Article Text

Abstract
Objectives We compared the ability of antibodies against cyclic citrullinated peptides (anti-CCP2), against mutated citrullinated vimentin (anti-MCV) and against citrullinated fibrinogen (AhFibA) to predict 1 year rapid radiographic progression (RRP; total Sharp score variation ≥5 points), in early rheumatoid arthritis (RA).
Methods We analysed 566 patients from the ESPOIR cohort with early RA fulfilling the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) criteria at year 1. We assayed the 3 anticitrullinated peptide antibodies (ACPA) tests on baseline sera. We compared the performance of these 3 ACPA tests to predict first-year RRP, by comparing areas under the receiver operating characteristic curves (ROCs). We assessed the 1 year RRP risk by ACPA titres. We used a logistic multivariate regression to analyse RRP risk in terms either of ACPA positivity or titre: high (>3 times the N cut-off) and low (1 to 3N).
Results 145 patients displayed RRP. Areas under the ROCs were similar (0.60) for the 3 tests. High ACPA titres were associated with 1 year RRP, whatever the test was, and with similar ORs. Low+ anti-MCV titres were not associated with 1-year RRP, whereas low+ anti-CCP2 titres (p=0.0226) and low+ AhFibA titres (p=0.0332) were significantly associated. In multivariate analysis, 1 year RRP was associated with anti-CCP2 positivity (p<0.0001), AhFibA positivity (p<0.0001) and high anti-MCV titres (p<0.0001).
Conclusions Anti-CCP2 antibodies and AhFibA were predictive of 1 year RRP in early RA whatever their titre was, whereas only high anti-MCV antibody titres were predictive, potentially making them more discriminant to predict 1 year RRP risk.
- Early Rheumatoid Arthritis
- Ant-CCP
- Autoimmunity
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Anticitrullinated peptide antibodies (ACPA) are among the best predictors of erosive rheumatoid arthritis (RA), but data concerning ACPA specificity and radiographic progression showed discrepancies.
What does this study add?
We showed that anticitrullinated fibrinogen antibodies (AhFibA) predict 1 year rapid radiographic progression as well as antibodies detected by anticyclic citrullinated peptide (anti-CCP2) test. We showed that antimutated citrullinated vimentin antibody (anti-MCV) titres were predictive of 1 year rapid radiographic progression.
How might this impact on clinical practice?
AhFibA test should be considered not only as a valuable test for RA diagnosis, but also for RA radiographic prognosis. Considering anti-MCV titres rather than their positivity is potentially discriminant to predict 1 year rapid radiographic progression.
Introduction
Anticitrullinated peptide antibodies (ACPA) are the most specific autoantibodies known as markers of rheumatoid arthritis (RA). In cohorts of early RA, ACPA are associated with increased clinical disease activity and progression of structural damage.1 ACPA have high weight in the final scoring system of the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) RA classification criteria for RA.2 This weight is modulated by the ACPA titre (negative, low and high), with increased risk of RA being associated with high titres.
Data concerning the link between the structural expression of RA and ACPA detected with various tests show discrepancies. In four works performed in early RA with various ACPA tests using different antigens, the link between ACPA and structural progression was variable.3–6 In the work of Fisher et al,3 radiographic progression (RRP) over 2 years was greater for ACPA-positive than for ACPA-negative patients; however, anti-CEP-1 antibodies (directed to citrullinated α-enolase) did not confer additional severity. In a study by Scherer et al,5 the structural damage progression over 5 years in ACPA-positive patients was not associated with any antibody to the six citrullinated peptides used as antigens (2 from vimentin, 2 from fibrinogen, 1 from α-enolase, 1 from myelin basic protein). The extent of the ACPA epitope directory analysed on these peptides did not modify the structural prognosis.
However, three studies considered antimutated citrullinated vimentin (anti-MCV) antibodies as an additional marker of structural severity.7–9 Montes et al9 found that patients with antibodies to the citrullinated vimentin peptide 60–75 show a higher prevalence of erosions than patients without, independently of their positivity for anticyclic citrullinated peptide (anti-CCP2) antibodies. Harre et al7 found that the presence of anti-MCV antibodies could increase osteoclastogenesis and bone resorption.
Our work compared ACPA assayed with three different tests. The anti-CCP2 antibodies were considered as the reference because of their wider usage. We evaluated the anti-MCV antibodies because of the supposed direct pro-erosive role of anticitrullinated vimentin antibodies.7 Lastly, we evaluated the anti-human citrullinated fibrinogen antibodies (AhFibA) since citrullinated fibrin is the main ACPA autoantigen in the synovial tissue of patients with RA.10 The 3 tests have shown similar value for the diagnosis of RA in early arthritis,11 but, to date, only a few studies have assessed their performance in terms of structural outcome and, moreover, they show some discrepancies.12–17
This work aimed to compare anti-CCP2 antibodies, anti-MCV antibodies and AhFibA, all assayed at baseline in the patients of the ESPOIR cohort, and to analyse their association with rapid RRP at 1 year.
