Article Text

Abstract
The therapeutic window of opportunity in rheumatoid arthritis (RA) is often referred to. However, some have questioned whether such a period, in which the disease is more susceptible to disease-modifying treatment, really exists. Observational studies are most frequently referenced as supporting evidence, but results of such studies are subject to confounding. In addition formal consensus on the definition of the term has never been reached. We first reviewed the literature to establish if there is agreement on the concept of the window of opportunity in terms of its time period and the outcomes influenced. Second, a systemic literature search was performed on the evidence of the benefit of early versus delayed treatment as provided by randomised clinical trials. We observed that the concept of the window of opportunity has changed with respect to timing and outcome since its first description 25 years ago. There is an ‘old definition’ pointing to the first 2 years after diagnosis with increased potential for disease-modifying treatment to prevent severe radiographic damage and disability. Strong evidence supports this concept. A ‘new definition’ presumes a therapeutic window in a pre-RA phase in which the biologic processes could be halted and RA development prevented by very early treatment. This definition is not supported by evidence, although is less well studied in trials. Some suggestions for future research in this area are made.
- rheumatoid arthritis
- treatment
- outcomes research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Outcomes for patients with rheumatoid arthritis (RA) have changed dramatically over the last 25 years. These advances have been attributed to the development and use of novel disease-modifying drugs (including biologics), treat-to-target strategies resulting in better control of disease activity, and the earlier initiation of disease-modifying treatments.
The rationale behind earlier treatment initiation is that it allows modulation of biologic processes while they are in a less mature and more reversible stage.1 2 This stage has previously been referred to as a therapeutic window of opportunity.1 2 Nevertheless, varying definitions exist of the window of opportunity. The first mention of a window of opportunity in RA was in 1992 by Dawes and Symmons.3 At that time it was described as ‘a small window of opportunity (2 years) in which to get the disease in remission before irreversible damage is done to joints’. Since then, the term ‘window of opportunity’ has been increasingly used in the rheumatological literature. However some have questioned whether such a period, in which the disease is more susceptible to disease-modifying treatment, really exists, and formal consensus on the definition of the term has never been reached.
In this Viewpoint we set out to propose a definition of the ‘window of opportunity’ based on data obtained from the literature. First we questioned whether or not the term ‘window of opportunity’ has been used in a consistent way since 1992. To address this, we reviewed the literature on articles that used the term ’window of opportunity’ in the context of RA. We explored whether there was consensus in terms of the long-term outcomes that were considered to benefit from early treatment, as well as on the time period, expressed as the symptom or disease duration, that was proposed to cover the window of opportunity. Second, we determined the level of evidence for the association between the timing of intervention and the disease outcomes that were identified in the first part. Although a previous literature review concluded that prolonged symptom duration at treatment initiation in patients with classified RA is associated with more radiographic progression and a lower chance of achieving disease-modifying antirheumatic drug (DMARD)-free sustained remission (findings that may support the presence of a window of opportunity), this conclusion was largely driven by findings from observational cohort studies.4 In such cohort studies, the timing of DMARD start was not determined by randomisation. Therefore, a combination of patient and environmental characteristics, both known and unknown, may have influenced when DMARD therapy was initiated. Because of this, the causality of the associations with symptom duration is susceptible to confounding and reverse causation bias. Randomised controlled trials (RCTs) do not have this drawback. Therefore we systemically searched the literature on RCTs evaluating the effect of early (vs delayed, thus initial treatment with placebo) treatment with DMARDs. We exclusively concentrated the present literature search on findings from RCTs. We studied RCTs performed in patients with classified RA. Moreover, as the field of RA has moved towards identifying patients in earlier disease phases, in the current search we also performed RCTs performed in patients with undifferentiated arthritis (UA) and arthralgia without clinically apparent arthritis.
Is there consensus on how to define the window of opportunity?
A generic search on PubMed on (‘((rheumatoid arthritis) AND window of opportunity)’) resulted in 89 articles; evaluation of full texts revealed 75 relevant articles (both original articles as well as other types of papers) on the window of opportunity.
