Article Text

Abstract
Background Systemic sclerosis (SSc) is a severe, progressive multiorgan disease but to date, there are no established standardised international guidelines for follow-up of patients with SSc. The goal of this project was to develop an expert consensus for annual systematic investigations in patients with SSc to enhance their standard-of-care.
Material and methods The Delphi method was applied. All SSc experts from the European Scleroderma Trials and Research group network and the Scleroderma Clinical Trial Consortium were invited to participate. All experts were asked to answer questionnaires in five Delphi steps to determine the domains of interest and tools for each domain for an annual systematic assessment of patients with SSc. Each item was rated on a scale between 0% and 100% (not and very important), and parameters rated >80% by more than 75% of the experts were regarded as acceptable.
Results In total, 157 experts worldwide participated with 71.3% experts seeing >50 patients with SSc annually. In the first round, 23 domains and 204 tools were suggested. After five Delphi steps, experts agreed on 10 domains including (1) Raynaud’s phenomenon; (2) Digital ulcers; (3) Skin and mucosa; (4) Lung; (5); Heart; (6) GI domain, (7) Renal; (8) Musculoskeletal; (9) Laboratory and (10) Treatment. Overall, 55 tools were identified including clinical assessments, laboratory measurements and imaging or functional investigations.
Conclusion Through five Delphi steps with world leading experts, a consensus was established on strongly suggested tools for a minimum annual systemic assessment of organ involvement in SSc. This work should enhance the standardisation and homogenisation of the practices.
- systemic sclerosis
- autoimmune diseases
- multidisciplinary team-care
- qualitative research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Systemic sclerosis (SSc) is a severe, progressive multiorgan disease but to date, there are no established standardised international guidelines for follow-up of patients with SSc.
What does this study add?
Through this study, a consensus on strongly suggested and easily applicable tools for a minimum annual systemic assessment of organ involvement in SSc was established with world leading experts.
How might this impact on clinical practice?
The development of these easily applicable tools may ensure an adequate standard of care for all patients with SSc and enhance the standardisation and homogenisation of the practices worldwide.
Introduction
Systemic sclerosis (SSc) is a severe multiorgan disease that is associated with substantial morbidity and mortality and impaired quality of life.1–5 Lung and heart involvement are currently the major causes of disease-related deaths in SSc, while scleroderma renal crisis was the predominant cause of death in previous decades.1 6 7 Skin, gastrointestinal (GI) and musculoskeletal involvement, digital ulcers (DU) and Raynaud’s phenomenon (RP) have shown to be associated with high morbidity, reduced quality of life and lower social functioning.2 3 8 9 SSc can be progressive and many of the disease features including ILD and GI dysfunction can aggravate over time.3 5 In 2013, new classification criteria for SSc were launched and they have been shown to be a major step forward in identifying patients with SSc particularly at early stages compared with previous criteria.10 11 Although early classification has been improved, there are no standardised international guidelines for the follow-up of patients with SSc. One exception is the 2015 European Society of Cardiology and the European Respiratory Society (ESC/ERS) guideline recommending annual echocardiography (echo) in all patients with SSc to determine the risk of pulmonary hypertension (PH).12 13 Recent studies indicate that echo screening has resulted in earlier PH diagnosis, with earlier onset of specific therapies and increased survival.14 It is therefore conceivable that a standardised follow-up of other disease features than PAH could have beneficial effects on morbidity and mortality in patients with SSc, improve quality of care and impact quality of life. The follow-up of patients with SSc may also vary between academic centres and non-academic centres; therefore, a unified, standardised annual systemic assessment of organ involvement in SSc should exist to guarantee all patients with SSc an adequate standard of care regardless of location and centre.13 15
The European Scleroderma Trials and Research group (EUSTAR) has been founded in Europe to foster the study of SSc with the aim of achieving equality of assessment and care of patients with SSc according to evidence-based principles throughout the world.16–18 Their work has enhanced the awareness of SSc worldwide substantially leading, among other things, to an increased number of clinical trials.19 20 With new treatment options for SSc in pipeline, the interest in developing valid methods for a standardised follow-up of patients has increased to diagnose disease progression at an early stage and to be able to start treatment in a timely matter.19
The aim of the present study was to establish an expert consensus regarding the annual systemic assessment of organ involvement in SSc and to develop easily applicable tools that may ensure an adequate standard of care for all patients with SSc and enhance the standardisation and homogenisation of the practices worldwide.