Methods
Patients
Eight hundred and thirteen patients with suspected or confirmed diagnosis of early RA, referred to 1 of 14 regional centres, were included in the French ESPOIR cohort. The inclusion criteria of ESPOIR cohort were: age 18–70 years, more than two swollen joints for >6 weeks and <6 months, suspected or confirmed diagnosis of RA and not taking any disease-modifying antirheumatic drugs (DMARDs) or steroids except for <2 weeks before enrolment. We analysed data from 3 ACPA tests at baseline (anti-CCP2, anti-MCV, AhFibA) and from radiographic assessment at baseline and at 1 year, for 566 patients fulfilling the 2010 ACR/EULAR criteria at year 1. Patients were excluded from analysis because of 232 missing radiographs at baseline or year 1, 109 did not fulfil ACR/EULAR criteria and 115 had missing data for ACPA (crude counts; some patients had several missing data). All patients gave their written informed consent to the prospective follow-up study before inclusion. Further details concerning patients are provided in a previous publication.18
Clinical evaluation
For each patient, we collected data on age, sex, smoking, symptom duration, Disease Activity Score in 28 joints, patient and physician visual analogue scale score for global assessment, functional ability by Health Assessment Questionnaire-Disability Index and disease activity by the Simple Disease Activity Index.
Biological evaluation
ACPA tests were assessed at baseline. Anti-CCP2 (DiaSorin) and anti-MCV antibodies (Orgentec) were assayed in Montpellier or Paris centres. AhFibA were assayed in the Toulouse centre with an in-house ELISA.11 For these ACPA tests, we used the positivity threshold (N) corresponding to the 95% diagnostic specificity: anti-CCP2 >25 U/mL, anti-MCV >20 UA/mL, AhFibA >0.056 AU. ACPA tests were also assessed at the 98% diagnostic specificity threshold: 40 U/mL for anti-CCP2, 35 UA/mL for anti-MCV and 0.119 AU for AhFibA. Moreover, the anti-CCP2 test was assessed at a previously validated cut-off: 50 U/mL.11 Over the cut-off sera were considered positive. Considering the weight of ACPA titres in the 2010 ACR/EULAR criteria, we assessed the antibody titres, classified as high positive if >3 times the cut-off (3N), and low positive if 1 to 3 times the cut-off.2 IgM rheumatoid factor (RF) (Menarini Diagnostics) was considered positive if >9 UI/mL. HLA-DRB1 4-digit typing and subtyping was performed in a single laboratory (Immunology laboratory, CHU Montpellier, France) using a PCR-based method. Erythrocyte sedimentation rate and C reactive protein (CRP) level were measured at baseline, then at each visit in each centre.
Radiographic evaluation
Radiographs of hands (anteroposterior view) and feet (anteroposterior and oblique views) were performed at inclusion and at 1 year. All radiographs were evaluated blinded by a single reader (GT, CHU Brest) by the van der Heijde-modified Sharp score. Results were expressed as total van der Heijde-modified Sharp score (mTSS). Intra-reader correlation coefficient was 0.97. The smallest detectable change was estimated at 1 point. RRP was defined as an increase in the mTSS ≥5 points per year.19 In this study, 145 patients displayed RRP.
Statistical analysis
The primary end point was to compare the performance of the 3 ACPA tests to predict first-year RRP by comparing areas under the receiver operating characteristic curves (AUC). Secondary end points were (1) to assess the 1 year RRP risk linked to the baseline ACPA titres, and (2) to further analyse the 1 year RRP risk by multivariate analysis including ACPA positivity and high ACPA titres if associated on univariate analysis. For descriptive analysis, continuous quantitative data with normal distribution are expressed as mean+SD and with non-normal distribution as median+IQR. One-year RRP was compared by autoantibody titres in terms of class (negative, low and high) by χ2 test. We modelled 1 year RRP risk by backward logistic multivariate regression, with 1 model for each test. The covariates tested included age, gender, duration of disease course before inclusion, smoking consumption, clinical centre, presence of erosions at inclusion, presence of the HLA-DRB1 shared epitope (SE) and ACPA, RF and CRP positivity. The use of steroids, or synthetic or biological DMARDs (within the first year) was included in the model. Covariates were selected if associated on univariate analysis (α=20%). Performance of the models was compared by area of the receiver operating characteristic curve analysis for each model. p Value <0.05 was considered statistically significant, with a 95% CI.
