Article Text

Abstract
Objectives This post-hoc analysis explored the impact of body mass index (BMI) on tofacitinib efficacy/safety in patients with active psoriatic arthritis (PsA).
Methods Data were pooled from two phase 3 studies (NCT01877668; NCT01882439). Analyses included patients randomised to tofacitinib 5/10 mg two times a day or placebo, stratified by baseline BMI: <25 kg/m2, ≥25–<30 kg/m2, ≥30–<35 kg/m2 or ≥35 kg/m2. Endpoints (month 3): American College of Rheumatology (ACR20/50/70), Health Assessment Questionnaire-Disability Index (HAQ-DI) and Psoriasis Area and Severity Index (PASI) 75 response rates; dactylitis/enthesitis resolution rates; changes from baseline Short Form-36 Health Survey version 2 (SF-36v2) Physical/Mental Component Summary (PCS/MCS) scores and Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) total score. Safety was also reported.
Results Analysis included 710 patients; 43.8% were obese (BMI ≥30 kg/m2). Tofacitinib demonstrated higher efficacy response rates at month 3, compared with placebo, regardless of baseline BMI. Generally, ACR20/50/70 and HAQ-DI response rates, enthesitis resolution rates and changes from baseline in SF-36v2 PCS score and FACIT-F total score (month 3) were reduced in patients with baseline BMI ≥35 kg/m2 versus patients with lower BMIs. Elevated alanine aminotransferase/aspartate aminotransferase levels were reported in patients with baseline BMI ≥35 kg/m2 receiving tofacitinib 5 mg but not 10 mg two times a day.
Conclusion Tofacitinib demonstrated greater efficacy than placebo in patients with PsA, regardless of baseline BMI. For all treatment arms, reduced efficacy was observed in patients with baseline BMI ≥35 kg/m2. Safety was generally comparable across BMI categories, although the effect of tofacitinib on liver enzymes in patients with baseline BMI ≥35 kg/m2 was inconclusive.
- inflammation
- arthritis
- psoriatic
- autoimmune diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Obesity is prevalent in patients with psoriatic arthritis (PsA) and is associated with a reduced response to tumour necrosis factor inhibitors (TNFi).
What does this study add?
The oral Janus kinase inhibitor tofacitinib demonstrated greater efficacy than placebo in patients with PsA, irrespective of baseline body mass index (BMI).
Efficacy response rates to tofacitinib and placebo were generally reduced in patients with baseline BMI ≥35 kg/m2, compared with patients with a lower baseline BMI.
The safety profile of tofacitinib was largely similar across baseline BMI categories; however, per cent changes from baseline alanine aminotransferase and aspartate aminotransferase levels were greater in patients treated with tofacitinib 5 mg but not 10 mg two times a day in the baseline BMI ≥35 kg/m2 category compared with those in the other baseline BMI categories.
How might this impact on clinical practice?
Our data suggest that tofacitinib can still be considered an effective treatment option for patients with PsA, regardless of their BMI status.
Introduction
Obesity (body mass index (BMI)≥30 kg/m2) poses a significant global health and economic burden.1 Elevated BMI, a surrogate indicator of obesity,2 is a key risk factor for numerous conditions, including cardiovascular disease,3 diabetes mellitus3 and chronic autoimmune disorders such as psoriatic arthritis (PsA).4 5
PsA is a chronic, systemic inflammatory arthritis characterised by involvement of the joints, entheses, skin and nails, and the axial skeleton.6 7 The prevalence of obesity is increased in patients with PsA compared with patients with psoriasis or rheumatoid arthritis (RA) and with the general population.8–10 Furthermore, in a population-based study of ~2 million individuals, obesity was identified as a risk factor for developing PsA in patients with psoriasis and in the general population.4
Treatment options for PsA include: non-steroidal anti-inflammatory drugs; conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), for example, methotrexate, sulfasalazine and leflunomide; biological DMARDs (bDMARDS), for example, tumour necrosis factor inhibitors (TNFi), interleukin (IL)-12/23 inhibitors and IL-17 inhibitors; and targeted synthetic DMARDs, for example, phosphodiesterase inhibitors and Janus kinase (JAK) inhibitors.11 12 Intriguingly, therapeutic response to TNFi was decreased in patients with obesity with PsA compared with patients without obesity.13 14 Moreover, in a meta-analysis of 19 372 patients with various autoimmune conditions, including PsA, patients with obesity were found to have 60% higher odds of failing TNFi therapy versus patients without obesity.15 Weight loss (≥5% from baseline) is associated with higher rates of achieving minimal disease activity (MDA) in overweight patients or patients with obesity with PsA treated with TNFi.16 Accordingly, the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis guidelines recommend maintaining a healthy body weight in patients with PsA to improve TNFi effectiveness.12
Tofacitinib is an oral JAK inhibitor for the treatment of PsA. The efficacy and safety of tofacitinib was demonstrated in phase 3 trials of up to 12 months’ duration in patients with active PsA and an inadequate response to csDMARDs or TNFi therapy,17 18 and for up to 36 months’ duration in a long-term extension study.19 Here, for the first time, we examined the impact of baseline BMI on the efficacy and safety of tofacitinib in patients with active PsA. Understanding the potential effect of BMI on treatment response in patients with PsA may inform therapeutic decision-making in the clinic.
