06, 95% CI 1.01–1.12, p = 0.01), a history of transient visual ischemic symptoms (OR 2.62, 95% CI 1.29–5.29, p < 0.01), and jaw claudication (OR 2.11, 95% CI 1.09–4.10, p = 0.03). The presence of fever (OR 0.30, 95% CI 0.14–0.64, p < 0.01) and rheumatic symptoms (OR 0.23, 95% CI 0.10–0.57, p = 0.001) were associated with a markedly reduced risk of developing visual loss (3.7% if features were both present). No laboratory variables were independently associated with PVL.
Conclusion. The visual ischemic risk of untreated GCA can be readily estimated upon simple clinical findings, but not laboratory variables. However, we did not identify a subgroup of patients carrying no risk of developing visual loss. Glucocorticoid treatment remains, therefore, urgent for any patient with a high clinical suspicion index.
Giant cell arteritis (GCA) is the most frequent systemic vasculitis in the elderly1. Its main complication is permanent visual loss (PVL), which occurs in 10%–20% of the cases2. During the last 2 decades, large retrospective series have pointed out a number of risk factors for visual impairment, notably a history of amaurosis fugax3,4,5, jaw claudication3,4,5,6,7,8, lack of constitutional syndrome4,6,9,10,11,12, presence of blood thrombocytosis4,7,13, and a lower inflammatory response4,9,14,15. However, some of these studies have included, for statistical purposes, patients with either transient or PVL6,8,10, while other studies have pooled permanent visual and cerebrovascular events9,11,12,15. Interestingly, Cid, et al identified the clinical (fever, weight loss) and laboratory [erythrocyte sedimentation rate (ESR) ≥ 85 mm/h, hemoglobin < 11 gm/dl] inflammatory status as highly potent means of discriminating patients with GCA with a very low visual ischemic risk9. However, a cross validation of this model on other large cohorts of patients with GCA has not been performed.
In a previous study including 174 (147 biopsy-proven) patients with GCA, we showed that a history of transient visual ischemic symptoms (TVIS) and a higher platelet count were main independent predictors associated with PVL, while the presence of constitutional signs, polymyalgia rheumatica (PMR), and a higher C-reactive protein (CRP) level were associated with a reduced risk4. The aims of our present study were to reinvestigate the risk factors for PVL in a much larger sample of biopsy-proven patients diagnosed and followed at a single institution, and to search for a simple model that could help physicians to distinguish patients at high risk from those at low risk of developing visual damage.
MATERIALS AND METHODS
Patients and data collection
We analyzed the clinical, laboratory, and pathologic features, treatments, and outcomes of 339 consecutive patients with biopsy-proven GCA who were referred to the Internal Medicine Department of a tertiary care teaching hospital from January 1976 through May 2015. Biopsy-negative cases (117 patients) and nonverified cases (6 failures of biopsy procedure) were excluded from our study. The cohort, albeit large (462 patients in all), cannot be regarded as population-based. Our catchment area, the Limousin region, has a population of about 750,000 people, including 30% over the age of 55 years. Assuming that GCA onset before age 55 is exceedingly rare and the incidence of GCA in France may be close to 10/105 persons over age 50 per year, the observed number of cases compared with the expected during the study period may be 50%. The biopsy-proven inception cohort consisted of 147 patients (recruited from 1976 through 2000) from the 2001 study4, 14 patients excluded from that study because they did not have a platelet count before corticosteroid treatment, and 178 patients recruited between 2001 and April 2015. Ninety-three percent of the patients were recruited before steroid treatment; the remaining cases already being treated for < 1 month at the time of admission. The diagnosis of GCA was pathologically established according to currently accepted criteria16. In addition, all the patients but 3 (2 large vessel vasculitides and 1 occult GCA with sudden blindness) fulfilled the criteria from the American College of Rheumatology17. Pretreatment clinical, laboratory, and pathological data were recorded prospectively at the time of first admittance to our department by a senior internist using a specifically designed, comprehensive questionnaire that included a precise history and 176 items4. The questionnaire was completed in 96% of the cases. Data from patients recruited since 1990 were stored in real time in a computerized file and regularly updated by one of the authors (EL). Individual questionnaires from 87 patients recruited before 1990 were initially stored in a personal library and then transferred to the computerized file. This way, nearly all the patients recruited in the department during the 39-year period were included in the inception cohort.