Further details concerning Methods section are provided in a previous publication.18
Results
Characteristics of patients with RA
We analysed data from 566 patients with early RA, having a complete biological and radiographic set of data. The main characteristics of patients are shown in table 1. Three hundred and thirty-three patients were positive for at least one of the three ACPA tests, 2 were anti-CCP2+/anti-MCV−/AhFibA−, 32 were anti-CCP2−/anti-MCV+/AhFibA− and 25 were anti-CCP2−/anti-MCV−/AhFibA+ (see online supplementary table S1). Three hundred and seven patients were positive for RF and 145 showed 1 year RRP as defined above. Serological data concerning the 98% diagnostic specificity thresholds and previously validated anti-CCP2 threshold are available in online supplementary table S2.
Demographic, biological and radiographic data for the patients with early rheumatoid arthritis
RRP risk at 1 year by positivity of ACPA
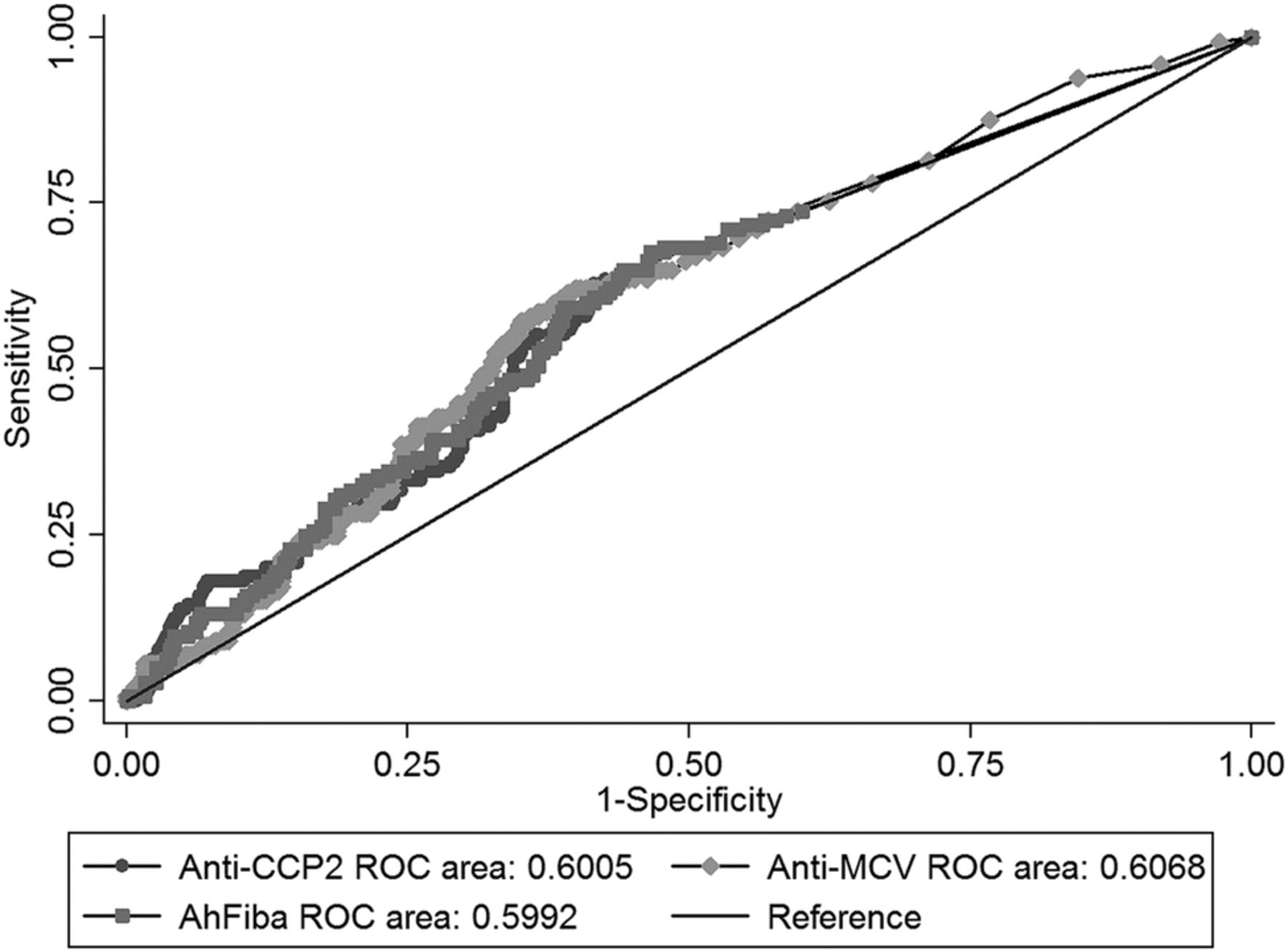
The AUCs for anti-CCP2, anti-MCV and AhFibA antibodies were similar, and matched with modest performance: respectively, 0.601 (95% CI 0.550 to 0.651), 0.607 (95% CI 0.555 to 0.659) and 0.599 (95% CI 0.547 to 0.651). No differences were found among the tests (p=0.87; figure 1).