Methods
Patients
This post-hoc analysis pooled data from two randomised, placebo-controlled, double-blind, phase 3 studies (OPAL Broaden (NCT01877668); OPAL Beyond (NCT01882439)) in patients with active PsA.17 18
OPAL Broaden was a 12-month study in patients who had an inadequate response to ≥1 csDMARD and were TNFi-naïve. Patients were randomised 2:2:2:1:1 to receive oral tofacitinib 5 or 10 mg two times a day, adalimumab 40 mg subcutaneously every 2 weeks, or placebo progressing to tofacitinib 5 or 10 mg two times a day at 3 months.17 OPAL Beyond was a 6-month study in patients who had an inadequate response to ≥1 TNFi and were randomised 2:2:1:1 to receive tofacitinib 5 or 10 mg two times a day, or placebo progressing to tofacitinib 5 or 10 mg two times a day at 3 months.18 Throughout both studies, all patients were required to receive a stable dose of one csDMARD (eg, methotrexate, leflunomide or sulfasalazine). Full study details, including patient inclusion and exclusion criteria, have been published previously.17 18 Briefly, eligible patients were aged ≥18 years, had signs and symptoms consistent with a diagnosis of PsA ≥6 months prior to the study and met the Classification Criteria for Psoriatic Arthritis at screening.17 18
The current post-hoc analysis study included all patients from OPAL Broaden and OPAL Beyond who received tofacitinib 5 or 10 mg two times a day, or placebo. Patients were stratified into the following baseline BMI categories according to the WHO2: underweight/normal (<25 kg/m2), overweight (≥25–<30 kg/m2), class 1 obesity (≥30–<35 kg/m2), and class 2 and 3 obesity (≥35 kg/m2).
Both OPAL Broaden and OPAL Beyond were conducted in accordance with the Declaration of Helsinki and Good Clinical Practice Guidelines of the International Conference on Harmonisation, and were approved by the relevant Institutional Review Board and/or Independent Ethics Committee of the investigational centres. All patients provided written, informed consent.
Efficacy outcomes
Efficacy data were pooled at month 3 from OPAL Broaden and OPAL Beyond and stratified by baseline BMI category. Endpoints included: American College of Rheumatology (ACR) 20/50/70% (ACR20/50/70) improvement from baseline in tender and swollen joint counts, and in three of the five remaining ACR core domains (patient’s and physician’s global assessment of arthritis activity, patient’s assessment of arthritis pain, measurement of disability and level of acute-phase reactants); Health Assessment Questionnaire-Disability Index (HAQ-DI) response rate (defined as a ≥0.35-point decrease from baseline, which is considered to be the minimum clinically important difference)20; response rate in achieving ≥75% reduction from baseline Psoriasis Area and Severity Index (PASI75) in patients with baseline body surface area (BSA) ≥3% and PASI >0; dactylitis and enthesitis resolution rates (Dactylitis Severity Score (DSS)=0; Leeds Enthesitis Index (LEI)=0) in patients with baseline DSS >0 and LEI>0, respectively; least squares (LS) mean changes from baseline Short Form-36 Health Survey version 2 (SF-36v2) Physical Component Summary (PCS) and Mental Component Summary (MCS) scores; LS mean change from baseline Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F) total scores; and LS mean change from baseline HAQ-DI scores.
Patients achieved MDA response if they met ≥5 of the following criteria: tender joint count ≤1; swollen joint count ≤1; PASI score ≤1 or BSA ≤3%; patient’s assessment of arthritis pain visual analogue scale (VAS)≤15 mm; patient’s global assessment of arthritis activity VAS≤20 mm; HAQ-DI score ≤0.5; or LEI≤1.
Safety outcomes
Safety data were pooled up to month 3 from OPAL Broaden and OPAL Beyond and stratified by baseline BMI category. Endpoints included adverse events (AEs), changes from baseline in liver function tests and lipid panel parameters.
Statistical analyses
All analyses were performed on the full analysis set, which included patients who were randomised and received ≥1 dose of study treatment.
For the binary efficacy endpoints (ie, response rates), non-responder imputation was used to account for missing values; patients with missing values were treated as non-responders. Observed data were used for continuous efficacy endpoints.