Clinical definitions
The temporal arteries were considered abnormal on examination if there were decreased or absent pulses, or nodules, redness, thickening, or tenderness in at least 1 artery. Constitutional syndrome was defined by a temperature ≥ 38°C for at least 1 week, severe asthenia, and/or weight loss > 5%. Jaw claudication was considered present if the patient reported recurring pain upon chewing, which resolved after chewing stopped, or trismus. PMR and nonerosive, seronegative peripheral arthritis formed parts of the rheumatic spectrum of GCA. PMR was defined by the presence for at least 2 weeks of moderate to severe pain and morning stiffness lasting more than 30 min in at least 2 of neck, shoulders, and pelvic girdles. Upper limb artery involvement was defined on a clinical basis (bruits over axillary/humeral arteries, decreased radial pulses, ischemic arm pain) with confirmation on Doppler-echography studies and/or angiography. The occult form of temporal arteritis consisted of a visual ischemic accident in an otherwise asymptomatic patient4,18. Inflammatory markers, blood counts, and hepatic tests were only recorded in glucocorticoid-naive patients. Since 1991, the initial workup also consisted of a measurement of immunoglobulin G anticardiolipin antibodies. To avoid false-negative results, we excluded samples taken after 2 days of glucocorticoid treatment19.
All the patients but 7 were treated using standardized protocols. Prednisone was given at 0.6 to 1 mg/kg according to clinical severity. Two hundred twenty-three patients (67%) without ischemic manifestations received prednisone 0.6–0.8 mg/kg/day until the patients became symptom-free and the CRP level fell below 5 mg/l. The prednisone dose was then progressively tapered down to 0.35 mg/kg within 4 to 6 weeks. One hundred nine patients (33%) with ischemic manifestations or threat to their vision (transient ischemic symptoms, abnormal fundus, or abnormal ophthalmic artery flow on Doppler studies) initially received prednisone 0.9 to 1 mg/kg, preceded in 82 by pulse methylprednisolone, then similarly tapered down. In addition, dapsone (75–100 mg/day) was given to 21 unselected patients as a first-line glucocorticoid-sparing agent20, while 30 other patients were included in various prospective, ongoing multicenter studies.
Visual ischemic manifestations
Only visual events that occurred before therapy or within the first 2 weeks of its initiation were included in our analysis. Ischemic visual symptoms included transient symptoms and PVL4. Amaurosis fugax lasting from seconds to a few minutes, intermittent blurred vision, or transient diplopia were considered transient ischemic visual symptoms. PVL, which was always confirmed by a staff ophthalmologist, included anterior ischemic optic neuropathy (AION), central retinal artery occlusion (CRAO), and posterior ischemic optic neuropathy (PION), while isolated eye nerve palsies were not regarded as visual ischemic manifestations.
Statistical analyses
Continuous variables were expressed as mean ± SD, while categorical variables were expressed as frequencies and percentages. Checking normality of the distribution of quantitative variables was performed using the Shapiro-Wilk method. Comparisons of continuous variables were performed using the Student t test. Proportions were analyzed using the chi-square or Fisher’s exact test. To identify the best predictors of PVL, multivariate analysis was performed with multiple logistic regression models. Multivariate analysis compared patients with and without permanent visual ischemic manifestations (patients with isolated TVIS were included in the group without visual loss). To reduce residual confounding, crude and age-adjusted and sex-adjusted models for potential predictors of visual loss were built, including variables with a p value < 0.2. The significance threshold selected for the final model was set at 0.05. In an attempt to define a group of patients without any visual damage, we applied to our patients a variant of the model empirically defined by Cid, et al9. We defined fever and weight loss by a temperature of ≥ 38°C for at least 1 week (instead of > 37°C) and at least 5% loss (instead of > 5 kg), respectively. Calculations were performed using the statistical package SAS, release 9.1.3 (SAS Institute).