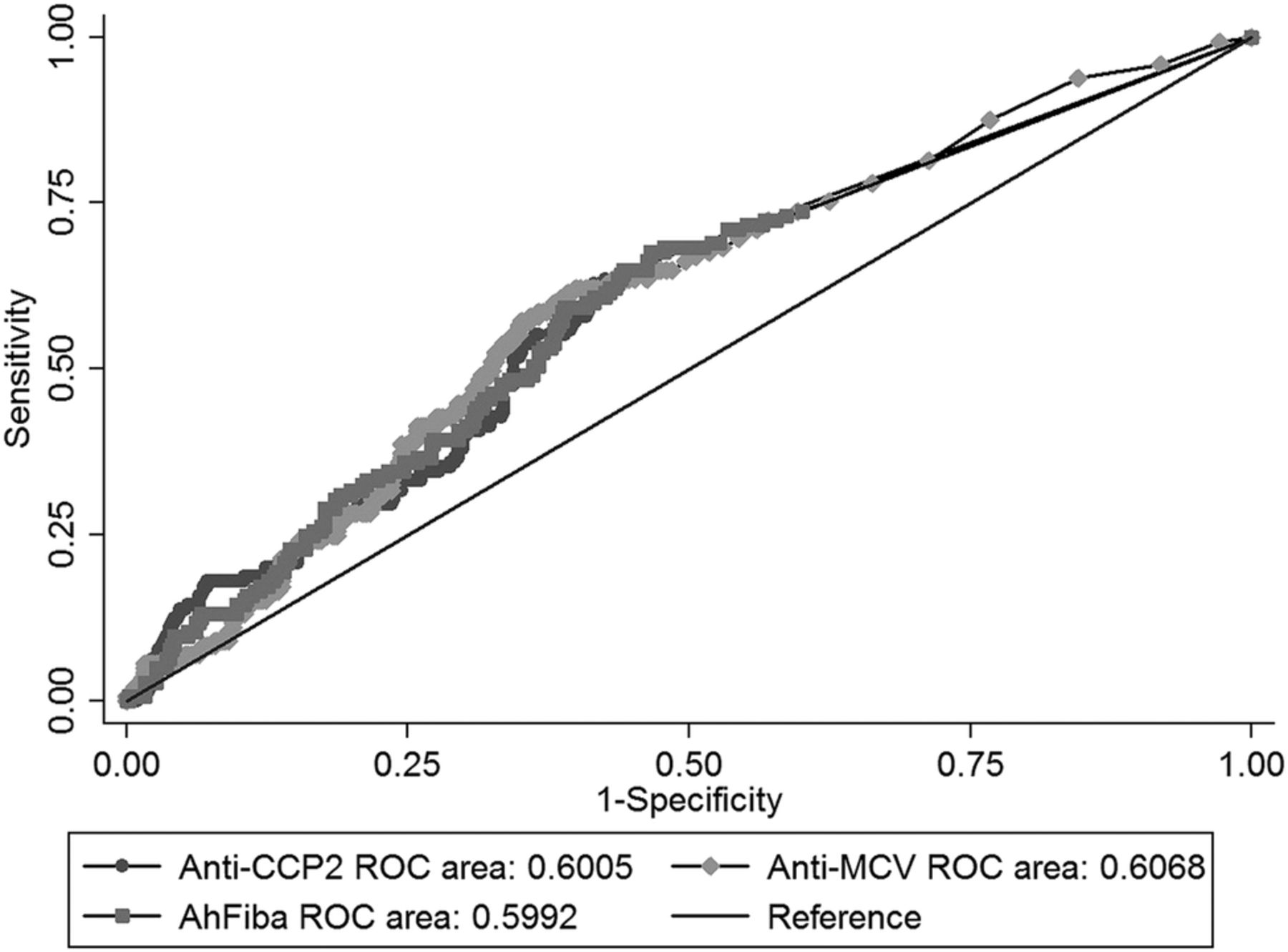
Receiver operating characteristic (ROC) curves: rapid radiographic progression prognosis by anticyclic citrullinated peptides generation 2 antibodies (anti-CCP2), antimutated citrullinated vimentine antibodies (anti-MCV) and antihuman citrullinated fibrinogen antibodies (AhFibA) tests. ROC curves built on the ability of each test (for anti-CCP2, anti-MCV and AhFibA) to predict 1-year rapid radiographic progression. Area under the curve values are expressed as continuous variables.