Material and methods
Initiation, steering board and participating centres
This study was initiated by the EUSTAR board and led by the first and last author (AMHV and YA). The steering board of the study included the EUSTAR board (YA, OD, OK), the first author (AMHV), the president of the Scleroderma Clinical Trial Consortium (SCTC) (MB) and an invited international SSc expert from Northern America (DK). All experts in SSc registered in the EUSTAR network and the SCTC were invited to participate in the study to cover a broad spectre of physicians following patients with SSc. All participants were individually informed and invited multiple times by email in December 2016. The final independent expert panel included a multidisciplinary team including rheumatologists, dermatologists, pulmonologists, cardiologists and nephrologists. No patients were represented in the process.
Delphi method
The Delphi method is a systematic interactive way of gaining opinions from a panel of independent experts over two or more steps frequently applied in medical and health service research. It is a type of consensus method which does not require face to face meetings and thereby enables participation of experts without geographic limitations; and the internet-based method allows a large number of experts to participate worldwide. Through the stepwise procedure, participants can change their opinion after statistical feedback of the group response in consecutive stages of the process. The Delphi method was internet-based and completed from December 2016 until October 2017. To ensure security and confidentiality, each participant received a web link attached to the email invitation, allowing individual access to the questionnaire. All participants received three email reminders per step. It was possible to interrupt the survey at any time and complete it later. The survey was pilot tested by the initiators.
Delphi rating
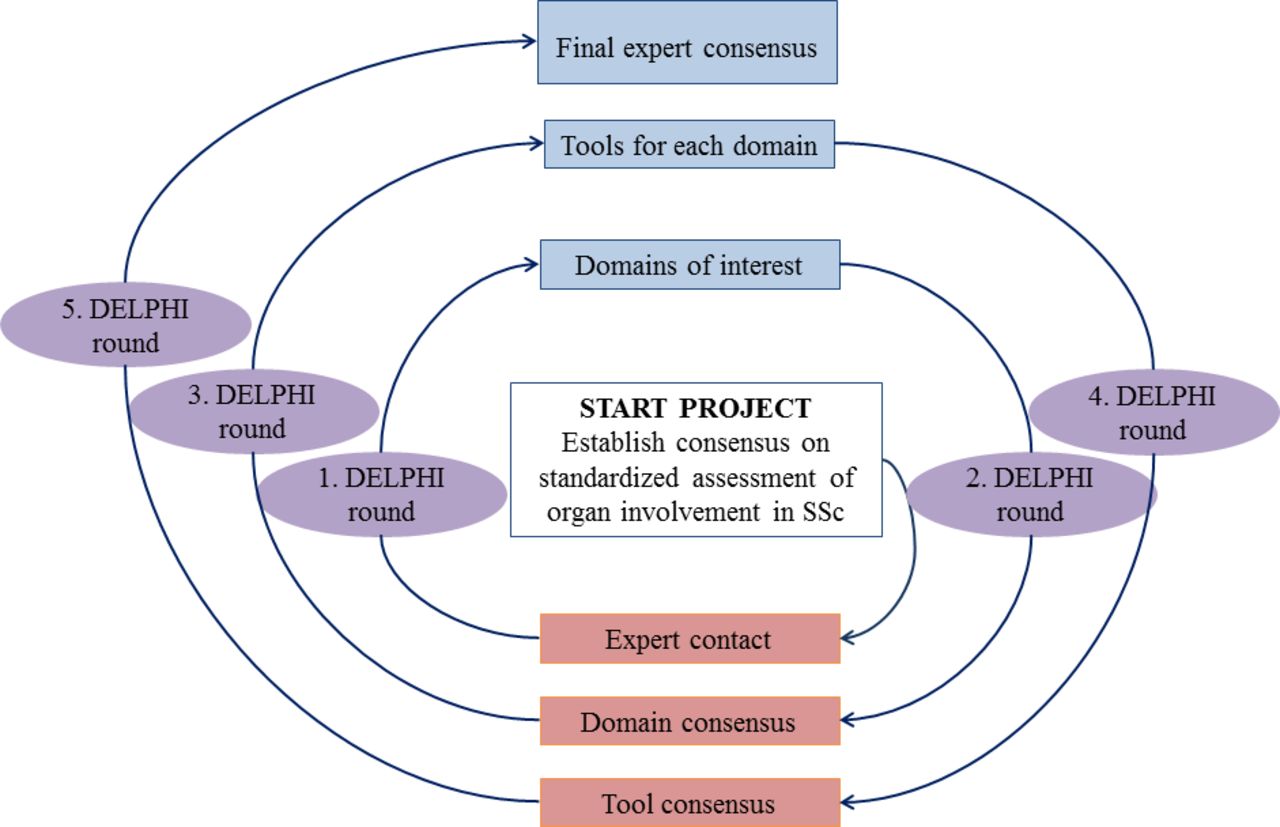
The goal of the different steps was to reduce the range of responses and arrive ultimately at an expert consensus. The method included five Delphi steps and entailed the entire group of experts who anonymously replied to in total five online questionnaires (figure 1) and a last step including solely the steering committee. The participants did not have the ability to see comments or answers from other participants. Every item in every questionnaire and step was asked to be rated between 0% and 100%, with 100% as ‘very important/appropriate’ and 0% as ‘not important/appropriate at all’. Participants did not have to provide a ranking of each individual domain and/or tool to be able to finish the survey in any step. Consensus was defined based on ratings of the experts. In all steps, parameters rated >80% by more than 75% of the experts were regarded as consented.21 Parameters regarded as consented were reconciled by the study initiators before proceeding to the next step. All experts subsequently received feedback in the form of a statistical representation of the ‘group response’ per email after each step before the process repeated itself.