Timing of the window of opportunity
In 37 of 75 (49%) articles, no exact duration of the window of opportunity was included in the description; these articles often used general terms, like ‘early’. Other articles did not include a chronological period, but a disease phase, such as the phase preceding radiographic damage (two articles)5 6 or preceding RA development (five articles).7–11 With regard to studies that mentioned a specific time duration, some studies described the window to encompass the first 2 years after disease onset (nine articles).3 6 10 12–17 As illustrated in figure 1A, these articles were mainly written in the 1990s and early 2000s. The most frequently used time description period encompassed the first 12 weeks or 3 months after symptom onset (19 articles)1 4 6 10 12 18–31; the majority of these papers were published after 2010 (figure 1A). Hence, as time has passed, the window of opportunity has been assumed to be confined to a shorter period occurring in an earlier phase of the disease.
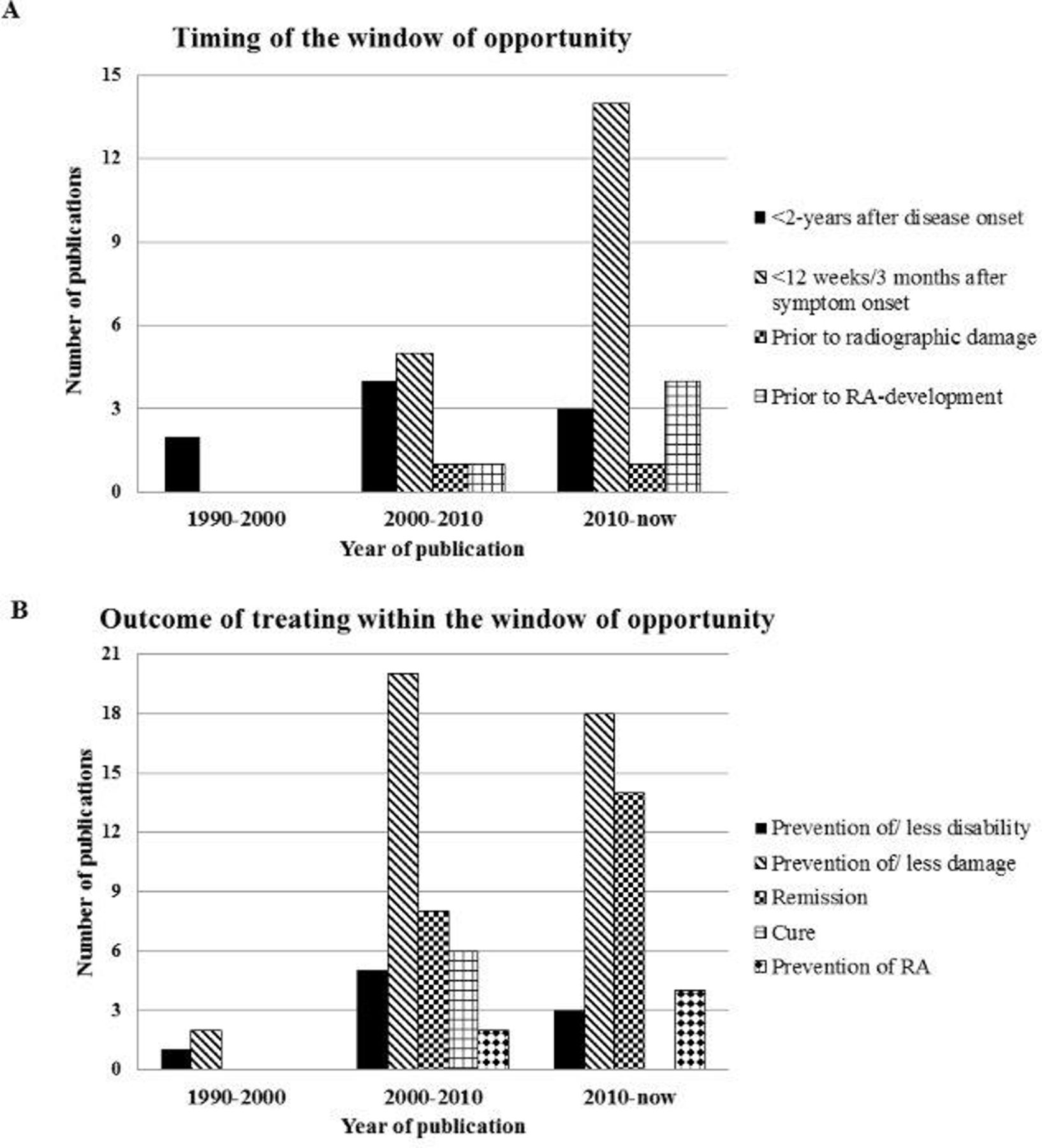
Results from literature search on the concept of the window of opportunity in rheumatoid arthritis (RA) with regard to its time period (A) and long-term outcome that is influenced (B). The bars correspond to the number of times a specific time period or long-term outcome was mentioned in the 75 articles mentioning the window of opportunity in RA. As some articles mentioned more than one time period or outcome, and other papers did not mention a specific time period or outcome at all, the numbers in the bars do not necessarily add up to 75.