Predictive values of these tests were also similar (see online supplementary table S3).
RRP risk at 1 year by baseline ACPA titres
Patients with high baseline ACPA titres (>3N) showed increased risk of RRP regardless of the test (table 2). Low anti-CCP2 and AhFibA titres were associated with a significant increase in 1 year RRP, unlike low anti-MCV. Low and high anti-CCP2 and AhFibA titres showed similar performance to predict 1 year RRP. When these two tests were positive, about one-third of patients showed 1 year RRP.
One-year RRP and baseline ACPA titres (anti-CCP2, anti-MCV, AhFibA)
High anti-MCV antibodies titres were associated with an increase in 1 year RRP with a risk similar to that given by high anti-CCP2 or AhFibA titres. Unlike patients with high anti-MCV titres or those positive for the other two tests, only 13.7% of the patients with low anti-MCV titres showed RRP. These results remained similar with other positivity thresholds (see online supplementary table S4).
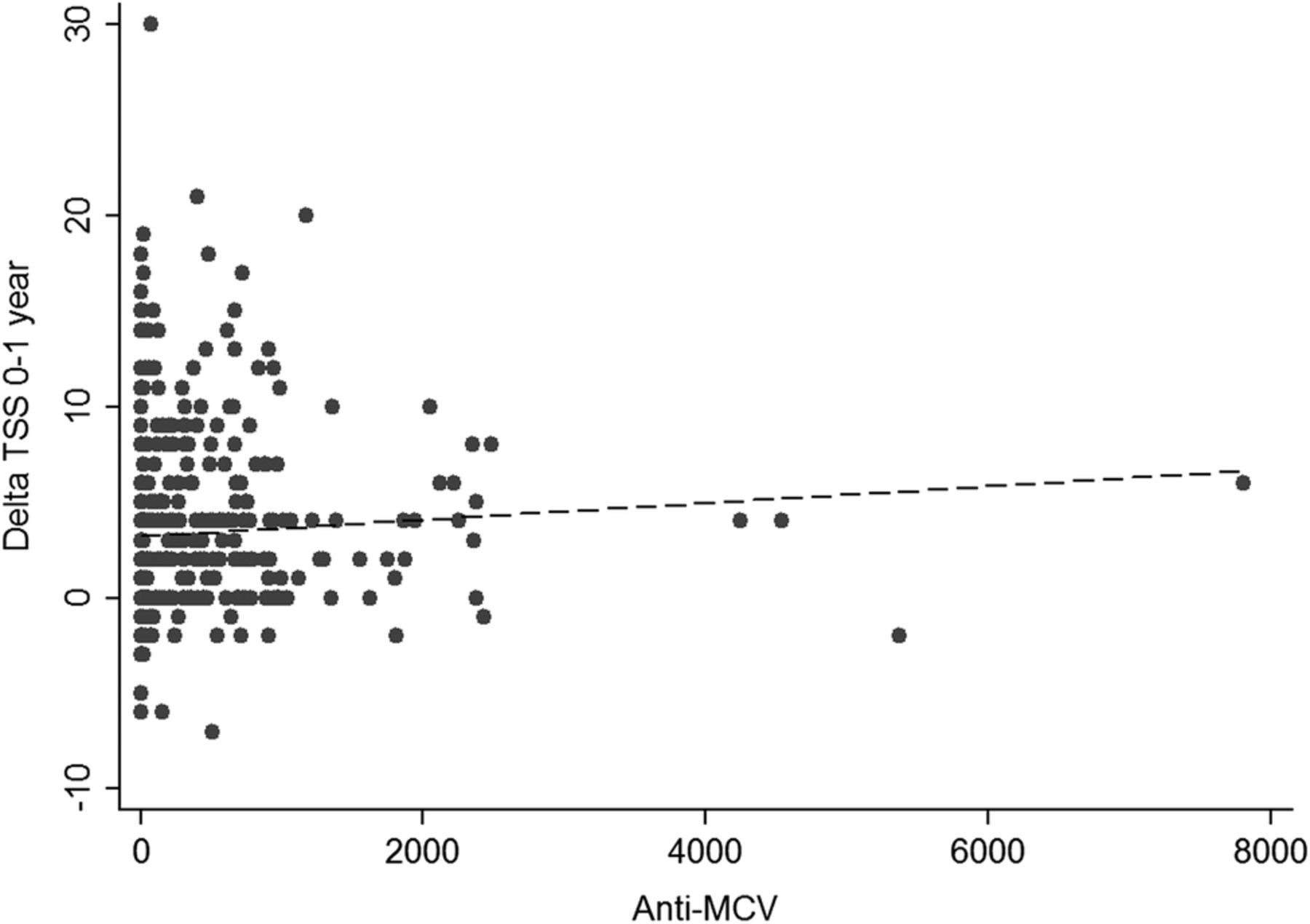
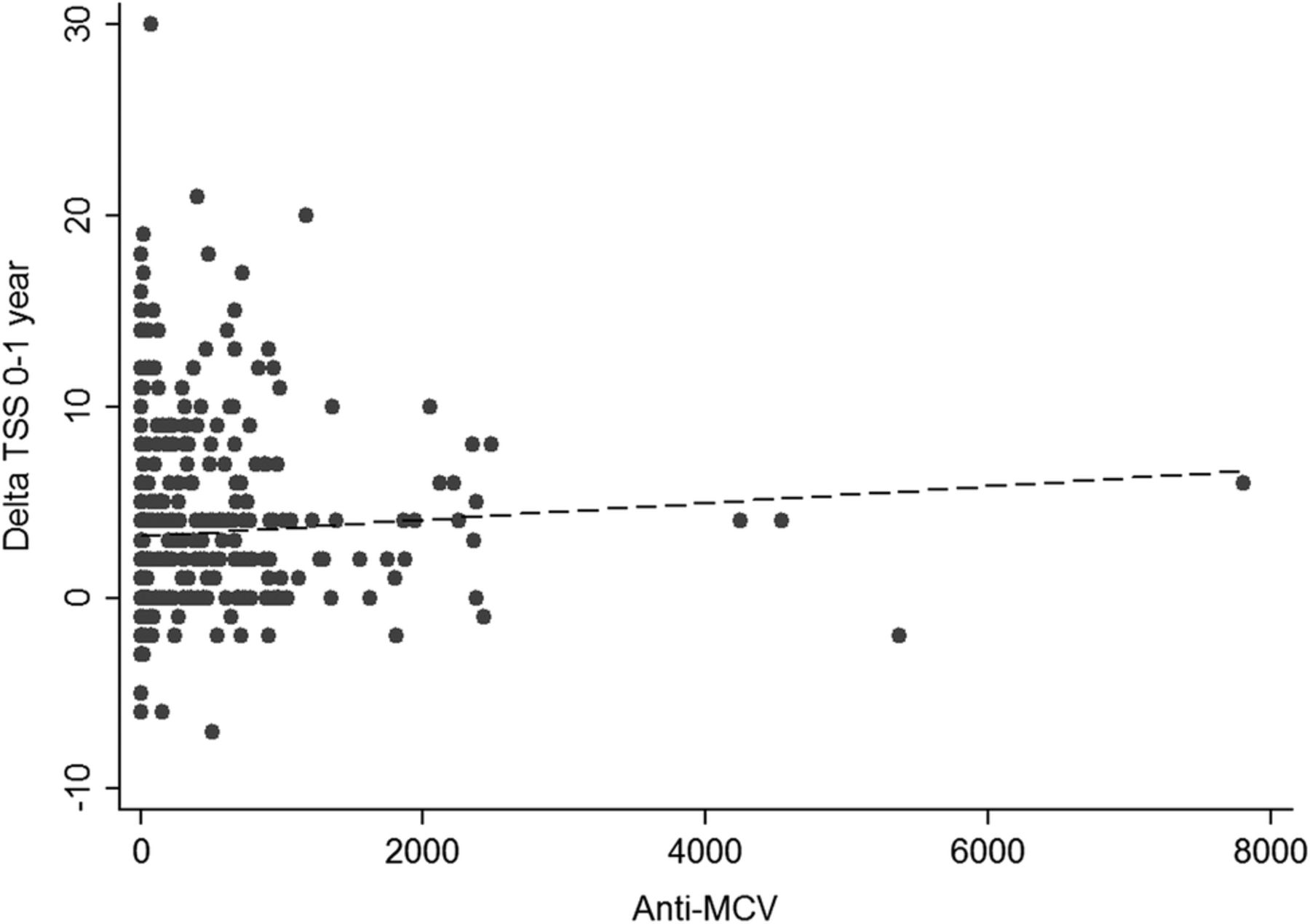
Correlation between anti-MCV titres and mTSS evaluated by the Spearman correlation test was: 0.214; p<10−6 (see figure 2).