RESULTS
Main characteristics of the series
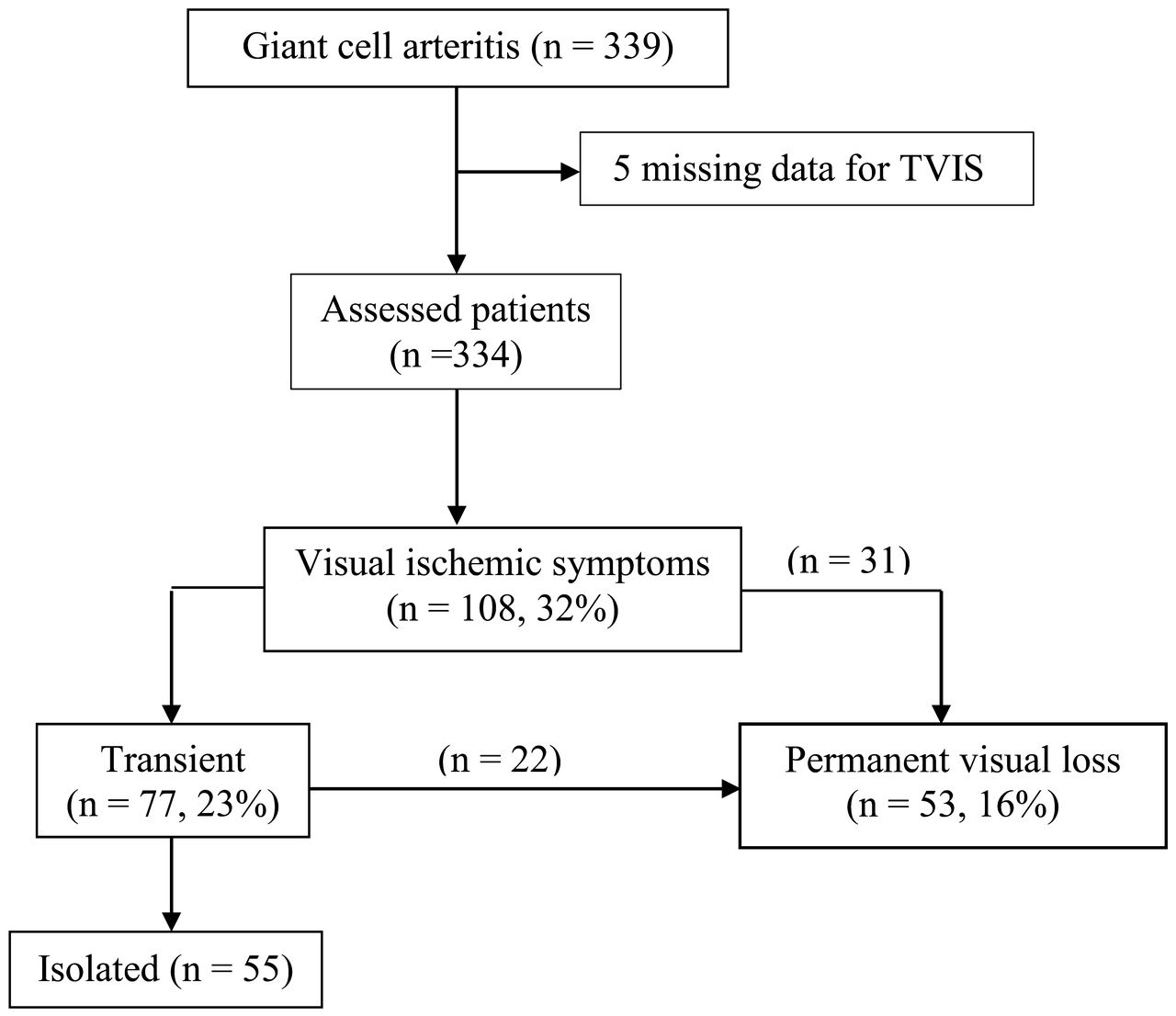
The mean patients’ age was 75.6 years (range 51–94 yrs); 65% were women. All the patients but 3 had GCA confirmed by a positive temporal artery biopsy; the remainders were biopsy-proven at other sites (thoracic aorta, femoral artery). Visual ischemic manifestations were recorded in 108 of 334 assessable patients (32%; Figure 1). A history of TVIS was elicited from 77 of the patients including amaurosis fugax from 54 (16%). PVL occurred in 53 patients (16%). Fifteen patients (28%) developed bilateral PVL, synchronously or sequentially. Whereas most ischemic events occurred before treatment, blindness occurred in 5 patients shortly after glucocorticoid treatment was started. All these patients had unilateral blindness prior to treatment and 3 became completely blind because of AION in the fellow eye within the first 9 days of treatment, despite pulse methylprednisolone. None of 286 patients without permanent visual impairment at diagnosis developed subsequent visual loss once treatment was initiated. TVIS, mainly amaurosis fugax, heralded PVL in 22 (41.5%) of the patients with permanent loss. Of 68 permanently affected eyes, 51 showed isolated AION, 8 showed isolated CRAO, 2 showed both involvements, and 7 showed both normal fundus and retinal arteriography, suggesting PION. Rheumatic symptoms were recorded in 113 patients (35%), including PMR in 84, peripheral synovitis in 15, and both features