Article Text

Abstract
Background Patients recently diagnosed with rheumatoid arthritis (RA) have specific educational and supportive needs. These could partly be addressed with mentoring by other patients living with RA. This qualitative study explores stakeholder perceptions towards peer mentoring in early RA care.
Methods Two focus groups with patients with early RA (n=10), one with patient organisation representatives (n=5), one with rheumatologists (n=8) and one with rheumatology nurses (n=5) were held. Two patient research partners supported analysis and interpretation.
Results Four overarching themes were found: added value, experience with peer mentoring, concerns and need in daily care. Patients and patient organisation representatives confirmed the potential of peer mentoring especially regarding sensitive topics not easily discussed with professionals. Patients felt it could provide additional understanding and recognition. Nurses and rheumatologists were less convinced of the added value of peer mentoring because patients never mentioned it and they were concerned about the loss of control over correct information provision. The need for peer mentoring was perceived as person and disease phase-dependent and should therefore be optional, rather than a care standard. The requirements for a peer mentorship programme remained challenging to define for stakeholders. However, all expressed the need for supervision by healthcare professionals and that peer mentors should be carefully selected, educated and matched to newly diagnosed patients.
Conclusion Peer mentoring and its implementation remain vague concepts, especially for healthcare providers. However, patients are interested in mentoring by peers, and the current results may support in effectively implementing such programmes early in the disease.
- rheumatoid arthritis
- qualitative research
- patient care team
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. The data source is available on reasonable request to the authors.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Studies have found benefits for peer mentoring in chronic inflammatory rheumatic conditions. Peer mentoring, especially in the early vulnerable phase of the disease, could contribute to an improved disease management for patients with rheumatoid arthritis (RA). However, perspectives on peer mentoring in the care for patients with early RA remain largely unknown.
What does this study add?
The concept of peer mentoring remains vague in this qualitative study among four key stakeholder groups, including patients with early onset RA, patient organisation representatives, rheumatologists and rheumatology nurses. While patients and patient organisation representatives did feel that peer mentoring has potential, nurses and particularly rheumatologists saw less immediate benefits in a peer-mentoring programme, since they assumed that they would have limited control over it.
Appropriate education, selection, coaching and supervision of peer mentors was considered essential as well as matching them to specific patients and integrating them in the multidisciplinary care team.
How might this impact on clinical practice or further developments?
Successful Implementation of a peer mentoring programme will require a shift in sentiment towards peer mentorship by healthcare providers. Key seems to be appropriate training of the peer mentor and the integration of the peer mentor in the multidisciplinary care team.
Introduction
The early phase of rheumatoid arthritis (RA) is an important period from a therapeutical perspective1 2 but also poses additional and specific challenges to patients.3 4 They are confronted with the diagnosis of a chronic disease, and often struggle at first to grasp how this will impact their lives. This phase can, therefore, represent a significant psychological burden.5 Patients with inflammatory arthritis, and specifically those with recent disease onset, require an individually tailored and needs-based educational programme, as recommended by the European League Against Rheumatism (EULAR) as an integral part of the standard of care.2 A study using the Dutch Educational Needs Assessment Tool (ENAT) indicated that educational needs may differ among patients with RA, especially with varying age and disease duration.4 Moreover, evidence has shown that needs-based education in RA helps to improve self-efficacy and specific aspects of reported health.6 The recently updated EULAR-guidelines for the management of RA confirm education as an ‘implicit and inseparable basis for shared decision making in therapy’.2 However, a recent study from the Netherlands suggests there is room for improvement in its implementation.7 This indicates a need to better understand the patient perspective, to improve education and to contribute to patient centricity in daily practice.