Delphi method applied to achieve expert consensus on standardised assessment of organ involvement in SSc. SSc, systemic sclerosis.
First step
In the first step, domains of interest for an annual systematic investigation were determined. All experts were contacted by email and asked to provide an overview over their proposed domains to establish a consensus agreement for annual systemic assessment of patients with SSc (figure 1).
Second step
In the second step of the Delphi survey, participants were asked to rate every single domain included based on the information received by the experts in the first step (figure 1). All experts received a web link sent by email and were asked to answer the question: ‘Which domains do you strongly suggest for the minimum annual systemic investigation of SSc patients’; and to score each individual item included in the survey as mentioned above. This step in the Delphi survey was performed to give responders the chance to reflect their opinion on specific items of the previous step.
Third step
In the third step, proposed tools for each domains of interest for an annual systematic investigation were determined. All experts were contacted again by email and asked to provide an overview over their proposed tools for each domain to establish a consensus agreement for annual systemic assessment of patients with SSc similar to step 1 (figure 1). All participants were at the same time informed about the results from the second Delphi step.
Fourth step
In the fourth step of the Delphi survey, participants were asked to rate the tools for each domain based on the received information from the experts of step 3 (figure 1). In this step, all experts received web links sent by email and were asked to answer the question for each tool: ‘Which tools for each domain do you strongly suggest for the minimum annual systemic investigation of SSc patients’; and to score each individual item included in the survey as mentioned above. To reduce the lengths of the questionnaires, the 10 domains were separated into five links, sending out with a web link once a week.
Fifth step
The preliminary results from the fourth step were shown and discussed with the experts at the EUSTAR reloaded meeting in Florence in August 2017 where all EUSTAR centres were invited to participate. This was followed by the fifth step in the Delphi survey, where all participants received a web link sent by email to answer the question for each domain: ‘Which final tools for each domain do you strongly suggest for the minimum annual systemic investigation of SSc patients’ and to score each individual item included in the survey. This step was performed to repeat the rating of all included domains and tools from the previous steps to reflect their opinion for a last time on specific tools for each domain.
Last step
In a last step, the steering board perused all final tools (box 1) for feasibility reasons, faces validity and phrasing and discussed every single variable in multiple rounds.
Overview of the tools for each domain that the SSc expert panel agreed on for the longitudinal annual assessment of organ involvement in systemic sclerosis
1. Domain: Raynaud’s phenomenon
Symptoms: Frequency and severity of attacks
2. Domain: Skin and mucosa
Symptoms: Skin changes (worsening or improvement; patient reported)
Clinical assessment: Puffy fingers, modified Rodnan Skin Score (mRSS), telangiectasias, calcinosis
3. Domain: Musculoskeletal
Symptoms: Muscle weakness and stiffness
Clinical assessment: Puffy fingers, joint contractures, arthritis, calcinosis, tendon friction rub count
4. Domain: Digital ulcers
Symptoms: Fingertip ulcers, finger ulcers proximal of DIP joints, development of new ulcers during the last year, coexisting conditions relevant for perfusion (ie, diabetes), smoking status
5. Domain: Lung
Symptoms: Dyspnoea
Functional assessment: Functional class (NYHA 1–4)
Clinical assessment: Basal lung crackles on auscultation
Investigation: Lung function test and DLCO
6. Domain: Heart
Symptoms: Dyspnoea
Functional assessment: Functional class (NYHA 1–4),
Clinical assessment: Leg oedema
Investigation: ECG, Doppler-echocardiography, heart rate, blood pressure
Others: Concurrent heart disease
7. Domain: Gastrointestinal
Symptoms: Night and day time heart burn/reflux, dysphagia, diarrhoea, weight loss
Clinical assessment: Weight
8. Domain: Renal
Investigation: Serum creatinine, eGFR, urine analysis, blood pressure
9. Domain: Laboratory
Investigation: Acute phase reactants, creatine kinases, haematology, renal function test, liver function test
10. Domain: Treatment
Type of treatment (generic and name of drug), date of initiation, date of finalisation of every medication
Statistics
Analyses were performed with IBM SPSS software, V.22, and STATA software, V.14. Descriptive statistics were applied.