Multivariable analyses were conducted to evaluate the possible association between baseline BMI (as a continuous or categorical variable) and the efficacy endpoints: ACR20/50/70, HAQ-DI and PASI75 response rates, and change from baseline in HAQ-DI, LEI and DSS. For each tofacitinib treatment group, a multivariable logistic regression analysis for binary endpoints and multivariable regression analysis for continuous endpoints were conducted, to determine significant predictors for each efficacy endpoint based on a backward selection method using a 5% level of significance. Separate models were run using categorical BMI and continuous BMI as covariates. Other baseline covariates included: age, race, gender, region, weight, smoking status, disease duration, prior bDMARD use, FACIT-F total score, LEI, DSS, C-reactive protein (CRP), metabolic syndrome, corticosteroid use, prior TNFi use, pain VAS, HAQ-DI, SF-36v2 PCS and SF-36v2 MCS. No multiplicity adjustment was performed in this post-hoc analysis. Safety endpoints were analysed descriptively.
Results
Patients
In total, 710 patients (OPAL Broaden, n=316; OPAL Beyond, n=394) were included in this post-hoc analysis, 311 (43.8%) of whom were obese. Of these, 186 had a BMI ≥30–<35 kg/m2, and 125 had a BMI ≥35 kg/m2. The majority of patients were middle-aged, female and Caucasian (table 1). Slightly more female patients were randomised to the <25 kg/m2 and ≥35 kg/m2 baseline BMI categories compared with patients in the other baseline BMI categories. Metabolic syndrome and elevated CRP levels (>2.87 mg/L) were more frequent in patients with baseline BMI ≥35 kg/m2 versus those with a lower baseline BMI (table 1). Higher HAQ-DI scores, tender and swollen joint counts and lower SF-36v2 PCS scores were observed in patients in the baseline BMI ≥35 kg/m2 category, compared with patients in the other baseline BMI categories. Additionally, prior use of one bDMARD was more prevalent in patients with baseline BMI ≥35 kg/m2 versus those with a lower baseline BMI.
Patient demographics and baseline disease characteristics by baseline body mass index (BMI) category (pooled data from OPAL Broaden and OPAL Beyond)
Patient demographics and baseline disease characteristics by baseline BMI category and treatment are shown in online supplemental table 1.
Supplemental material
Efficacy outcomes by BMI category
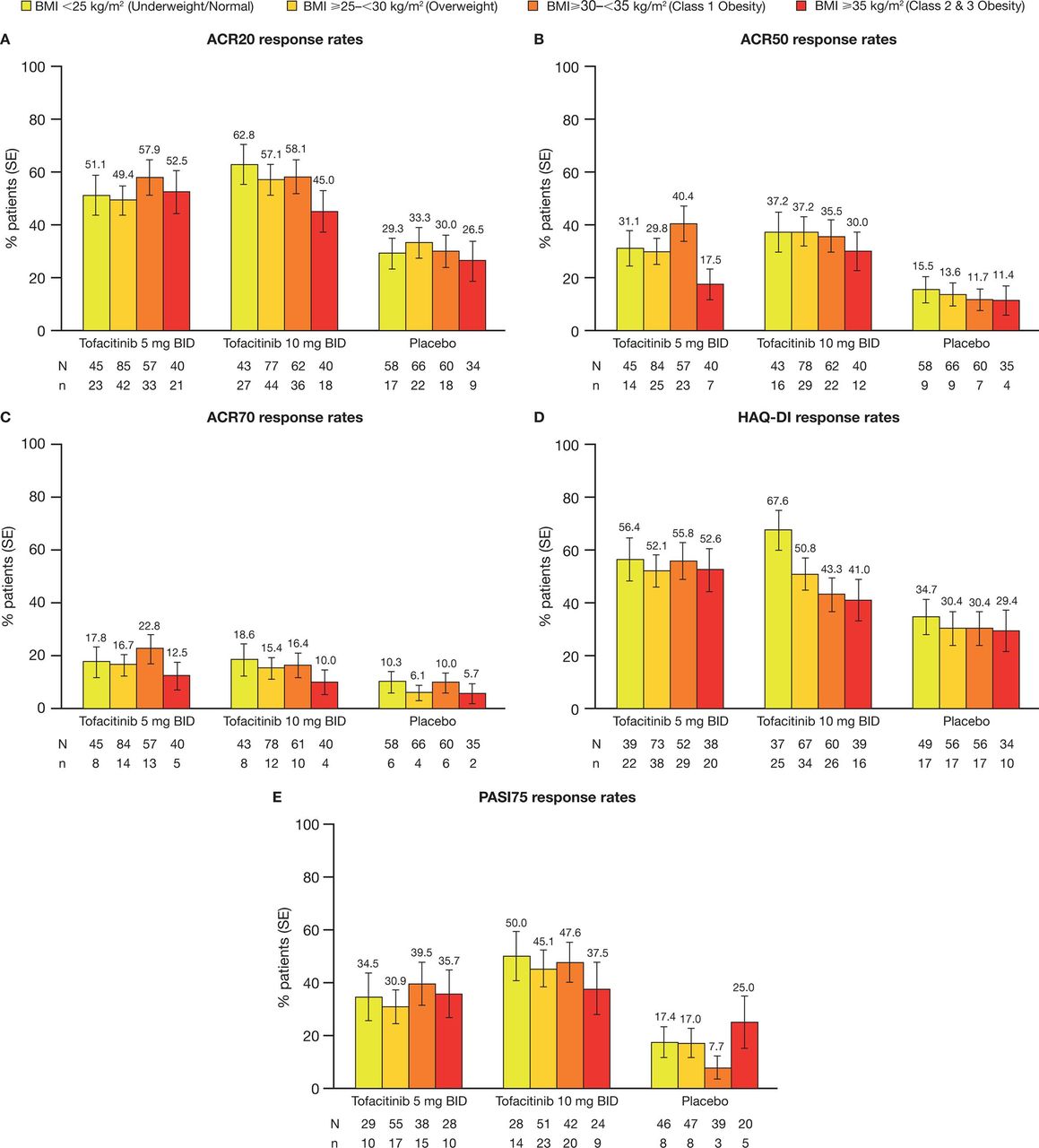