A possible strategy to improve patient education could be provided by peer mentoring. Peer mentoring introduces patients as coaches or mentors who can share their disease experience and views with other patients affected by the same condition.8 This way, the knowledge, skills and experience of these peer mentors can be used as a complementary method of patient education. Moreover, peer mentors could harmonise disease perceptions and address discrepancies in disease outcome perceptions between healthcare professionals and their patients.9 Positive effects of peer mentoring have been demonstrated in several chronic diseases, such as chronic kidney disease, diabetes mellitus, hypertension and HIV/AIDS.10–17 The concept of peer-mentorship has to date been implemented in many different forms in practice. In previous peer-mentorship studies, interventions have been organised either individually or in groups, via personal or telephone contact and at various locations (hospital, home setting or community centre), and the training and role of peer mentors was often very diverse.13 18–20
In the rheumatic diseases, there are surprisingly few studies relating to peer mentoring, although preliminary evidence suggests possible benefits in ankylosing spondylitis,17 juvenile idiopathic arthritis,21 inflammatory arthritis22 and RA.23 Only one pilot study by Sandhu et al24 investigated the feasibility and potential benefits of peer mentoring in RA. However, this study did not examine peer mentoring from the perspective of the different stakeholders, which could be considered a crucial element in light of the successful implementation of peer-mentoring programmes.25
Therefore, we performed a qualitative study to explore the need for and attitudes towards peer mentoring in the care for patients with early RA among four key stakeholder groups, including patients with early onset RA, patient organisation representatives, rheumatologists and rheumatology nurses. Additionally, we aimed to gather ideas for the content and format of a peer mentoring programme in clinical practice.
Patients and methods
This study was carried out in Flanders, Belgium, using a qualitative research design with focus groups.26
Participants
Four groups of stakeholders were included in this study: patients with early RA, patient organisation representatives, rheumatologists and rheumatology nurses. All included participants were required to understand and speak Dutch.
Recruitment of patients: Four rheumatologists were asked to recruit two men and two women with early RA by informing their consecutive patients about the study during a routine consultation. Early RA was defined as a maximum disease duration 24 months since diagnosis. Patients were recruited from one academic and two non-academic centres from two Belgian provinces. Patients who showed interest were asked to sign the informed consent form, after which the contact details of the interested patients were shared with the research team.
Recruitment of patient organisation representatives: Three Flemish patient organisations were purposefully selected, based on their current contributions in the field of RA, and asked to recruit two of their interested active core members.
Recruitment of rheumatology nurses: Rheumatology nurses were invited via the Belgian rheumatology nurses working group. Only those nurses actively involved in the care for patients with rheumatic diseases could participate.
Recruitment of rheumatologists: Practising rheumatologists were invited through a mandatory local peer quality group. These rheumatologists were active in private practices, academic and non-academic hospitals, all in the same region.
Patient research partners
We recruited two patient research partners involved in this study (LDC and IL). At the beginning of the study, we introduced them to the concept of peer mentoring, and they received specific training in qualitative data analysis. They were involved in the development of the interview guide, coding of the transcripts, data interpretation and the description of the results, and they also participated in peer debriefings as part of the interdisciplinary research team. Collaboration with these patient research partners was based on the FIRST-framework of Hewlett et al.27
Data collection
Between December 2015 and May 2017, one moderator (LB) and two participating observers (LP, KVdE) conducted semistructured face-to-face focus groups. The interview guide included open-ended and probing questions and its content was based on literature review on peer mentoring and critical input of two patient research partners (LDC and IL). For each stakeholder group, the interview guide was adjusted to fit with their profile (eg, the question ‘How could a peer mentor support your daily practice?’ was not asked to patients). Focus groups were audiorecorded and transcribed verbatim.
A questionnaire was given to each participant to gather key characteristics per individual.