Results
Response rate and characterisation of the participating centres
Of the 269 invited registered experts from EUSTAR and/or SCTC, 157 (58.4%) participated in at least one of the steps in the Delphi survey. In 46 cases (17.1%), the emails were not able to deliver due to unknown recipients. In step 1, 132 (84.1%) participants responded. Step 2 was answered by 118 participants (75.2%), step 3 by 125 (79.6%), step 4 by 108–115 (68.8%–84.1%) and step 5 by 126 (80.3%), respectively. Of the participants, 71.3% were seeing >50 patients with SSc annually and 48.3% seeing >100 patients on an annual basis. Of all, 115 of the centres of the participating experts were located in Europe (73.2%), 23 in North America (14.6%), 9 in Asia (5.7%), 6 in South America (3.8%) and 4 in Oceania (2.5%).
Domains and tools determined through five Delphi steps
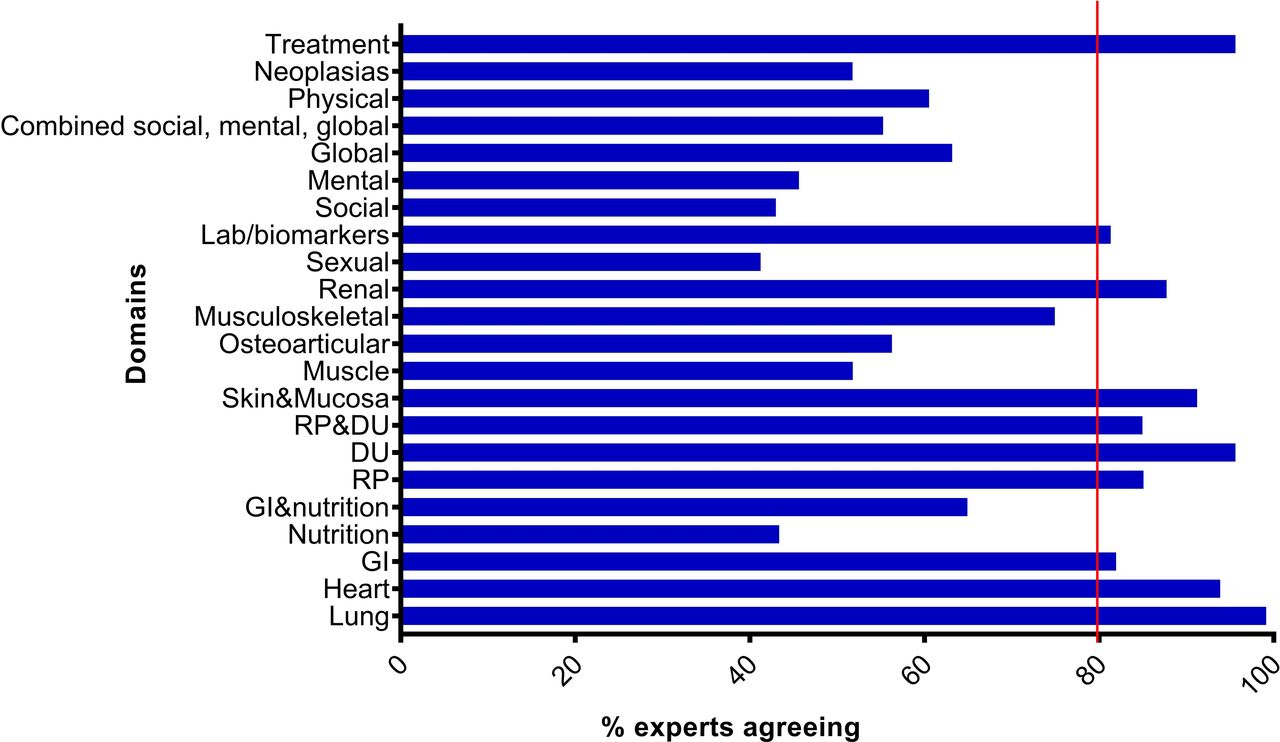
In the first Delphi step, 23 domains were suggested by the expert participants and sent individually to the study lead. In the second step, these domains were rated by the experts as shown in figure 2. Out of the 23 domains, 10 domains were rated as >80% by>75% of all participating experts. Nine were included in the fourth step by the definition of reached consensus. The ‘Raynaud’s phenomenon and digital ulcer’ domain was excluded by the study lead since it fully equalled to the single domains for ‘Raynaud’s phenomenon’ and ‘digital ulcer’. The musculoskeletal domain was rated as 74.2% by >80% of the experts and did not meet the a priori definition for consensus. It was nevertheless included as a domain after discussion of the study lead due to the borderline rating and the importance of this domain for measuring disease activity in SSc. All participants were informed about the decision and the rationales before starting in step 3. No complaints from the participants were received.