Consistent with the main findings of OPAL Broaden and OPAL Beyond, ACR20/50/70, HAQ-DI and PASI75 response rates at month 3 were higher in tofacitinib-treated patients, compared with placebo-treated patients, across all baseline BMI categories (figure 1). In all treatment groups, response rates were generally lower in patients in the baseline BMI ≥35 kg/m2 category, compared with patients in the other baseline BMI categories, particularly when treated with tofacitinib 10 mg two times a day (figure 1). In patients treated with placebo, the PASI75 response rate was higher in patients in the baseline BMI ≥35 kg/m2 category, compared with patients in the other baseline BMI categories (figure 1E). It should be noted that PASI75 response rate was only assessed in patients with baseline BSA ≥3% and PASI >0, and patient numbers were lower than those for the ACR20/50/70 and HAQ-DI response rates.

Response rates at month 3 for (A) ACR20,* (B) ACR50,* (C) ACR70,* (D) HAQ-DI† and (E) PASI75‡ by baseline BMI category and treatment group (pooled data from OPAL Broaden and OPAL Beyond). N indicates the number of patients with non-missing BMI evaluable at month 3; n indicates the number of responders. All patients received a stable dose of one csDMARD throughout each study. *ACR20/50/70 response rates were defined as the proportions of patients achieving a ≥20/50/70% improvement from baseline in tender and swollen joint counts and ≥20/50/70% improvement from baseline in three of the five remaining ACR core measures. †HAQ-DI response rate was defined as the proportion of patients achieving a reduction from baseline HAQ-DI of ≥0.35, considered the minimum clinically important difference. ‡PASI75 response rate was defined as the proportion of patients achieving a reduction from baseline PASI of ≥75%, assessed only in patients with baseline BSA ≥3% and a baseline PASI>0. ACR20/50/70, American College of Rheumatology≥20/50/70% response criteria; BID, two times a day; BMI, body mass index; BSA, body surface area; csDMARD, conventional synthetic disease-modifying antirheumatic drug; HAQ-DI, Health Assessment Questionnaire-Disability Index; PASI75, ≥75% Psoriasis Area and Severity Index improvement from baseline.
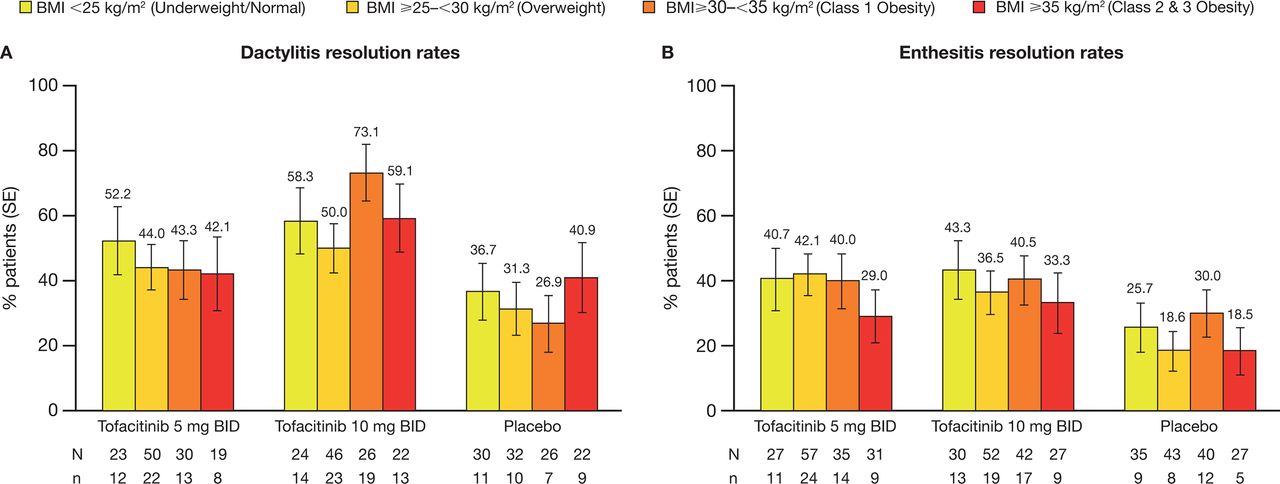
Consistent with the main findings of OPAL Broaden and OPAL Beyond, dactylitis and enthesitis resolution rates at month 3 were higher in tofacitinib-treated patients, compared with placebo-treated patients, across all baseline BMI categories (figure 2). The dactylitis resolution rate was numerically higher in placebo-treated patients with baseline BMI ≥35 kg/m2, compared with placebo-treated patients in the other baseline BMI categories (figure 2A). Across all baseline BMI categories, the dactylitis resolution rate was increased in patients treated with tofacitinib 10 mg two times a day versus those treated with tofacitinib 5 mg two times a day or placebo (figure 2A). Patients with baseline BMI ≥35 kg/m2 exhibited lower enthesitis resolution rates, compared with patients in the other baseline BMI categories, regardless of treatment (figure 2B).