For each focus group, observational notes related to participants’ behaviour, interaction between participants and remarkable quotations were prepared to be used as contextual information when interpreting the data.28
Data analysis
The analysis was carried out in accordance with the Qualitative Analysis Guide Of Leuven (QUAGOL), which is based on the principles of grounded theory, as a tool to work systematically and according to the principle of constant comparison.28 The transcripts were independently coded by three researchers (LB, LP and KVdE) and two patient research partners (IL and LDC), and these codes were further discussed and refined during peer debriefings. The final codes were discussed until agreement by the interdisciplinary research team consisting of two rheumatologists (RW and PV) one nurse specialist (KVdE), the patient research partners and the other researchers included as co-authors.
Results
Five focus groups with a total of 28 participants were organised: two with patients with early RA, one with patient organisation representatives, one with rheumatologists and one with rheumatology nurses. Table 1 presents the participant characteristics per stakeholder group.
Participant characteristics per stakeholder group
Perceptions of stakeholders on peer mentorship
The conceptual synthesis of the focus groups resulted in four overarching themes across patients, patient organisation representatives, nurses and rheumatologists with respect to their perceptions of peer mentorship: experience with peer mentoring, the need in clinical practice, the added value and concerns (figure 1).

Perceptions on peer-mentorship by stakeholders.
Experience with peer mentoring
Previous experiences with peer mentoring were limited for all stakeholders, and many participants expressed only vague conceptual knowledge. Patient organisation representatives mentioned the initiatives they had already organised to stimulate peer contact. Nurses referred to informal contact between patients in the waiting room as a form of peer mentoring.
It’s a strange phenomenon. You know, where I realise it, it’s [happening] in the waiting room [at the consultation]. A lot! (Nurse, N3)
In general, the conceptualisation of peer mentoring by health professionals was rather narrow, as they described it foremost as an informal contact between patients talking to each other, without more details on the potential content/value of these contacts.
The need for peer mentoring as part of daily care practice in early RA
Differences between stakeholders
Most patients expressed an interest in peer mentoring and felt that having contact with a peer, who could give information and advice based on experience with the same disease, rather than with healthcare professionals, could help meet their social support needs.
Well, I think it gets more tangible when you talk to people who are in the same or a similar situation. Then it all becomes just that little bit easier. (Patient with early RA, P5)
Because that professor can know everything perfectly, it is the same as a dietician telling you to lose weight but does not really know what it means (Patient with early RA, P3)
Patient organisation representatives expressed that patients might feel reluctant to discuss certain topics with a rheumatologist, and that peer mentoring could help bridge this gap.
By contrast, both rheumatologists and rheumatology nurses questioned the need for peer mentoring because their patients did not usually mention or request it. In addition, rheumatologists considered referral to a rheumatology nurse or patient organisations to be sufficient to meet patients’ needs.
Rheumatology nurses also questioned the need for a peer mentoring programme based on their negative experiences with a broad range of self-management initiatives in the past.
Especially if it is a starting RA and there are apps that say ‘you must do this and work and this and that’, that they are like ‘oh my god, I'm going to do this and that’[…]‘oh dear, is this going to happen to me?[…] am I going to be able to do that? (Nurses, N2)
However, rheumatologists and nurses did identify the experience of not being alone in suffering from such a disease as a potential advantage of peer mentoring. Finally, they would not propose peer mentoring to all patients.
I do not understand the added value, how is the concept different then a patient organisation. Do I Miss.? you can refer to them too. They meet their peers there too. (Rheumatologist, R3)
Person-specific and disease-phase-specific need
All stakeholders expressed that the potential need for peer mentoring would depend on the individual and on the stage or course of the disease. Patients and patient organisation representatives stressed that transitioning from medication-free to medication-dependent, dealing with one’s social circle and grasping the content and impact of the disease are often overwhelming in the initial phase of RA. Therefore, they assumed peer mentoring could provide more disease context to patients struggling with these challenges.
You have to get back on your feet every time and some people can't do it on their own. I think that at any stage or at any time someone may need a peer. (Patient organisation representative PO4)
To identify these patients, nurses indicated that healthcare professionals should consider whether a patient would benefit from peer mentoring to receive extra advice.
