Article Text

Abstract
Treatment of rheumatoid arthritis (RA) has improved substantially during the last decades, mainly due to the development and introduction in everyday practice of new, highly efficacious, disease-modifying antirheumatic drugs (DMARDs), more optimal usage of them, earlier diagnosis and tighter control of disease activity targeting at remission. Methotrexate is still today the anchor drug and the first-line treatment after diagnosis. However, numerous studies comparing methotrexate and biologic DMARDs, as well as new targeted synthetic DMARDs, both in early as in more established disease, have shown consistently better efficacy of the latter compared with methotrexate, with methotrexate yielding remission to maximum half of patients. This could suggest a new paradigm shift with earlier start of a biologic or a targeted synthetic DMARD, with the possibility of subsequent discontinuation in case of achievement of stable remission. Several strategy trials, however, have shown that there might be a clinical and structural benefit of initial, aggressive therapy, possibly even associated with higher chance of remaining in remission, after cessation of the biologic DMARD and continuing with methotrexate alone, but they have failed to show a clear advantage of such an aggressive treatment strategy. This might become a valuable option for the future treatment algorithm of RA, especially for a subgroup of patients with RA, but further confirmation from future research is needed. The crucial role of glucocorticoid use as part of the combination strategy should be acknowledged, and strategy trials should include this combination as an active comparator.
- rheumatoid arthritis
- dmards (biologic)
- methotrexate
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The landscape of rheumatoid arthritis (RA) treatment has changed dramatically during the last decades. The classical treatment pyramid consisted mainly of rest, physiotherapy, non-steroidal anti-inflammatory drugs and surgery. Disease-modifying antirheumatic drugs (DMARDs) were only used years after diagnosis and after joint destruction and disability had already been established.1 2 Better understanding, however, of the disease and the immunopathogenic mechanisms that drive inflammation in RA has led to a paradigm shift with a reversed pyramid, where new and highly effective DMARDs are introduced as soon as possible after diagnosis is confirmed in order to inhibit radiographic progression due to irreversible joint damage that causes functional disability, chronic pain, early unemployment and poor quality of life.3 4 Earlier diagnosis, early treatment with DMARDs and a well-defined target of therapy combined with a tight evaluation have revolutionised the field and have improved substantially the prognosis of the disease. Herein we attempt to discuss the current evidence about an important but controversial topic, namely whether the use of a biologic DMARD or a targeted synthetic DMARD in combination with methotrexate as the initial treatment might become a possible strategy in the future.
Early treatment and treat-to-target
It is indisputable that treatment should be started as early as possible so as to take advantage of the early period of the disease when underlying inflammation is more susceptible to immunomodulatory treatment than at later time-points, something that has been shown irrespective of therapy.5–7 There are new classification criteria for RA enabling earlier diagnosis of the disease,8 and even recommendations for management of early arthritis.9 However, in real life, there is still significant delay between symptom start and referral to rheumatologist,10 making early intervention difficult.
It is also widely accepted that the goal of RA treatment today should be achieving a state of minimum or no disease activity, that is, remission. Attaining remission minimises joint destruction, improves physical function and quality of life, increases work capacity, and reduces risks for comorbidities, such as cardiovascular comorbidities.11–13 In some patients, especially those with long-standing disease or difficult-to-treat, refractory disease, remission might be impossible and low disease activity might be a more realistic goal. Sustained remission is the logical next goal, especially if this can be achieved in the context of drug discontinuation, the so-called drug-free remission.
Treatment in early RA
The armamentarium of available antirheumatic treatments has increased tremendously during the last years and includes today three major groups of DMARDs: conventional synthetic DMARDs (csDMARDs), with methotrexate being the anchor drug in this category; biologic DMARDs (bDMARDs), targeting cytokines and cells of the immune system that are important players in the immunopathogenesis of RA (five inhibitors of tumor necrosis factor (TNF), rituximab, tocilizumab, abatacept, sarilumab); and targeted synthetic DMARDs (tsDMARDs) (figure 1). The last category includes tofacitinib and baricitinib, two Janus Kinase (JAK) inhibitors that have received approval for the treatment of RA.