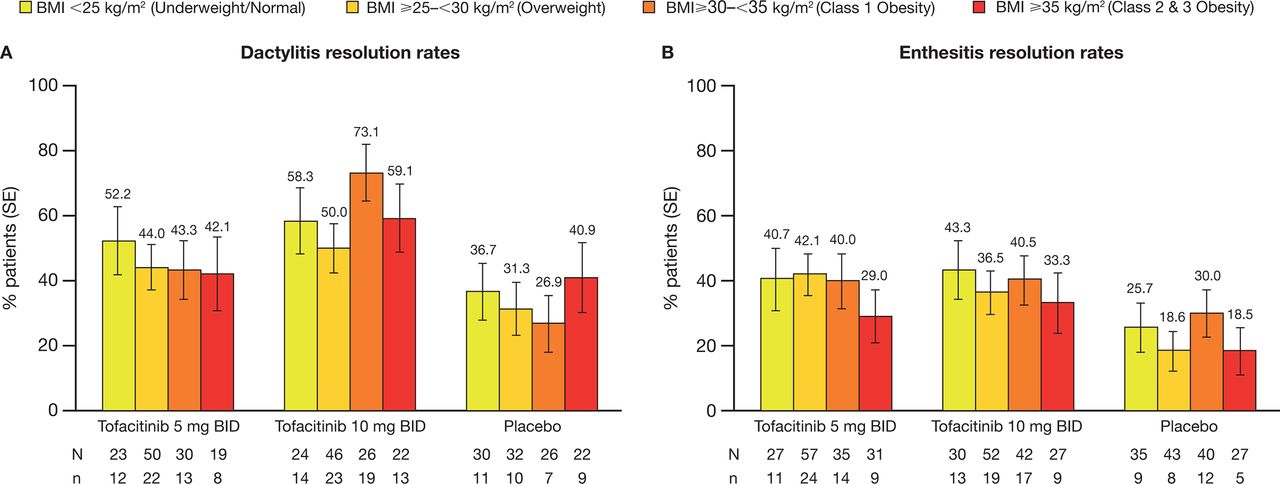
Resolution rates at month 3 for (A) dactylitis* and (B) enthesitis† by baseline BMI category and treatment group (pooled data from OPAL Broaden and OPAL Beyond). N indicates the number of patients with non-missing BMI evaluable at month 3; n indicates the number of responders. All patients received a stable dose of one csDMARD throughout each study. *Dactylitis resolution rates, defined as the absence of dactylitis in all of the 20 assessed digits, assessed only in patients with baseline DSS >0. †Enthesitis resolution rates, defined as the absence of enthesitis in all of the six assessed sites, assessed only in patients with baseline LEI >0. BID, two times a day; BMI, body mass index; csDMARD, conventional synthetic disease-modifying antirheumatic drug; DSS, Dactylitis Severity Score; LEI, Leeds Enthesitis Index.
Overall, patients treated with tofacitinib 5 and 10 mg two times a day exhibited greater mean changes from baseline SF36v2 PCS and MCS scores, FACIT-F total scores and HAQ-DI at month 3, compared with patients treated with placebo (figure 3). Patients in the baseline BMI ≥35 kg/m2 category treated with tofacitinib 5 or 10 mg two times a day exhibited lower mean changes from baseline SF-36v2 PCS score and FACIT-F total score, compared with patients in the other baseline BMI categories (figure 3A,C).

{kind=link}
{kind=link}
{kind=link}
LS mean (SE) changes from baseline at month 3 in (A) SF-36v2 PCS score, (B) SF-36v2 MCS score, (C) FACIT-F total score and (D) HAQ-DI by baseline BMI category and treatment group (pooled data from OPAL Broaden and OPAL Beyond). N indicates the number of patients with non-missing BMI evaluable at month 3; n indicates the number of responders. All patients received a stable dose of one csDMARD throughout each study. Δ, change from baseline; BID, two times a day; BMI, body mass index; csDMARD, conventional synthetic disease-modifying antirheumatic drug; FACIT-F, Functional Assessment of Chronic Illness Therapy-Fatigue; HAQ-DI, Health Assessment Questionnaire-Disability Index; LS, least squares; MCS, Mental Component Summary; PCS, Physical Component Summary; SF-36v2, Short Form-36 Health Survey version 2.