in 15. While fever was recorded in 149 patients (45%), constitutional symptoms (or isolated raised inflammatory markers) were the only features of GCA in 34 patients (10%). Table 1 lists the main characteristics of the series and the results of a univariate analysis comparing patients according to permanent visual status.
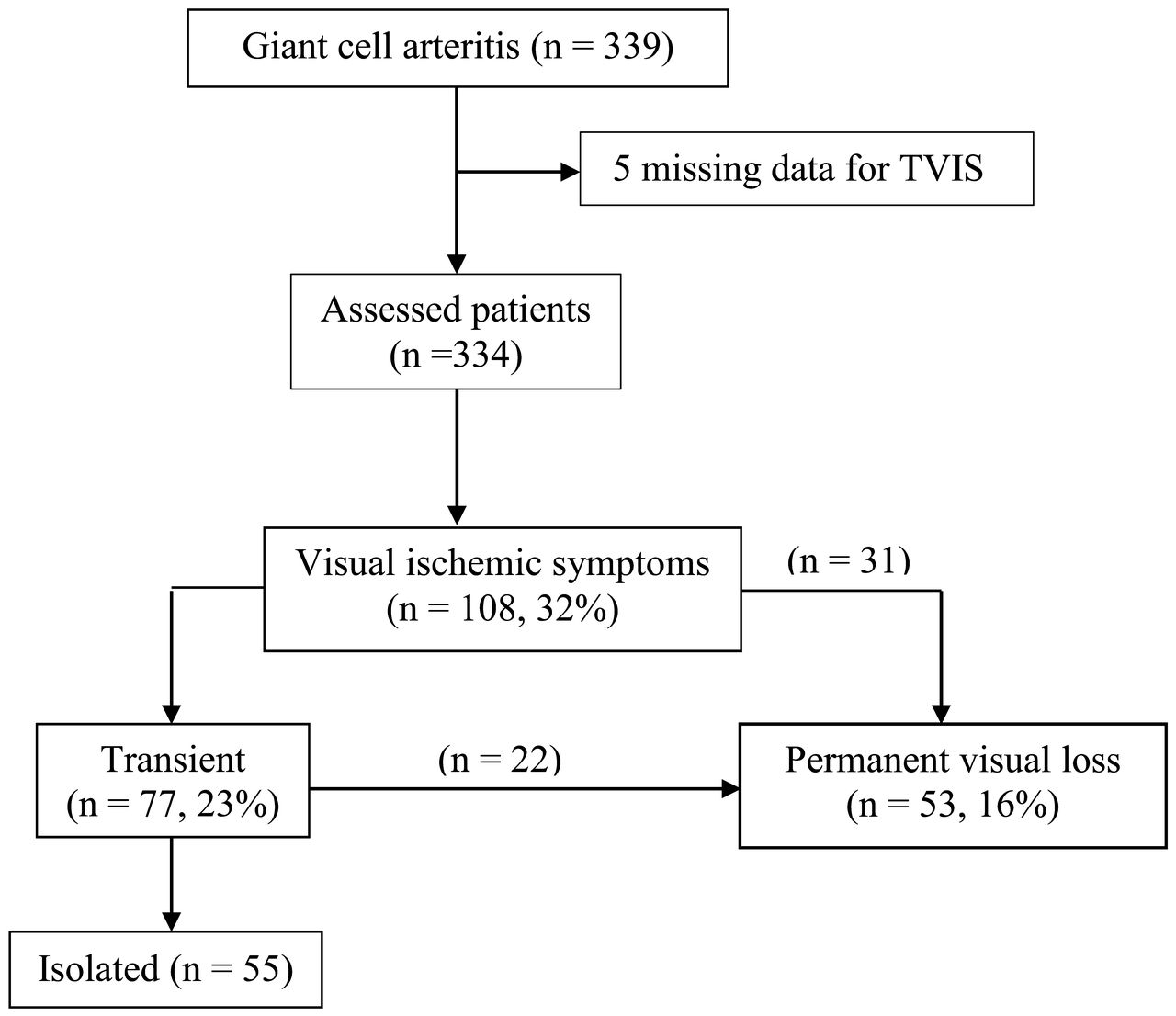
Frequency of occurrence of TVIS and its relationship to permanent visual loss in patients with giant cell arteritis. TVIS: transient visual ischemic symptoms.
Comparison of various clinical and laboratory variables in patients with GCA with PVL and without (univariate analysis). Values are n (%) unless otherwise specified.
Predictors of PVL
In a crude global model, jaw claudication and fever were predictive variables of PVL using logistic regression (Table 2). In the final model, only age, amaurosis fugax, and jaw claudication were independent risk factors for PVL, whereas rheumatic symptoms and fever were associated with a markedly reduced risk (Table 3). A borderline significant negative association between visual loss and male sex was also found (OR 0.53, 95% CI 0.25–1.10, p = 0.09). The mean blood platelet level (determined before treatment in 308 patients) was higher in patients with PVL compared with patients without (489 ± 140 × 109/l vs 444 ± 161 × 109/l, p = 0.02), but was not independently associated with the visual risk (OR 1, p = 0.743). Of the 179 patients with thrombocytosis (platelet count > 400 × 109/l), 