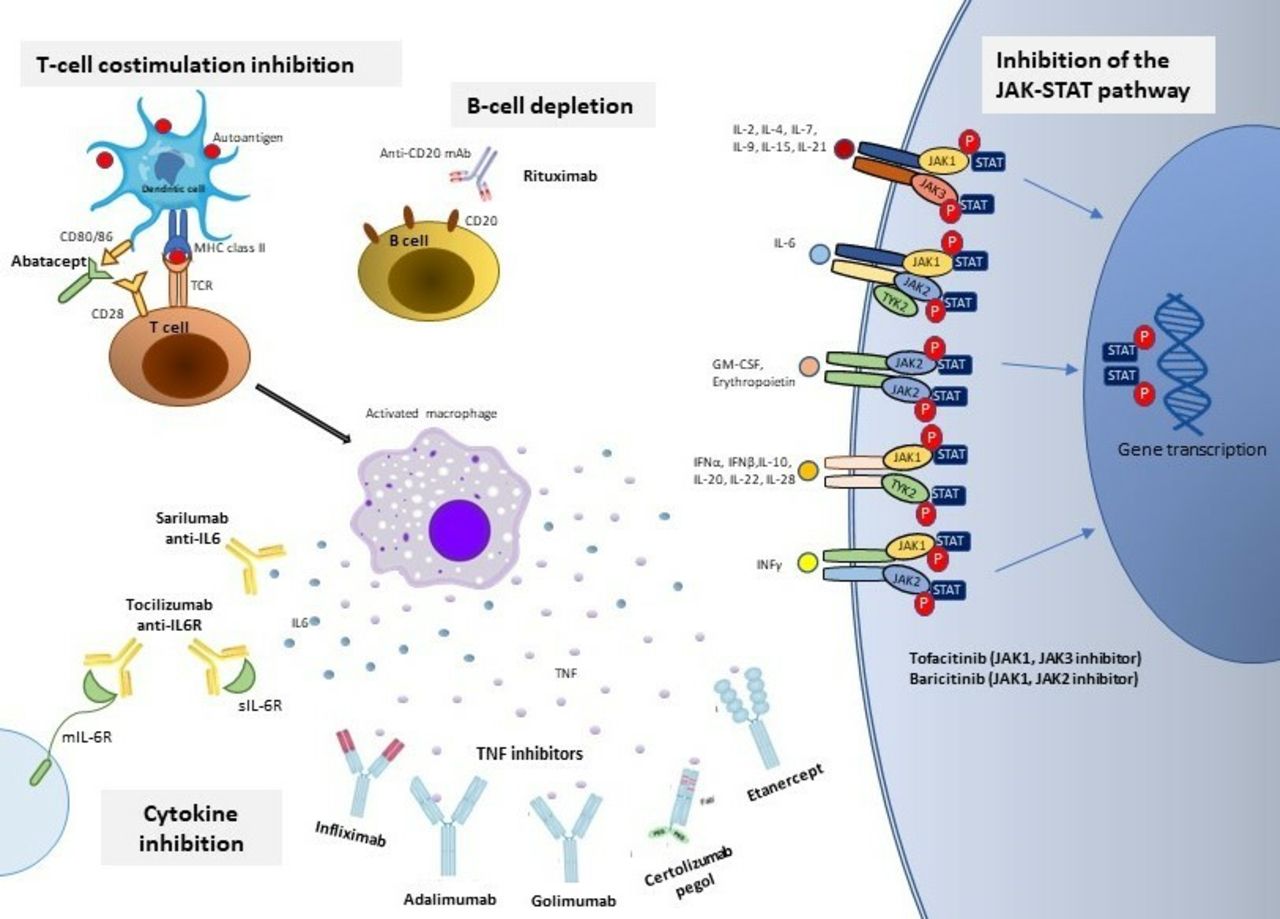
Biologic DMARDs and targeted synthetic DMARDs approved for the treatment of rheumatoid arthritis. DMARDs, disease-modifying antirheumatic drugs; IFN, interferon; IL,interleukin; IL6R, interleukin 6 receptor; INFγ, interferon γ; JAK-STAT, Janus Kinase/Signal Transducer and Activator of Transcription proteins; mAb, monoclonalantibody; MHC, major histocompatibility complex; mIL6R, membraneinterleukin 6 receptor; sIL-6R, soluble interleukin 6 receptor; TCR, T cellreceptor; TNF, tumor necrosis factor.