{kind=link}
{kind=link}
Spearman correlation between anticitrullinated peptide antibodies (ACPA) titres and total modified sharp score (mTSS): antimutated citrullinated vimentine antibodies (anti-MCV) test.
RRP risk by shared epitope carriage and ACPA status
We analysed the RRP outcome in regard to the SE status and ACPA positivity (table 3). In the SE negative subgroup (249 patients), ACPA-positive patients displayed a significant higher RRP risk when compared to ACPA-negative patients. However, this increased RRP risk was observed with anti-CCP2 and AhFibA tests but not with the anti-MCV test (OR=1.86; 95% CI 0.94 to 3.64). In the SE-positive subgroup (292 patients), ORs were not different from 1, whichever the ACPA test was.
One-year RRP in regard to the shared epitope and ACPA status
Multivariate analysis of 1 year RRP risk
To test the independence of the association of ACPA with 1 year RRP, we evaluated four multivariate models by backward logistic regression. Results are shown in table 4.
Multivariate analysis of variables associated with 1 year RRP
With assessment of ACPA positivity as a binary variable (presence/absence; models 1, 2 and 3), both anti-CCP2 and AhFibA tests were significantly associated with 1-year RRP (anti-CCP2: OR 2.15, 95% CI 1.43 to 3.21; AhFibA: OR 2.39, 95% CI 1.57 to 3.63). In model 2, anti-MCV positivity was not significantly associated with 1 year RRP.
In model 4, only high anti-MCV positivity was conserved among the three ACPA.
For the four models, a positive CRP level was associated with 1 year RRP, as were presence of erosions or RF positivity.
Results concerning anti-CCP2 and anti-MCV at other positivity thresholds were similar (see online supplementary table S5).
Discussion
ACPA are among the best predictors of erosive RA. A direct role of the RA-specific autoantibodies in production of structural damage is highly suspected.7 ,20 In modelling the RRP risk at 1 year after inclusion in the ESPOIR cohort, we identified initial erosions, CRP positivity, RF positivity and ACPA positivity as the best prognostic markers. Even if it was expected, since AhFibA constitute a subfamily of ACPA, this work is the first to demonstrate that AhFibA positivity is comparable to anti-CCP2 positivity regarding association with the risk of 1 year RRP. For AhFibA-positive and anti-CCP2-positive patients, association with the 1 year RRP risk was significant whatever the titre. By contrast, in anti-MCV-positive patients, only those with a high titre showed increased 1 year RRP risk.
The impact of ACPA fine specificities on radiographic outcome remains difficult to specify. The discrepancies between studies may be explained by differences in inclusion criteria and treatment regimen across studies. Only few studies compared ACPA specificities in terms of radiographic outcome.
In our cohort, low anti-MCV titres were not associated with 1 year RRP, as compared with high ACPA titres. The threshold of 3N was more discriminating to predict the risk of RRP among patients with a positive anti-MCV test, which was not the case with two other tests. In multivariate analysis, the erosive burden brought by ACPA positivity was associated with high anti-MCV titre but not with the other two tests titres. Thus, the anti-MCV titre was discriminating to predict the evolution towards 1 year RRP unlike the other two tests titres.
Syversen et al21 ,22 were among the first to show that high anti-CCP2 and high anti-MCV (ELISA, Orgentec) titres added information to the radiographic outcome when compared to ACPA positivity. The observation concerning anti-MCV test supports our results. In these studies, high ACPA corresponded to the third tertile (>253 U/mL) for anti-MCV test and >200 U/mL for anti-CCP2 test. It seems important to consider that: high ACPA titres in these papers are higher than our cut-off (3 times the positivity threshold ie, 75 U/mL for anti-CCP2 and >60 U/mL for anti-MCV) and populations studied were not comparable.
In the current work, one weakness is the small sample size for patients with low anti-MCV positivity (51 patients). Most of the patients with rapid RRP had high ACPA titres (approximately 60%) and only a few (<10%) had low+ ACPA. We cannot exclude the fact that a lack of power could explain the absence of observed 1 year RRP risk in the low+ anti-MCV group. However, even with small sample size for patients with low anti-CCP2 positivity and low AhFibA positivity, we observed an over-risk of 1 year RRP. These results need to be confirmed on other cohorts of early RA.
Studies assessing prognostic relevance of anti-CCP levels often evaluated ‘radiographic progression’. We assessed the correlation with the ‘rapid radiographic progression’ (RRP), with a different definition from ‘radiographic progression’. The change in the radiographic outcome may influence the results.