Long-term outcomes
Twenty-six out of 75 articles (35%) used general terms with regard to the long-term outcomes that could be achieved when treatment is started within the window of opportunity (eg, ‘sustained clinical benefits’ or ‘better outcomes’). The most frequently mentioned specific outcome was prevention or slowing of radiographic damage (40 articles).3–6 10 12–18 22 24 26 30–54 The second most frequently mentioned outcome was remission, either clinical remission, Disease Activity Score (DAS) remission or drug-free remission (22 articles).1 10 15 16 18 19 22 24–26 31 34 46 48 49 55–61 Furthermore, six articles mentioned that treatment within the window of opportunity could result in cure6 14 29 30 49 62 of RA, and six articles even mentioned prevention of RA as the outcome of treatment within the window of opportunity.7–11 61 As shown in figure 1B, these latter outcomes were present in more recent descriptions of the window of opportunity.
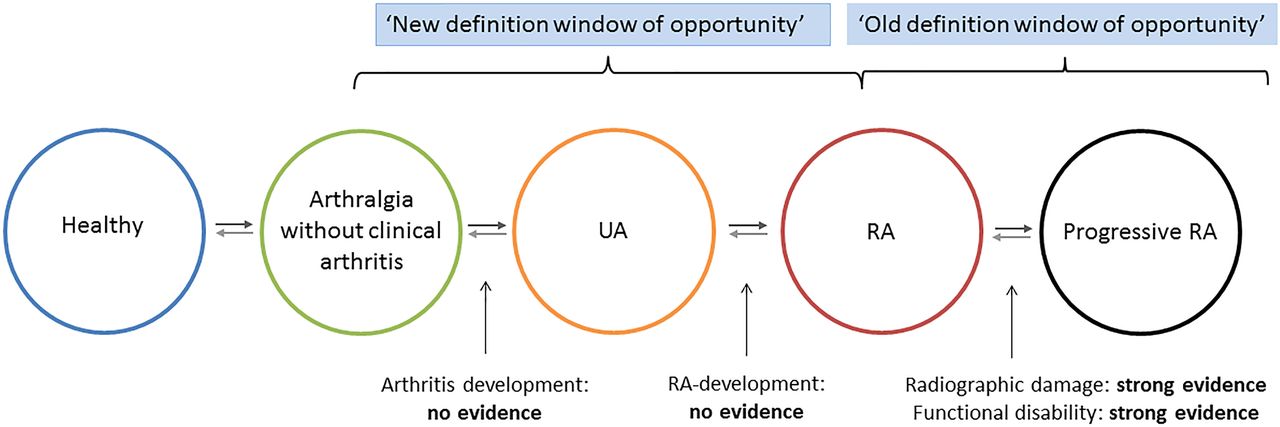
In conclusion, the definition of the window of opportunity as was retrieved from the literature revealed that the concept has changed over time. Whereas it was previously defined as a treatment period in the first 2 years after disease onset in which joint damage could be halted (‘old definition’), it is increasingly considered to represent a period before the diagnosis is established in which treatment could potentially prevent RA development (‘new definition’).