According to the latest recommendations of EULAR and the American College of Rheumatology, methotrexate should be part of the first treatment strategy.14 Additionally, short-term glucocorticoids should be considered when initiating or changing csDMARDs, in different dose regimens and routes of administration, but should be tapered as rapidly as clinically feasible.14 During the last years, numerous randomised controlled trials (RCTs) have compared head to head methotrexate monotherapy and methotrexate in combination with bDMARDs,15–25 and more recently even tsDMARDs,26 27 in patients with methotrexate-naïve RA. Almost all of these studies have shown superiority of the combination arms to methotrexate monotherapy in patients with RA who have been naïve to methotrexate, although remission was not in all of them the primary outcome. Disease duration varied significantly among these trials, with some of them recruiting patients with very early disease and others with longer disease duration. There is no consensus about the definition of early RA. As we can see from table 1A, 1B, remission rates were generally higher in studies with low disease duration. However, even in those groups, the remission rates with methotrexate alone do not exceed 50%. With combination therapy, methotrexate + bDMARD or tsDMARD in early RA (<1 year), high remission rates of up to 86% can be achieved (table 1A,1B).
Randomised clinical trials of bDMARDs and tsDMARDs in combination with methotrexate compared with methotrexate alone in methotrexate-naïve patients with RA with disease duration <1 year
Randomised clinical trials of bDMARDs and tsDMARDs in combination with methotrexate compared with methotrexate alone in methotrexate-naïve patients with RA with disease duration >1 year
Some of these trials failed to reach the primary outcome, such as the OPERA trial. In the OPERA trial, patients with early RA who were DMARD-naïve were randomised to receive either methotrexate alone or methotrexate in combination with adalimumab. Both groups received intra-articular corticosteroids. The primary outcome was the achievement of low disease activity (DAS28CRP <3.2) at 12 months. Remission (DAS28 <2.6) was one of the secondary endpoints. While a similar percentage of patients in the two groups achieved low disease activity (80% vs 76%, p=0.65), there was a significant difference in remission rates (74% vs 50%, p<0.01). This might suggest that early and more aggressive, treat-to-target treatment strategy with combination treatment from the beginning is superior to monotherapy for achieving more stringent outcomes, such as remission.
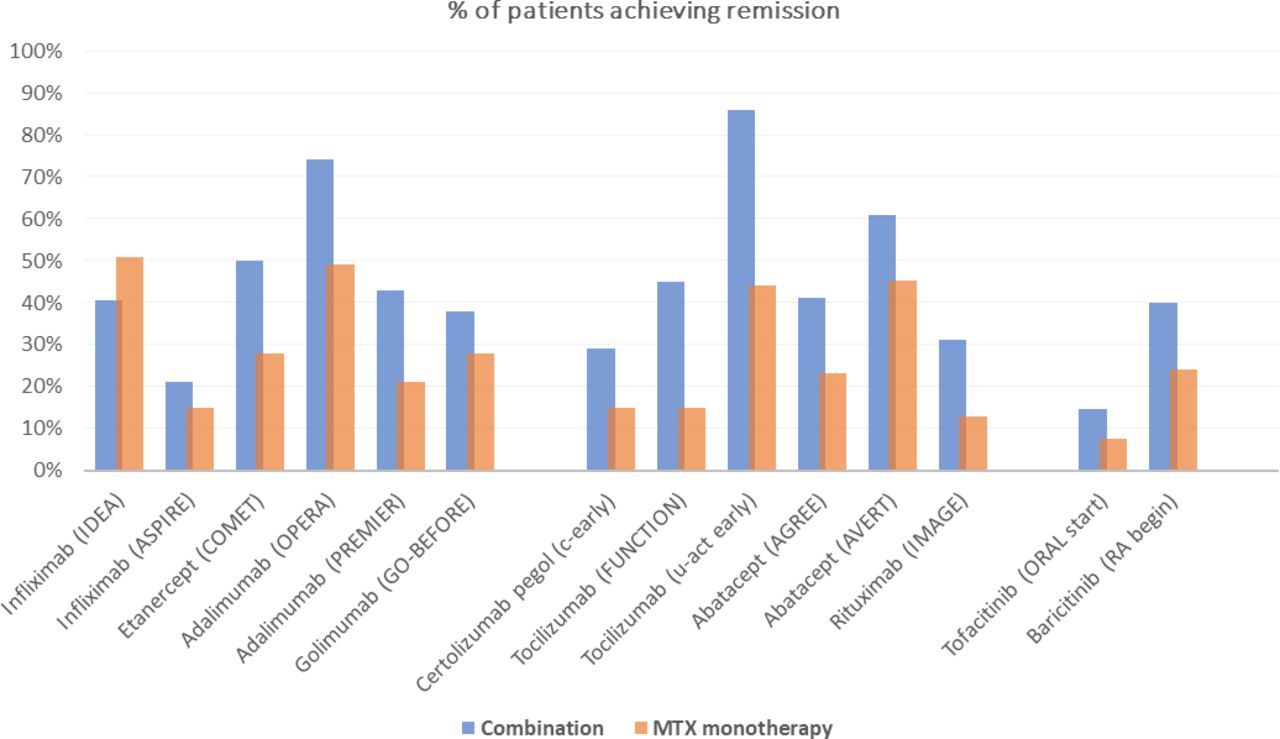
In some of these trials, such as in the tofacitinib ORAL Start trial, the remission rate of methotrexate alone was unexpectedly low (table 1B, figure 2). There are two possible explanations for this observation. First, it is known that the patient population in RCTs is selected and not representative of the whole real-life RA population due to the strict inclusion criteria, which often include high disease activity with high numbers of swollen and tender joints and high acute phase reactants, seropositivity and others. Thus, the external validity of the results is a potential issue. We know that achieving remission is more difficult for patients in high disease activity status at baseline. At the same time, this might support the need to differentiate treatment strategies according to the presence of risk factors for more aggressive disease, even at the initial treatment step in untreated patients. Second, the ORAL Start trial included patients with a mean disease duration of 3 years, which might explain the low frequency of remission both in the methotrexate monotherapy arm and in the combination arm.