{kind=link}
{kind=link}
Results from the second Delphi step showing the percentage of rated domains that the experts agreed on as domains for the annual systemic assessment of organ involvement in systemic sclerosis. DU, digital ulcers; GI, gastrointestinal; RP, Raynaud’s phenomenon.
In the third round, a large number of tools for each domain were sent from each individual participant to the study lead (online supplementary table 1). All the received tools were included in the online survey of the fourth step and rated by all participating experts. The tools for each of the 10 domains that were rated as >80% by >75% by all experts were included in the last step of the Delphi survey (online supplementary table 1). These results were presented and discussed at the EUSTAR meeting with 70 participating experts. Rationales for including the musculoskeletal domain were once more presented and broad approval achieved by the participating experts.
Supplemental material
In the last Delphi round, all tools for each domain from the fourth round were re-rated. Another 11 tools from step 4 were excluded and the final tools for each domain are shown in box 1.
Last step
In a last step, the steering board perused and discussed all final tools for clarification of the terminology, but did not remove any items. The final consensus was considered as having high face validity with regard of the transparency and relevance of included items.
A case report form was developed by the steering board (online supplementary table 2) for practical implications that can easily be applied if preferred by the physicians following patients with SSc longitudinally. Since the consensus does not contain specified measures for the included items, for all tools overlapping with items from the existing EUSTAR registration, their measures and definitions were chosen due to long experience and use of the majority of participating experts. As this step was no longer part of the consensus, this is the sole opinion of the steering board rather than a consensus of the whole group.
Supplemental material
Discussion
Achieving equality of assessment worldwide will most likely increase the standard of care for SSc. However, to date there are no existing guidelines for standardised follow-up of patients with SSc. In this study, we developed an expert consensus on the requirements for annual assessment of organ involvement in SSc by applying the Delphi method. We propose a minimum set of 10 key domains in SSc with related sign/symptoms and tools for assessment. All the items are easily applicable, even in non-academic centres, and we believe that they ensure an adequate standard of care for patients with SSc worldwide.
There are few existing expert consensus and suggestions from single centres or national networks on SSc follow-up, mainly focusing on one single organ, but to the best of our knowledge, this is the first study where an international multidisciplinary panel reached consensus on the longitudinal follow-up scheme covering all core clinical domains in SSc.13 22
To reach consensus, we applied the Delphi method including a structured flow of information, with repetition and feedback and anonymity for the participants during the exercise. Aiming to develop tools that should be applicable in most clinical practices and easy to implement across health systems and national regulations, we considered it as important to design a broad, multidisciplinary panel including five different disciplines that would cover a wide range of experience with patients with SSc (from academic centre experts, clinicians from non-expert centres to researchers with little clinical experience) and the most important specialities involved in the care of patients with SSc (rheumatology, dermatology, cardiology, pulmonology and nephrology). We chose an ambitious inclusion of participants and invited all members of EUSTAR and SCTC to cover afore-mentioned demands and achieved to include a large amount of experts. The response rate was comparable to previously published Delphi exercises, but somewhat lower than anticipated, probably due to the fact that not all participants could be addressed personally due to limitations of updating email addresses of international experts registered in EUSTAR and SCTC.13 However, the total number of participating experts in this Delphi and the response rate to the different steps throughout the process was constant and high.