31 (17.3%) developed PVL compared with 13 (10%) of those without thrombocytosis (p = 0.15). Of patients with a platelet count below 400 × 109/l, 5.4% developed PVL, as did those with a platelet count above 700 × 109/l (5.2%).
Predictive variables of permanent visual loss using logistic regression: crude global model and model adjusted for age and sex*.
Predictive variables of permanent visual loss using logistic regression (final model*) adjusted for age.
We also investigated whether the model proposed in 1998 by Cid, et al to estimate the visual/cerebrovascular risk9 applied to our patients. Those investigators defined clinical inflammatory status and biologic inflammatory status in patients with GCA empirically (clinical: fever and weight loss; biologic: ESR ≥ 85 mm/h and hemoglobin < 11.0 g/dl). The risk was greatly reduced among patients with either a clinical (OR 0.177, 95% CI 0.052–0.605) or a biologic (OR 0.226, 95% CI 0.076–0.675) inflammatory reaction. No patients with both a clinical and a biologic response developed ischemic events9. According to this model, 307 of our patients were fully assessable. The presence of at least 1 variable was associated with a significantly reduced rate of visual loss, while the combination of both variables yield a more than 4-fold reduction (Table 4).
Results of the application of the model developed by Cid, et al9 to determine the risk of visual loss in patients with giant cell arteritis. Values are n (%) unless otherwise specified.