{kind=link}
{kind=link}
Percentage of methotrexate-naïve patients with RA achieving remission with methotrexate monotherapy or methotrexate in combination with biologic DMARD or targeted synthetic DMARD. DMARD, disease-modifying antirheumatic drug; MTX, methotrexate; RA, rheumatoid arthritis.
As we mentioned before, short-term glucocorticoids should be added to methotrexate as part of the initial treatment strategy. Limited use of corticosteroids in most of these studies (table 1A,1B) constitutes an important issue regarding the application of the results in real-life practice. Indeed, in trials where glucocorticoids were used as part of the treatment strategy, the results differ from the above, and the difference becomes less evident. In the IDEA trial, treatment-naïve patients with early RA were blindly randomised to receive methotrexate plus infliximab, or methotrexate plus a single-dose intravenous methylprednisolone 250 mg. Both treatment strategies yielded good results without any observed significant difference between them regarding structural damage or clinical efficacy, although a trend towards earlier responses with earlier achievement of DAS28 remission and better synovitis reduction on ultrasound was seen in the methotrexate plus infliximab group.28 In the BeST trial, initial combination treatment consisting of methotrexate plus either a TNF inhibitor (infliximab) or prednisone resulted in earlier clinical improvement and less joint damage progression than monotherapy. Early use of a bDMARD was associated with higher productivity, better quality of life, higher chance of achieving drug-free remission, but also with higher medical costs, as expected.29
Should combination of methotrexate plus bDMARD or tsDMARD be the initial treatment?
The logical question that follows is whether we should consider changing the treatment paradigm starting with a combination treatment consisting of a bDMARD or a tsDMARD and methotrexate, since it is more likely to achieve the goal of remission, according to the trials above.
A number of strategy trials have tried to tackle this important question. In OPTIMA trial, initial treatment with adalimumab in combination with methotrexate was compared with delayed addition of adalimumab to methotrexate, after 26 weeks of methotrexate monotherapy, in those patients who did not achieve low disease activity.30 At week 26 a significantly higher percentage of patients achieved low disease activity when treated with combination treatment compared with methotrexate monotherapy. However, at week 78 the difference between initial and delayed combination treatment did not achieve statistical significance. In the second phase of OPTIMA trial, patients maintained a stable low disease activity even after withdrawal of adalimumab. Following a year of maintenance with methotrexate alone, a significantly higher proportion of patients achieved remission who started on combination therapy compared with monotherapy (27% vs 15%, p<0.0001).