Evidence obtained from randomised clinical trials in favour of early treatment
Next, in order to determine the level of evidence of the associations that are the basis of these definitions, we systematically assessed databases (PubMed, Medline, Embase) for RCTs that compared early versus delayed treatment with DMARDs in different disease phases (RA, UA and arthralgia preceding clinical arthritis) (see online supplementary methods for used terms). Patients in all these phases required to be DMARD-naïve at trial entry. Delayed treatment was defined as absence of DMARD use for a certain period. Hence an early treatment group was compared with a group that only used placebo (please see online supplementary methods for the inclusion and exclusion criteria that were used). The quality of all included studies was determined using a 15-point quality list that was adapted from lists previously used in systematic reviews4 63 (online supplementary tables 1 and 2). As previously,4 studies with a quality score ≥75% were considered high-quality studies. Due to heterogeneity in study designs, pooled effect estimates were not calculated, but a best-evidence synthesis was performed, based on the method described by the Cochrane Collaboration Back Review Group (online supplementary table 3).64
Supplemental material
Supplemental material
RCTs in early RA
First we searched the literature for RCTs in early RA (disease duration <2 years) comparing early DMARD initiation with non-DMARD therapy or delayed DMARD therapy. A total of 11 trials were identified, all published between 1988 and 2003 (table 1); 9 trials assessed the outcome radiographic damage17 65–72 and 8 functional disability.17 65 69–74
Overview of placebo-controlled trials comparing early versus delayed DMARD initiation in early RA looking at radiographic joint damage and disability
Radiographic damage in RA
All nine RCTs included DMARD-naïve patients with a disease duration of <2 years who fulfilled the classification criteria for RA (either the 1958 or the 1987 criteria) (table 1). Follow-up ranged between 6 months and 5 years. Different DMARDs (gold, sulfasalazine, hydroxychloroquine, methotrexate [MTX] and prednisone) and different measures for radiographic damage (Larsen score, [modified] Sharp score, presence of erosions and erosion area) were used. A significant benefit for the early DMARD arm with regard to radiographic damage was shown in five RCTs,17 65 68 70 71 of which three were of high quality17 65 70 (two of these reported on the same trial).17 65 Three RCTs showed a statistically non-significant benefit for the early DMARD arm,66 67 69 and in one trial there was no effect.72 Since there were consistent findings in multiple high-quality RCTs (as well as in low-quality RCTs), there is strong evidence to conclude that early DMARD initiation results in better radiographic outcomes (figure 2). Importantly, earlier treatment resulted in lower absolute levels of joint damage and in lower progression rates (ie, less steep progression curves over time).17 65 70 Especially the latter finding of less rapid rise over time is suggestive of true disease modification. With respect to timelines, the early treatment group in these trials started DMARDs ~6–12 months earlier than the delayed group (table 1).
{kind=link}
{kind=link}
Summary of evidence for randomised controlled trials on the effect of early versus delayed treatment with disease-modifying antirheumatic drugs per disease phase. RA, rheumatoid arthritis; UA, undifferentiated arthritis.