Multivariable analyses with BMI as both a categorical and continuous variable demonstrated that BMI was not a significant predictor of response across most efficacy endpoints at month 3, and across both tofacitinib treatment groups (online supplemental table 2). However, in patients treated with tofacitinib 5 mg two times a day, BMI was a significant predictor of response for: ACR50 response (BMI categorical; p=0.035), ACR70 response (BMI categorical (p=0.023) and continuous (p=0.002)), MDA rate (BMI categorical (p=0.048) and continuous (p=0.003)), and change from baseline at month 3 in HAQ-DI (BMI continuous; p=0.050).
Safety outcomes by BMI category
Online supplemental table 3 shows AEs reported in ≥5% of patients up to month 3 for each treatment group across baseline BMI categories. The most common AEs were similar to past reports17 18; falls, constipation, dizziness, bronchitis and dry skin were reported more frequently among patients with baseline BMI ≥35 kg/m2. Up to month 3, three cardiovascular events were reported: a non-fatal cerebrovascular accident and a transient ischaemic attack (both occurring in the same patient; tofacitinib 5 mg two times a day; baseline BMI ≥30–<35 kg/m2) and a coronary artery revascularisation (patient received placebo; baseline BMI ≥35 kg/m2). One patient treated with tofacitinib 5 mg two times a day in the baseline BMI ≥30–<35 kg/m2 category had an arterial thromboembolic event. Those that experienced cardiovascular and thromboembolic events were found to have a history of hypertension, coronary heart disease, abnormal ECGs or angina. In this dataset, no deep vein thrombosis or pulmonary embolism events were reported up to month 3.
At month 3, per cent changes from baseline alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels were greater in patients treated with tofacitinib 5 and 10 mg two times a day, compared with patients treated with placebo, regardless of BMI category (table 2). Among patients treated with tofacitinib 5 mg two times a day, per cent changes in ALT and AST levels were notably greater in the baseline BMI ≥35 kg/m2 category than in the other baseline BMI categories; among patients treated with tofacitinib 10 mg two times a day, per cent changes in ALT and AST levels were greater in the baseline BMI ≥25–<30 kg/m2 category than in the other baseline BMI categories. Generally, observations were similar for absolute liver enzyme levels (table 2).
Liver enzyme and lipid panel parameters at month 3, by baseline BMI category and treatment group
For most BMI categories, per cent changes from baseline at month 3 in low-density lipoprotein, high-density lipoprotein, total cholesterol and triglyceride levels were greater in tofacitinib-treated patients, compared with placebo-treated patients. However, per cent changes from baseline triglyceride levels were higher in patients treated with placebo, compared with patients treated with tofacitinib 5 mg two times a day in the baseline BMI <25 kg/m2 category, and tofacitinib 5 and 10 mg two times a day in the baseline BMI ≥30–<35 kg/m2 category (table 2). Among patients treated with tofacitinib 5 mg two times a day, per cent change from baseline triglyceride levels was notably lower in the baseline BMI <25 kg/m2 category versus the other baseline BMI categories.
Discussion
This post-hoc analysis investigated the impact of baseline BMI on tofacitinib efficacy and safety in patients with active PsA. Tofacitinib 5 and 10 mg two times a day demonstrated higher efficacy response rates at month 3, compared with placebo, regardless of baseline BMI. Patients in the baseline BMI ≥35 kg/m2 category had more active disease (eg, elevated CRP levels (>2.87 mg/L) and higher tender/swollen joint counts) at baseline compared with patients in the other baseline BMI categories. For tofacitinib and placebo treatment arms, efficacy response rates were generally reduced in patients with baseline BMI ≥35 kg/m2 compared with patients with lower baseline BMIs. Additionally, baseline BMI was found to be a significant predictor of response for ACR50/70 and MDA rates, and change from baseline in HAQ-DI at month 3 in patients receiving tofacitinib 5 mg (but not 10 mg) two times a day. Up to month 3, there were no notable differences in the safety profile of tofacitinib between baseline BMI categories; however, the per cent changes from baseline ALT and AST levels were greater in patients treated with tofacitinib 5 mg (but not 10 mg) two times a day in the baseline BMI ≥35 kg/m2 category, compared with patients in the other baseline BMI categories.