The double-blind RCT HIT HARD also compared two treatment strategies in DMARD-naive patients with early RA, adalimumab in combination with methotrexate or methotrexate alone as initial treatment.31 After the first 24 weeks, adalimumab was discontinued and all patients continued with only methotrexate. At week 24, significantly more patients achieved DAS28 remission in the combination group compared with the monotherapy group (48% vs 30%, p=0.02). At week 48 though, this difference was no longer significant (42% vs 37%, p=0.47), suggesting that induction therapy for 24 weeks with methotrexate plus a Tumor Necrosis Factor inhibitor (TNFi) and with withdrawal of the bDMARD at 24 weeks does not lead to better clinical outcome after 1 year. The results were significantly better though in relation to reduction in radiographic progression.
The GUEPARD trial had a similar design but used a shorter induction period of 12 weeks with adalimumab plus methotrexate in an open design.32 Similarly to the HIT HARD trial, although the combination therapy induced a faster response, it did not achieve a better subsequent (at 1 year) clinical outcome. In this trial, combination treatment did not yield slower progression of structural damage compared with monotherapy.
In the second year of the OPERA trial that we mentioned earlier, adalimumab was discontinued. One year after adalimumab withdrawal, clinical responses did not differ between groups, with remission rates being 69% and 66% in the methotrexate and methotrexate plus adalimumab group, respectively.
A meta-analysis based on some of the trials mentioned above suggested that this induction maintenance approach might have clinical benefits both during the initial induction phase but also after the withdrawal of the TNFi, with a pooled risk ratio for achieving remission of 1.67 (95% CI 1.42 to 1.95) in the induction phase and 1.34 (95% CI 1.05 to 1.89) in the maintenance phase, after discontinuation of the biologic.33
We should acknowledge that a considerable percentage of patients achieve remission on methotrexate alone, which means that using a combination treatment from the beginning would lead to overtreatment of around 30% of patients. We should also take into consideration the safety profile and the high cost of bDMARDs and tsDMARDs.34 The emergence of biosimilars, however, with a reduced cost enables a higher accessibility in some countries and the ‘freedom’ to consider earlier introduction of these very effective but expensive drugs, under the prerequisite that there is medical evidence that there is a true clinical benefit for the patients.
Last, but certainly not least, we should acknowledge the crucial role of glucocorticoid use as part of the combination strategy. As we mentioned above, the current evidence supports combination of methotrexate with short-term glucocorticoids. In the CareRA trial, patients with early RA, but without poor prognostic factors, benefited from the addition of glucocorticoids to methotrexate with no differences in safety observed.35 The percentage of patients achieving remission at week 16 was only numerically but not significantly higher in the combination group (65.1% vs 46.8%, p=0.08). A 2-year prednisone treatment of 10 mg daily on top of tailored weekly methotrexate in the Computer Assisted Management in Early Rheumatoid Arthritis-II trial was very effective and reduced the need for biologics.35 The rate of discontinuation of the glucocorticoids is generally high in these trials. On the other hand, we should also acknowledge the potential side effects of chronic glucocorticoid use, poor patient compliance, and the fact that tight control and stringent treat-to-target principles, which have been applied to the trials, are not always feasible in everyday practice for various reasons, including accessibility to a rheumatology clinic, adherence of rheumatologists to the guidelines and so on.
Conclusion
Data from RCTs show generally low remission rates with methotrexate monotherapy, which fluctuate around 30% in patients with longer than 1 year disease duration and reach a maximum of 50% in patients with early disease (<1 year). Current evidence supports that there might be a clinical and structural benefit of initial, aggressive therapy with a combination of methotrexate and bDMARD or tsDMARD versus methotrexate monotherapy, possibly even associated with a higher chance of remaining in remission, which is the desirable target, after cessation of the bDMARD or the tsDMARD and continuing with a csDMARD alone. This might be a valuable option for the future treatment algorithm of RA, but further confirmation from future strategy trials is needed, especially trials that will include methotrexate plus glucocorticoids as an active comparator. Biomarkers which would identify patients who would benefit more from early combination treatment with bDMARD or tsDMARD, compared with the current recommended strategy of methotrexate plus glucocorticoids, could lead to a more individualised treatment approach and would help us determine the correct place of bDMARDs and tsDMARD in the early RA treatment algorithm.
References
Footnotes
Contributors Both authors contributed to conception, collection of data, analysis and critical interpretation of data, and preparation of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KC has received consultant fees from AbbVie, Pfizer and Lilly. PPS has received consultant fees and research grants from AbbVie, Pfizer, MSD, Roche, UCB, GSK and Novartis.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data are available.