Functional disability
All eight RCTs that measured functional disability as outcome (table 1) included DMARD-naïve patients fulfilling the classification criteria for RA (1958 or 1987) with a disease duration <2 years. Follow-up ranged between 36 weeks and 5 years. Different measures of functional disability were used (Health Assessment Questionnaire, Keitel Functional Index, Arthritis Impact Measurement Scales and McMaster-Toronto Arthritis Patient Preference Disability Questionnaire). Seven of the RCTs were of high quality. However, four different study populations were described, as three articles were long-term follow-up papers of previously reported study populations.17 72 74 Four out of seven high-quality studies revealed a significant benefit for the early DMARD arm,17 65 69 73 of which two reported on the same population.17 65 Of the other three high-quality studies, two reported a non-significant benefit for early treatment.72 74 The early group started DMARDs ~6–12 months earlier than the delayed group. Because of consistent findings in multiple high-quality RCTs, there is strong evidence for early DMARD initiation with regard to improved functional outcome (figure 2).
RCTs in UA aiming to prevent RA development
Next the literature was searched for RCTs in patients with UA (online supplementary methods). Six articles, reporting on five RCTs, compared DMARD treatment with placebo treatment in patients with UA (table 2). Different definitions of UA and inclusion criteria were used (table 2). Follow-up durations ranged between 1 and 5 years, and different DMARDs were investigated (MTX, infliximab, methylprednisolone and abatacept). The outcome was RA according to the 1987 criteria for RA75–78 or the clinical diagnosis.79 80 Four RCTs were of high quality.76 77 79 80 None of the trials reached a significant difference in the primary outcome, but all four high-quality studies showed a tendency towards less RA development in the DMARD arm. Interestingly a recent meta-analysis of trials in patients with UA or very early RA by Hilliquin et al81 did show a significant risk reduction on RA development in the case of DMARD initiation in a pre-RA phase when all trials were combined in one analysis.81 Nonetheless there is no conclusive evidence from individual RCTs that early treatment in patients with UA prevents progression to RA as none of the individual trials revealed a significant reduction (figure 2).
Overview of RCTs comparing early versus delayed DMARD initiation in patients with UA in order to prevent RA development
A difficult issue here is that the outcome in the trials was mostly fulfilment of the 1987 criteria, and that the concept of RA, at least with respect to classification, has changed in the last decennium.82 Some of the patients previously considered as UA may currently be diagnosed or classified as RA. On the other hand, patients with UA with a low risk of RA were also included. As demonstrated recently, such non-informative inclusions diminish the power to detect differences83 and may also have contributed to negative results.
Hopefully, a well-powered, placebo-controlled trial will be done in the nearby future to determine conclusively that early DMARD treatment in UA is beneficial in preventing progression to RA.
RCTs in arthralgia without clinical arthritis aiming to prevent RA development
Finally the literature was searched for RCTs (described in full papers) performed in patients considered at risk for RA development but without arthritis (online supplementary methods). One RCT was identified that included seropositive patients with arthralgia who were shared epitope-positive (table 3).84 Patients were randomised to either dexamethasone or placebo and followed for a median of 26 months. After this period, there was no difference in arthritis development between the two arms. Thus, no evidence from RCTs yet exists for prevention of arthritis by initiating DMARD treatment in patients with arthralgia without clinical arthritis with regard to arthritis/RA development (figure 2). However, several randomised clinical trials are currently ongoing and results are awaited in the next 5 years.7
Overview of placebo-controlled trials comparing early versus delayed DMARD initiation in patients with arthralgia considered at risk for progression to RA in order to prevent arthritis development
Discussion and future perspectives
The term ‘window of opportunity’ is commonly used within the field of RA, although its definition has changed over the last 25 years. There is an ‘old definition’ indicating that the therapeutic window lies within the first 2 years after disease onset, and treatment within it results in less radiographic damage and disability. We have here demonstrated that there is convincing evidence for this effect based on data from RCTs, particularly when treatment was delayed for 6–12 months after diagnosis, due to the use of placebo medication during this period. Notably, earlier treatment resulted in absolute lower levels of radiographic joint destruction and in slower progression rates. Lower absolute levels were possibly only the consequence of an earlier start, whereas a less steep rise in joint destruction is suggestive for true disease modification. In addition to an ‘old definition’, a ‘new definition’ is used in the literature as well. This states that the window could even lie in a phase preceding diagnosis or fulfilment of classification criteria for RA and that treatment initiated could possibly result in prevention of RA. However, this definition is not (yet) supported by evidence from RCTs.