Considering the anti-CCP2 test, we did not make the same observation as with the anti-MCV test, and the 3N threshold did not seem discriminating for identifying RRP RA. The wide antigen specificity of the anti-CCP2 test could also ‘attenuate’ the radiographic discriminating properties of some ACPA specificity titres.
We analysed patients with serodiscordance between the three ACPA tests. There were only a few patients displaying serodiscordance and subgroup size was too small to draw any firm conclusion. This concordance between the three ACPA tests suggests that they detected ‘similar’ autoantibodies. This concordance also suggests that, to improve our knowledge of the link between autoantibodies fine specificities and radiographic outcome in RA, assessment of tests with lower concordance is needed.
Our results should be interpreted with regard to the qualitative aspect of the ACPA test used. The commercial anti-CCP2 kit uses a mix of synthetic citrullinated peptides. Thus discussion about the fine specificities of ACPA and radiographic outcome is inappropriate with this test owing to its wide specificities. This kind of report cannot be made with home-made tests such as AhFibA. Although it is justifiable to wonder about the performances of home-made tests, the AhFibA test proved it was a reliable test for RA diagnosis with similar performances to those of anti-CCP2 and anti-MCV tests when used on a large scale on the ESPOIR cohort.11
We assessed the relationship between SE carriage, ACPA positivity and radiographic outcome. ACPA positivity was associated with an increased RRP risk, but only in the SE negative subgroup. This result suggests an interaction between the SE and the ACPA status with a redundancy. This interaction could explain why we did not find an association between SE carriage and RRP in our multivariate analysis models including ACPA status. Similar results were reported in a paper by Scherer et al.5 In their study, concerning patients with RA from the Leiden Early Arthritis Clinic and EURIDISS cohorts, SE alleles were associated with RRP. This association was not observed in the ACPA-positive subgroup.
Concerning comparability on therapy, we assessed the rapid RRP in different groups of patients depending on their treatment (data not shown). Baseline steroids and 1 year steroids use did not influence the 1 year RRP status. DMARDs use at year 1 influenced the radiographic course. Biologics use during the first year did not seem to influence the rapid RRP. But it is important to take into account that the inclusions were incorporated between 2002 and 2005 and that only 40 patients used biologics during the first year. Thus we cannot draw any conclusion concerning biologics. We cannot exclude the fact that some of our results could be explained, at least in part, by the treatment or the population size. We analysed the ‘treatment with DMARD at year 1’ as a variable (data not shown). About 83% of the patients were treated with any DMARD at year 1. Although associated with protection against rapid RRP in univariate analysis, this variable was not associated in our multivariate analysis, and keeping this variable in the three ACPA tests multivariate models did not change the results observed.
Our data concerning the anti-MCV test and the recent report of better radiographic outcome for patients with anti-MCV seronegativation20 support the point that, among ACPA tests, the anti-MCV test may predict RRP. The anti-MCV test is specific for the diagnosis of RA; we showed that anti-MCV titres may also be informative to predict 1 year RRP.
Acknowledgments
The authors thank Nathalie Rincheval for expert monitoring and data management; S Martin for measuring the central doses of CRP level, IgA and IgM RF, and anti-CCP antibodies; the Biological Resources Centre (Paris-Bichat, J Benessiano), which was in charge of centralising and managing biological data collection; and all the investigators who recruited and followed patients (F Berenbaum, Paris-Saint Antoine; M C Boissier, Paris-Bobigny; B Combe, Montpellier; M Dougados, Paris-Cochin; P Fardelonne and P Boumier, Amiens; B Fautrel and P Bourgeois, Paris-La Pitié; R M Flipo, Lille; Ph Goupille, Tours; F Liote, Paris-Lariboisière; X Le Loet and O Vittecoq, Rouen; X Mariette, Paris-Bicêtre; O Meyer +, Paris Bichat; A Saraux, Brest; Th Schaeverbeke, Bordeaux; J Sibilia, Strasbourg).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
- Data supplement 3 - Online table 3
- Data supplement 4 - Online table 4
- Data supplement 5 - Online table 5
Abstract in French
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Abstract in French - Online abstract
Footnotes
Funding An unrestricted grant from Merck, Sharp and Dohme (MSD) was allocated for the first 5 years of the ESPOIR cohort. Two additional grants from INSERM were obtained to support establishing part of the biological database. The French Society of Rheumatology, Abbvie and Wyeth also supported the ESPOIR cohort study, but the industrial firms were not involved in the study design, data collection, data analysis, manuscript preparation or decision to publish.
Competing interests None declared.
Ethics approval Ethics approval was provided by Montpellier Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.