Elevated ALT and AST levels in patients with baseline BMI ≥35 kg/m2 treated with tofacitinib 5 mg but not 10 mg two times a day provide limited evidence for an effect of tofacitinib on the liver enzymes of this BMI cohort. The small sample size within each tofacitinib arm (tofacitinib 5 mg two times a day, n=42; tofacitinib 10 mg two times a day, n=43) of the baseline BMI ≥35 kg/m2 category may have led to this random finding, although there could be other putative explanations. For example, undiagnosed non-alcoholic fatty liver disease, which is prevalent in obesity,21 might have contributed to the elevated ALT and AST levels in patients with baseline BMI ≥35 kg/m2 treated with tofacitinib 5 mg two times a day; although baseline ALT and AST levels in patients in the BMI ≥35 kg/m2 category were relatively similar to those in patients in the other baseline BMI categories. Furthermore, there were no notable differences in baseline disease characteristics or prior/baseline/concomitant treatments between BMI categories (or study treatment arms) that could account for the elevated liver enzyme levels observed in patients with baseline BMI ≥35 kg/m2 receiving tofacitinib 5 mg two times a day.
Overall, for most lipid panel measures, the per cent changes from baseline at month 3 were greater in patients treated with tofacitinib than in those treated with placebo, regardless of baseline BMI. Small increases in cholesterol, low-density lipoprotein, high-density lipoprotein and triglyceride levels have been reported previously in patients with moderate to severe psoriasis treated with tofacitinib at week 16.22 Accordingly, blockade of IL-6, a downstream target of tofacitinib,23 is associated with increased low-density lipoprotein levels in patients with RA.24 Although obesity is associated with dyslipidaemia,25 we observed no notable relationship between BMI and per cent changes from baseline lipid panel measures in response to tofacitinib.
In obese individuals, adipocyte hypertrophy can lead to overproduction of proinflammatory cytokines (eg, TNF-α and IL-6) which may increase the risk and severity of inflammatory disorders.26–29 Accordingly, there is an increased prevalence of obesity among patients with PsA.8–10 Moreover, patients with obesity with PsA have been shown to exhibit higher Disease Activity Score 28 and pain scores, compared with patients without obesity.14 The ongoing PsABio study (NCT02627768), including patients with PsA from eight European countries, recently reported an association between elevated BMI and higher clinical Disease Activity in Psoriatic Arthritis, Psoriatic Impact of Disease-12 and HAQ-DI scores.30 Here, increased baseline BMI (≥35 kg/m2) was generally associated with increased tender and swollen joint counts, PASI75 and HAQ-DI scores, elevated CRP (>2.87 mg/L) and decreased SF-36v2 PCS scores at baseline. Additionally, among placebo-treated patients, those with a baseline BMI ≥35 kg/m2 typically exhibited reduced efficacy response rates at month 3, compared with those in lower baseline BMI categories.
Tofacitinib inhibits the downstream signalling of several JAK-dependent cytokines, including TNF-α and IL-623; it is, therefore, possible that the therapeutic effectiveness of tofacitinib is attenuated by the elevated expression of proinflammatory cytokines in patients with obesity. Accordingly, among patients treated with tofacitinib 5 mg and 10 mg two times a day, those with a baseline BMI ≥35 kg/m2 generally experienced reduced efficacy response rates at month 3, versus those with lower baseline BMIs. Interestingly, an analysis of pooled data from two phase 3 studies in patients with RA treated with the JAK inhibitor baricitinib revealed reduced ACR20/50/70 response rates after 12 weeks in patients with baseline BMI >30.7 kg/m2, compared with those with lower baseline BMIs.31 Additionally, patients with obesity (BMI ≥30 kg/m2) with RA were reported to have reduced rates of achieving low disease activity and remission compared with normal weight (BMI <25 kg/m2) and overweight (BMI ≥25–<30 kg/m2) patients at 6 months after commencing baricitinib or tofacitinib treatment.32 It should be noted that tofacitinib has been shown to be efficacious versus placebo, in patients with PsA in the current study, and in patients with RA,33 regardless of BMI.
It is also noteworthy that pooled analyses of phase 3 studies in patients with RA33 and ulcerative colitis34 receiving tofacitinib 5 or 10 mg two times a day, or placebo, revealed similar efficacy outcomes across all treatment groups, regardless of baseline BMI category; however, these analyses included three BMI categories (<25 kg/m2, 25–<30 kg/m2 and ≥30 kg/m2) and the current analysis included a fourth BMI category (≥35 kg/m2), so a direct comparison with this analysis is limited.