Interpreting data from studies addressing the concept of a window of opportunity is challenging. One particular issue relates to understanding its duration. Measuring the duration of the window requires that a starting point is clearly defined. Many studies exploring the concept of a window of opportunity will simply report ‘disease duration’ and will conclude that treating patients with a disease duration of less than x months is associated with improved outcomes compared with treating patients with disease duration of greater than x months. However, when that x months is timed from is often inadequately described. Possibilities include when the patient first developed (1) inflammatory-type joint symptoms, (2) patient-reported joint swelling, (3) physician-observed joint swelling and (4) physician-documented fulfilment of the RA classification criteria.85 Clearly adopting different definitions of a starting point for the disease onset will lead to different durations of the therapeutic window.21 Although some recall bias may be present when collecting information about starting points, especially when this was a long time ago, specifying the different starting points using uniform definitions will promote comparability between studies and the interpretation of findings.
Another issue relates whether the concept of a window of opportunity requires that there must be a time after which it closes, that is, a time after which intervention is not as effective as it was if used during the window. Trials have used placebo regimens for defined periods of time, but the rationale for the duration of placebo treatment is never discussed. Many observational studies dichotomised symptom duration and compared outcomes; here a cut-off was frequently placed at 3 months after symptom onset. However this choice actually refers back to two observational studies revealing that treatment initiation within 3 months after symptom onset was associated with less damage and more remission; evidence for the choice of this time period was not provided and other time periods were not explored.31 86 Thus far only one study evaluated the time course and provided suggestive evidence that a confined period in which treatment is more effective is more likely than a general ‘the earlier the better’ effect.19
In the first part of this Viewpoint, we assessed the most commonly used definitions of the window of opportunity. A limitation is that this was done by a literature search in one database. We presume that a search in more databases and also incorporating different terminology may have yielded some additional papers providing descriptions of the window of opportunity. However, we expect that a more systematic search will not result in different conclusions regarding the long-term disease outcomes and time periods most frequently mentioned in the different time periods (as presented in figure 1). In the second part in contrast, we determined the level of evidence. Here a systematic literature search of results obtained from RCTs was required. Due to heterogeneity in study designs, meta-analyses were not possible, but a best-evidence synthesis, based on the method described by the Cochrane Collaboration Back Review Group, was performed.
The present review of the literature demonstrated that different definitions of the window of opportunity are used, of which two definitions were common. It is clarifying if subsequent studies that use the term the window of opportunity will specify which definition is meant. The current work does neither allow to make a statement about the best definition of the window of opportunity, nor determine the optimal period for starting disease-modifying antirheumatic treatment. This is subject for future studies.
Conclusion
In summary, while the concept of a window of opportunity in RA is widely used, different definitions of this window exist. We propose to differentiate an ‘old’ and a ‘new definition’. The ‘old definition’ points to the first 1–2 years after diagnosis with increased potential for disease-modifying treatment to prevent severe radiographic damage and disability, whereas the ‘new definition’ presumes a therapeutic window in a pre-RA phase in which the biologic processes could be halted and RA development prevented by very early treatment. A review of RCTs revealed a high level of evidence for the ‘old definition’ but no scientific evidence for the ‘new definition’. As there were relatively few trials performed in pre-RA phases, more research is needed to verify the new definition. Furthermore, to arrive at an evidence-based new definition of the window of opportunity, including information on its duration and possible closing, future trials should use adequately described definitions of the starting point.
Acknowledgments
The authors thank JW Schoones of the Walaeus Library for his help with the literature search.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
Footnotes
Contributors LEB did the literature search. All authors have written the manuscript and consented to the final version.
Funding This work has received funding from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme (starting grant, agreement no 714312). KR is supported by the NIHR Birmingham Biomedical Research Centre.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement No primary data were collected in this manuscript, therefore the authors have no data to share.