In 2011, Khanna et al performed a comprehensive literature review and the RAND/UCLA appropriateness method and proposed a set of quality indicators (QIs).23 In total, six domains were included in the follow-up section. Interestingly, by comparing the 10 items included in the tools in the present study, we found partly overlapping results except for the musculoskeletal domain where the QI included more comprehensive assessments taking into account MRI and EMG.23 Conversely, in the present study, the domains ‘DU’, ‘RP’ and ‘skin and mucosa’ were included as well as more tools in the laboratory domain. The domains of this study additionally overlap to a large degree with the domains in the treatment guidelines for SSc strengthening the importance of the core clinical domains in the final consensus.24 For the musculoskeletal domain, we made an exception of the entry criteria due to the importance of this domain for measuring disease activity in SSc. This might be a point of discussion; however, the participants were informed and in the next step and at the EUSTAR meeting, and there was no disagreement.
The information collected should have ideally reflected disease activity, disease status (remission) and organ damage, to predict outcomes and modulate treatment regimen. Unfortunately, in patients with SSc, concept of remission/low disease activity has never been validated and was therefore not considered in this consensus.
It must be emphasised that the final domains and assessment tools of this Delphi survey are the subjective opinion of experts in the field. This should not be confused with validation of particular domains and measurement tools, which was not the aim of the present study. Also, local feasibility, the applicability and usefulness of the present consensus data need to be evaluated in the respective countries due to varying possibilities in the different health systems. Hence, it will be necessary to formally validate the present expert consensus data in future studies and to conduct systematic literature reviews on the single domains and tools. Additionally, these consensus data should be evaluated by representatives of patients with SSc with distinct pathologies to add their opinions on priorities, effectiveness and meaningfulness of the consensus data, for weighing risks and benefits and assessing acceptability and feasibility.25
There are a number of other limitations to this study. Consensus statements are, in general, graded as the weakest form of evidence. However, they are still considered as the optimal method for identifying areas of interest for further research and future practice. The selection of experts is another critical issue with consensus statements. The group of experts involved in this study were all members of EUSTAR or SCTC with varying expertise and some experts might have been missed. Since SSc is a clinically heterogeneous disease, items required for assessment may also be different among patients: that is, dcSSc vs lcSSc, and early dcSSc and late dcSSc. This may influence items required for assessment and an interval of assessment but has not been considered in this consensus.
In conclusion, through five Delphi rounds with world leading experts in SSc, an expert consensus was established on strongly suggested tools for a minimum annual systemic assessment of organ involvement in SSc.
Acknowledgments
The authors are grateful to the experts who contributed to this project.
References
Footnotes
Collaborators EUSTAR and SCTC collaborators.
Contributors Substantial contributions to the conception or design of the work; or the acquisition, analysis or interpretation of data for the work: All authors. Drafting the work or revising it critically for important intellectual content: All authors. Final approval of the version to be published: All authors. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: All authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests A-MH-V has obtained research support from Boehringer Ingelheim. She is a scientific consultant for Actelion and Boehringer Ingelheim in the field of systemic sclerosis and related diseases. She has received travel expenses from GSK, Actelion and Boehringer Ingelheim. OD has obtained research support from Bayer, Sanofi, Ergonex, Boehringer Ingelheim, Actelion and Pfizer. He is a scientific consultant for 4 D Science, Actelion, Active Biotec, Bayer, BiogenIdec, BMS, Boehringer Ingelheim, ChemoAb, EpiPharm, Ergonex, espeRare foundation, Genentech/Roche, GSK, Inventiva, Lilly, medac, MedImmune, Pharmacyclics, Pfizer, Serodapharm and Sinoxa in the field of systemic sclerosis and related diseases and has a patent licensed on mir-29 for the treatment of systemic sclerosis. OK-B received consultancies, honoraria and/or speaker fees from Abbvie, Actelion, Bayer, Roche. DK has received consulting fees from Actelion, Bayer, Bristol-Myers Squibb, Cytori, CSL Behring, Corbus, Genentech/Roche, GlaxoSmithKline, Inventiva, Regeneron, Sanofi-Aventis and UCB and has stock options with Eicos Sciences, Inc. YA has/had consultancy relationship and/or has received research funding in relationship with the treatment of systemic sclerosis from Actelion, Bayer, Biogen Idec, Bristol-Myers Squibb, Genentech/ Roche, Inventiva, Medac, Pfizer, Sanofi/Genzyme, Servier and UCB.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data collected for this manuscript are included and there are no additional data for sharing.