DISCUSSION
In our large sample of patients with biopsy-proven GCA, 32% had visual ischemic symptoms and 16% had PVL, which was bilateral in 28% of the cases. The rate of irreversible sight damage is similar to those published previously3,4,9,10,12,13,21, as is the rate of bilateral blindness, about 30%3,4,6,10,13,22. In a recent report on a population-based cohort of 204 patients, there was a lower incidence of ischemic optic neuropathy in the 1980–2004 cohort versus 1950–1979 (15% vs 6%, p = 0.03)8. On the contrary, despite a progressive increase in the number of new cases diagnosed, we did not observe such a decline in the rate of irreversible visual loss over a 40-year study period. Likewise, in a defined population in northwestern Spain, no significant change in the proportion of patients with visual manifestations was recorded during an 18-year study period10. Visual loss remains, therefore, a frequent complication of GCA in western European populations.
As already seen in our first study4 and in other studies22,23, these complications occurred before treatment in most patients. Signs and symptoms suggesting cranial arteritis heralded blindness for weeks (7 in average) in a majority of patients. In fact, amaurosis occurring in the early course, or even as an initial manifestation, of GCA was only seen in one-fifth of the cases. Further, the start of steroid treatment before any permanent loss of vision had occurred was associated with an impressive decrease in the rate of subsequent severe visual events: no severe visual events in the 286 patients in our present study, and 1 in the 204 biopsy-verified patients in the study by Aiello, el al21. In this respect, our finding that a longer delay in diagnosis is not associated with a higher rate of visual loss may be intriguing. The recruitment of a significant proportion of patients with masked GCA in our inception cohort might partly explain the discrepancy. In this subset of GCA, diagnosis is often delayed but the visual risk is very low24. Overall, accumulated data suggest that more rapid recognition of GCA by primary care physicians might reduce the rate of irreversible blindness.
In a previous study, we found that advanced age (≥ 80 yrs) was associated with a poorer visual outcome in GCA25. In our present study, contrary to our first study4, age was independently associated with visual loss. Moreover, 24 (23%) of the patients 80 years of age and more had PVL including 6 with bilateral blindness. Other investigators found a borderline6,13 or significant26 association between the mean age and visual loss, the highest risk being seen in patients aged 80 to 90 years13. Therefore, because age appears to be a predictor of poorer visual prognosis, we do not recommend the use of lower initial doses of steroids in very elderly patients with GCA, despite the risk of side effects4. We found that male sex was marginally associated with a reduced risk of visual loss. This result confirms previous observations27,28 but does not negate the possibility that being male is linked to GCA-induced blindness in non-white populations11,29.
Our study confirms that TVIS and jaw claudication are strong predictors of PVL caused by GCA. This is in agreement with many other studies3,4,5,6,8,9,10,11,21. Among various forms of TVIS, amaurosis fugax is the most frequently reported and the most ominous, preceding PVL from a few hours to several weeks in 30%–50% of the patients with permanent blindness4,9,10,11,21. Notoriously, of our 22 patients in whom transient visual symptoms heralded permanent loss, 20 (91%) reported mainly or solely amaurosis fugax. Jaw claudication is a major symptom to elicit from elderly patients with persisting headache because it is both associated with a high-positive likelihood of proven temporal arteritis in patients referred for temporal artery biopsy30 and a factor in higher risk of PVL in some studies8,11,21. We agree with González-Gay, et al that when GCA is suspected and the patient reports either transient visual loss or jaw claudication, high-dose corticosteroids should be started urgently without waiting for the results of a temporal artery biopsy3.