By contrast, rheumatologists believed peer mentoring might be a good option to consider when patients express a need for peer support but admitted having received almost no requests for it.
The added value of peer mentoring in early RA
An extra dimension
Patients and patient organisation representatives felt that peers could make the context of the disease more tangible. They perceived the available time with a rheumatologist as often limited and the information provided as ‘academic’ and assumed a peer mentor could help digest this information while guiding and reassuring the patient through their experience.
It is very academic, I feel. The doctor approaches and explains the drugs but some aspects are less mentioned. Physiotherapy is non-existent here. I did not need it, but it was a question of mine. Don’t I have to do it? (Patient with early RA, P5)
Nurses mentioned that, unlike patients, they cannot know what it is like to actually suffer from the disease, although rheumatologists did not perceive this as a reason to implement peer mentoring. Some rheumatologists did question the added value of a peer mentor compared with patient organisations and nurses, and even perceived the provided help as inferior to those alternatives.
What is the added value if you have someone like a nurse who is trained, who knows what she is talking about, who can remain objective. (Rheumatologists, R4)
Feeling understood and recognised
Patients felt that a peer mentor would better allow them to share their feelings, get confirmation as to whether what they experienced was ‘normal’, as well as advice about dealing with the disease in everyday life. Patient organisation representatives confirmed that peers, in their opinion, often provide a sense of recognition and reassurance.
I see this happening in every training course for people in one way or another. And then the very nice thing is when you sit at the table together, half a word is enough, and everyone knows what this one’s talking about. (Patient organisation representative, PO1)
Additionally, emphasised in the focus groups with patients and patient organisation representatives was a perceived lack of recognition by the social environment of patients with RA. These stakeholders felt that a peer mentor could assist in the search for recognition in the patient’s social circle.
I was not able to open that door of the car, …, but no one could understand that I couldn't. (Patient with recent onset RA, P3)
Nurses also put forward the patient’s wish to be understood as an unmet need that could be addressed by peer mentoring, and this was regarded by some to be the only possible added value compared with the contribution of nurses.
I think the most important thing, I'm going to say to patients now, is that they'll be able to share their experiences with each other because people around them don't understand… and that is actually, in my opinion, the greatest added value. (Nurses, N3)
Rheumatologists did not mention this aspect.
Concerns towards peer mentoring in early RA
Some stakeholders expressed doubts towards peer involvement in patient care. For instance, patients mentioned that information from a peer mentor should not be accepted uncritically by the ones seeking help.
It’s not that a mentor owns all the wisdom, but those things that can work for you, you've got to pull it out…The requesting party just has to be very active… he [the peer mentor] is going to take care of you from now on. That’s not how it’s going to work. (Patients with early RA, P5)
One concern mentioned by nurses and rheumatologists was a potential loss of objective information transmission by the peer mentor in his contact with the patient. By contrast, patient organisation representatives expected this to be mitigated by the mentor’s professionalism and the accuracy of the information they could provide.
From person to person, from situation to situation, from disease to disease. There is too much to compare and it is all different. And that’s why I’m not fully behind it. (Nurses, N3)
You don't fall into small talk and into… complaining and nagging, coffee chatter. (Patient organisation representative, PO1/2)
Nurses, and particularly rheumatologists, feared a peer mentoring programme would not allow them to sufficiently control the information provided to the patient and the professionalism of the mentor. This way, they were concerned that some peer mentors would provide incorrect information to patients. However, both rheumatologists and nurses expressed that they would be less concerned if peer mentors had proper supervision and training.
So that [incorrect information] scares me a little right now. Now, if they are well-framed, if they are well-trained and very strictly defined, then I have no problem with that. (Rheumatologists, R4)
In general, all stakeholders agreed that peer mentors could have a certain natural authority and could potentially provide a powerful source of information, both in a positive and negative sense. Therefore, nurses and patient organisation representatives saw advantages for peer mentoring concerning medication-use and therapy compliance.