Tofacitinib has moderate lipophilicity. Analysis of pharmacokinetic parameters for tofacitinib demonstrated that while increased body weight results in lower peak (Cmax) and higher trough (Cmin) plasma concentrations, it has no clinically relevant impact on total drug exposure (AUC); therefore, no dose adjustment is recommended for tofacitinib based on patients’ body weight.35 The reduced efficacy response to tofacitinib in patients with baseline BMI ≥35 kg/m2 could be due to a larger volume of distribution, which can lower plasma concentrations. Body weight has been shown to influence the PK profile of biological agents, including TNFi, in various immune disorders.36–38 In a population PK study in patients with chronic inflammatory diseases, including PsA, treated with the TNFi infliximab, drug volume of distribution and clearance increased with body weight.37
In patients with obesity, increased immunogenicity and elevated drug clearance may account for the effect of high body weight on decreased efficacy of TNFi and other biological agents.15 39 A study in patients with PsA, RA and controls without rheumatic disease (n=89) reported increased adipose expression of inflammatory genes in patients with PsA, compared with patients with RA or controls, across all BMI categories. Additionally, patients treated with biologics expressed high adipose levels of inflammatory genes regardless of baseline BMI.40
Interestingly, although obesity is associated with a slight attenuated therapeutic response to TNFi and JAK inhibitors in patients with PsA and RA,13–15 31 the response to the IL-6 inhibitor tocilizumab in patients with RA was reported to not be affected by high baseline BMI.41 However, IL-6 inhibitors are not indicated for the treatment of PsA. The reasons why TNFi and JAK inhibitors have reduced effectiveness in patients with obesity compared with other drugs are poorly understood; however, PK properties, volume of distribution and lipophilicity may be contributing factors.42 It is also possible that, due to the inflammatory processes associated with obesity,26–29 higher doses of TNFi or JAK inhibitors are required to treat individuals with an elevated BMI, compared with those with lower BMIs.
Current ACR guidelines for the treatment of PsA recommend weight loss in overweight patients or patients with obesity to potentially improve pharmacologic responses.43 Correspondingly, in patients with obesity with PsA, weight loss has been reported to improve disease activity in a dose-dependent manner.44
A limitation of this research is that the analysis was post-hoc, and comparisons between tofacitinib and placebo treatment groups were limited to the 3-month, placebo-controlled portion of the OPAL Broaden and OPAL Beyond studies; further research is required to evaluate the long-term impact of BMI on treatment response to tofacitinib in patients with PsA in the real world. No adjustments for multiple comparisons were performed for this analysis; therefore, chance findings cannot be ruled out. In addition, small numbers of patients in the treatment and BMI strata limit the breadth of the conclusions that can be made from these analyses. Measures of peripheral proinflammatory molecules, such as IL-6 or leptin were not part of the study design and may have provided additional insight into the study results.
Conclusions
Across all baseline BMI categories, tofacitinib demonstrated higher efficacy in patients with PsA at month 3, compared with placebo. However, similar to TNFi therapy,13–15 reduced efficacy was generally observed in tofacitinib-treated and placebo-treated patients with baseline BMI ≥35 kg/m2, compared with patients in the other baseline BMI categories. In general, tofacitinib safety appeared similar across all baseline BMI categories up to month 3, although the effect of tofacitinib on liver enzymes in patients with baseline BMI ≥35 kg/m2 was inconclusive.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at Data in this manuscript were previously presented at the ACR/ARP 2019 Annual Meeting (Ritchlin C, Ogdie A, Giles J, et al. Arthritis Rheumatol 2019;71 [Suppl 10]:1513).
Contributors All authors provided critical revision of the manuscript. All authors interpreted the results, approved the final draft, and had the final decision to submit the manuscript for publication. Pfizer did not control the analysis or interpretation of the study results. Publication of this article was not contingent upon approval by Pfizer.
Funding This study was sponsored by Pfizer. Medical writing support, under the guidance of the authors, was provided by Dominic Singson, MD, and Emma Mitchell, PhD, CMC Connect, McCann Health Medical Communications and was funded by Pfizer, New York, New York, USA in accordance with Good Publication Practice (GPP3) guidelines (Ann Intern Med 2015;163:461–4).
Competing interests JTG has received research grants from Pfizer; and consultancy fees from AbbVie, Bristol-Myers Squibb, Eli Lilly, Genentech, Gilead and UCB. AO has received research grants from Amgen (to Forward/National Databank), Novartis (to the University of Pennsylvania) and Pfizer Inc (to the University of Pennsylvania); and consultancy fees from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Corrona, Eli Lilly, Janssen, Novartis, Pfizer, Takeda Pharmaceutical Company and UCB. AO’s husband has received royalties from Novartis. JJG-R has received funding from Pfizer. PSH has received research grants from AbbVie, Janssen and Novartis; and honoraria from AbbVie, Amgen, Celgene, Galapagos, Janssen, Pfizer and UCB. RG, LS, PY, WJ, RM and DG are employees and shareholders of Pfizer. CR has received research grants from AbbVie, Amgen and UCB; and consultancy fees from AbbVie, Amgen, Bristol-Myers Squibb, Eli Lilly, Janssen, Novartis, Pfizer and UCB.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Upon request, and subject to certain criteria, conditions and exceptions (see https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information), Pfizer will provide access to individual deidentified participant data from Pfizer-sponsored global interventional clinical studies conducted for medicines, vaccines and medical devices (1) for indications that have been approved in the US and/or EU, or (2) in programmes that have been terminated (ie, development for all indications has been discontinued). Pfizer will also consider requests for the protocol, data dictionary and statistical analysis plan. Data may be requested from Pfizer trials 24 months after study completion. The deidentified participant data will be made available to researchers whose proposals meet the research criteria and other conditions, and for which an exception does not apply, via a secure portal. To gain access, data requestors must enter into a data access agreement with Pfizer.