In our first study, no patients with PVL had concurrent upper limb involvement4. In our present study, upper limb involvement was not an independent negative predictor for visual loss, despite a low rate of blindness (5.6%) in this subset of patients. For Schmidt, et al, upper limb involvement was the only variable associated with a reduced risk of impaired vision31. Likewise, a comparative study of 120 large-vessel GCA and 212 cranial GCA found a smaller proportion (4% vs 11%, p = 0.035) of vision loss in the former group32. In fact, large vessel GCA often occurs without involvement of the cranial arteries and has been associated, in 1 large-scale study, with higher concentrations of interleukin 2 gene transcripts in arterial tissue and overrepresentation of the HLA-DRB1*0404 allele compared with classic cranial arteritis33. This particular pattern might account for a reduced visual risk in large vessel GCA. PMR has been shown to be a protective factor4,11. Our study confirms this, although 9 patients had both rheumatic involvement and visual loss, simultaneously or sequentially. Of note, all of these patients but 1 also expressed concurrently typical cranial symptoms including jaw claudication and abnormal temporal arteries on examination. Patients who show prominent polymyalgia symptoms after a self-limited course of dismissed mild cranial symptoms may be at very low risk of developing ischemic events34; on the contrary, the visual risk may increase notably in patients with PMR who later develop cranial symptoms11,34,35. In our cohort, neither the presence of at least 1 among classic cardiovascular risk factor such as hypertension, diabetes, and dyslipidemia nor a history of complicated atherosclerosis was associated with an increased risk of visual damage in patients with GCA. There is no consensus on whether the presence of traditional atherosclerosis risk factors and/or a history of ischemic heart disease or stroke at the time of diagnosis of GCA influence the risk of severe visual ischemic events11,12,36, deserving further investigation.
In our current study, fever was independently associated with a markedly reduced risk of permanent visual disturbances, whereas laboratory markers were not. The protective involvement of fever was first mentioned by Cid, et al9 and often confirmed later3,7,11. This is not surprising because fever, along with fatigue and weight loss, is a hallmark of systemic (or masked) temporal arteritis. Such forms of GCA do not carry a visual risk, unless cranial symptoms occur later24. In our present study, of 10 patients with fever and visual loss, only 2 denied jaw claudication and additionally had normal temporal artery on examination. Most studies found a negative association between the intensity of blood acute-phase reaction, i.e., the mean levels of ESR and CRP, and the visual ischemic risk3,4,9,10,13,14. For Lopez-Diaz, et al, an ESR between 70 and 100 mm/h was the best predictor of visual ischemic complications37. Moreover, anemia appeared to be protective in several studies9,10,15. Although in our current study no blood marker was independently associated with the risk of visual loss, the presence of a clinical and biologic inflammatory response, as proposed by Cid, et al9, delineated a subgroup at very low risk of developing such complications. The mechanisms by which a strong inflammatory response plays a protective role against severe ischemic manifestations of GCA are still unknown, but could rely on different anatomical, clinical, and cytokine patterns according to its intensity8. Finally, in disagreement with our previous study but consistent with several other studies9,10,11, thrombocytosis was not an independent risk factor for visual loss, although the mean platelet count and the frequency of thrombocytosis were higher in our patients with permanent sight impairment compared with other patients. The observed discrepancy between studies can be best explained by a much larger sample size and a larger proportion of systemic forms of the disease in the latter study. In this subset of GCA, the platelet count can rise spuriously, owing to a greater severity of the inflammatory response24.
Main study limitations include a substantial amount of missing data for several laboratory variables, lack of assessment of HLA-DR4 polymorphisms, and lack of precise data on continuous platelet inhibition treatment. Moreover, our inception cohort is not population-based, so that our results may not be fully applicable to other GCA populations. Nevertheless, our study on a large sample of biopsy-proven GCA investigated and treated homogeneously confirms that clinical features such as transient visual loss, jaw claudication, PMR, and fever strongly influence the visual ischemic risk. On the contrary, although the presence of an acute-phase reaction in an elderly patient with persistent headache strongly suggests temporal arteritis, its intensity might be a poorly reliable means of evaluating the risk of impending ischemic blindness. Currently, glucocorticoid treatment remains urgent for any patient with strongly suspected GCA because no subgroup of patients with zero risk of visual loss could be identified. Prospective, multicenter studies are needed to definitively confirm our findings and further delineate the main clinical patterns of GCA.
- Accepted for publication March 7, 2016.








{kind=link}