But suppose you have a patient who is not motivated to take his pills, perhaps a peer mentor would be able to do so. (Nurses, N1)
Format of peer mentorship
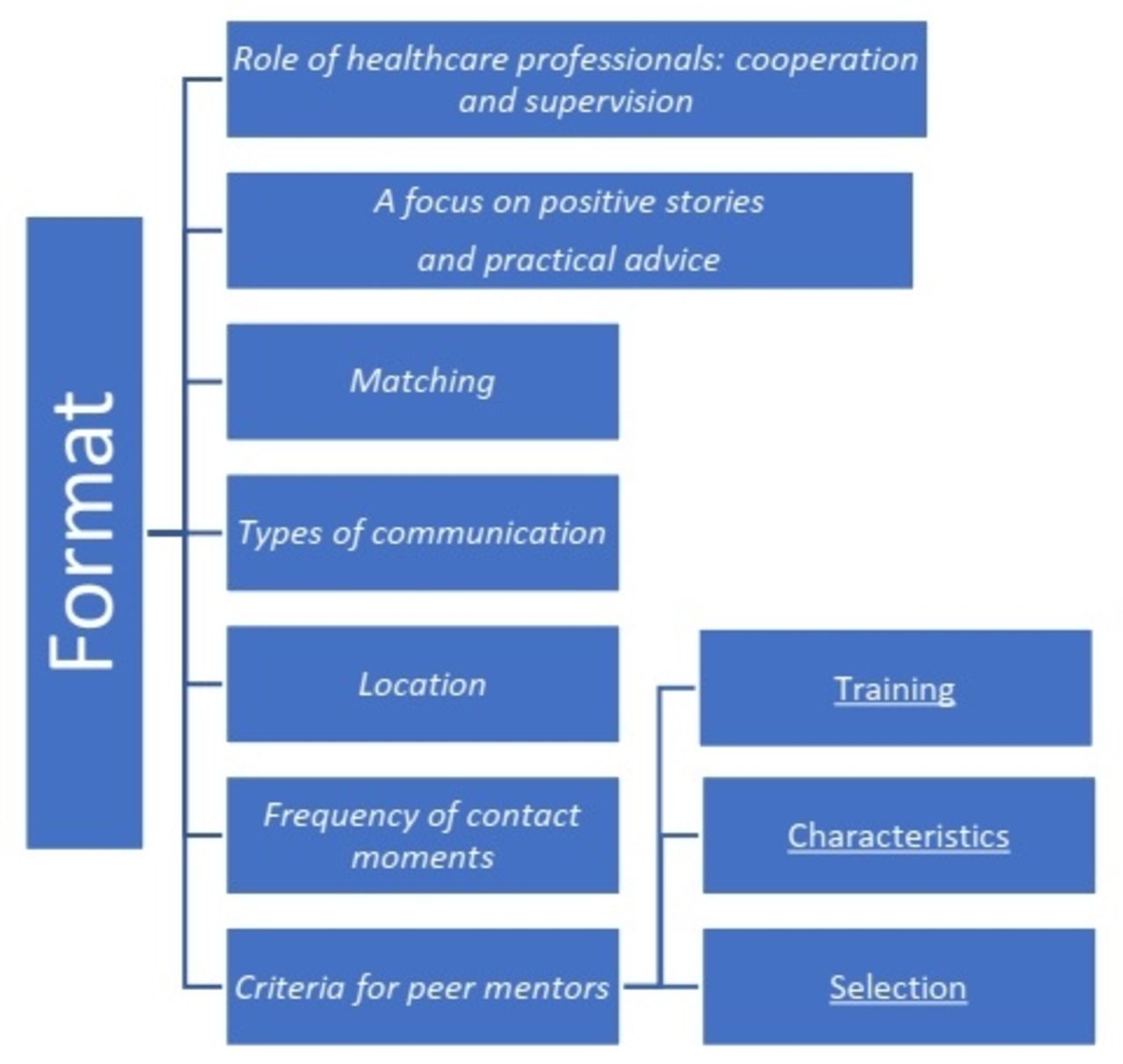
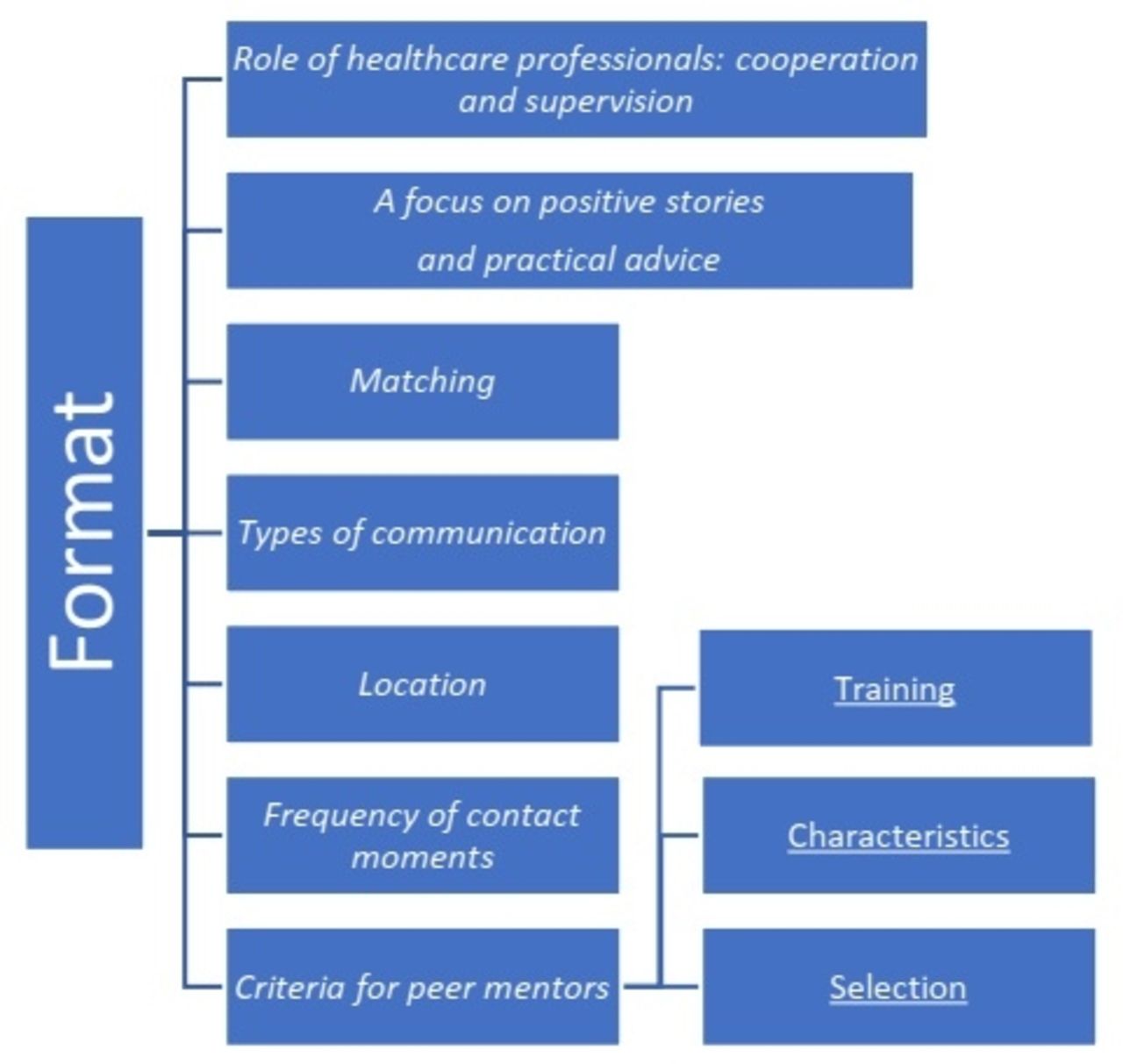
Opinions about the format and implementation of a peer mentoring programme varied among and within groups. Notably, the concept was more tangible for patients and patient organisation representatives than for healthcare providers. Figure 2 shows the themes important for stakeholders concerning the format of peer mentorship.
{kind=link}
{kind=link}
What can make a peer mentorship format successful?
Role of healthcare professionals: cooperation and supervision
Nurses and patients mentioned that the integration of peer mentoring in a multidisciplinary approach could provide a filter for correct and objective information transmission.
Yes, of course, because everyone can tell the biggest nonsense. If I, with a wrong conviction, talk about faith healers, naturopaths to patients, yeah, that doesn’t help anybody. And that’s what you want to avoid. So, if you have a kind of partnership, so to speak, with the professionals, then you don't completely rule out that risk, but the danger is reduced. (Patient with early RA, P5)
To provide this supervision, rheumatologists mentioned that it was important to personally know the peer mentor to reduce concerns of a subjective story. Another consideration made by rheumatologists was the current lack of integration of peer mentoring within the healthcare team.
Well, now I’m working with professional people. The nurses, the GP’s and the patients call me. That’s a closed system, we all have a shared responsibility, and we’re all covered by medical secrecy. But I’m not sure in what context we’re going to place those patient mentors, how much of a medical record of the other patient they can access. … So, I think that’s a delicate situation. (Rheumatologists, R1)
Generally, stakeholders’ motivation to be further involved in the development of a peer mentoring programme was quite varied. However, all stakeholders stressed the importance of cooperating in a multiprofessional team, including the rheumatologist, the nurse and the physiotherapist. Patient organisation representatives saw a role for themselves within a peer mentoring programme by assisting with the training and coaching of peer mentors. Healthcare professionals also mentioned their role in referring patients to a mentor.
Matching
Patients indicated that they would prefer peer mentors to be like them in terms of disease course, personal characteristics, stage of life and/or interests, to help answer questions about future perspectives. For instance, patients suggested a system of initial meetings with a group of peer mentors, before appealing to an individual mentor of their choice.
So, I shouldn’t ask a 90-year-old woman how she does it…I have to try to find someone who has a story similar to mine. (Patient with early RA, P5)
Nurses described this system as matching the profile between patient and peer mentor. Similarly, one rheumatologist briefly mentioned age as a characteristic to match these profiles.
A focus on positive stories and practical advice
The need for a standardised set of discussion themes for peer mentoring was cited by rheumatologists, nurses and patient organisation representatives. In general, all stakeholders mentioned that messages with a positive connotation should be emphasised to help provide reassurance to patients.
I’m beginning to understand this now. I think that reassurance is an important word in what is going to happen. And indeed, hearing about the experiences, what people are doing, what is helping them, is positive. I would only like to hear positive stories. (Patient with early RA, P1)
In addition, patients preferred a focus on practical issues that would help them to actively deal with their condition, including nutrition, fatigue, physiotherapy and practical tools. Similarly, patient organisation representatives discussed topics like fatigue, pain, activities, energy balance and employment. Caregivers also mentioned practical and everyday topics, such as role-fulfilment within the family. Finally, a theme underlined as a priority for all stakeholders was the discussion of future perspectives with peer mentors, to address the fears and uncertainties that often exist in the early disease stages.
I think the most important message should be ‘There is indeed still life after your diagnosis.’ (Rheumatologists, R5)
Notably, education on medication-use was expressed as a current unmet need by both patients and patient organisation representatives. However, this was perceived as a principal responsibility of care providers, rather than that of a peer mentor.
Location
No consensus was found across the focus groups concerning the ideal location for peer-mentoring activities. The location itself was generally perceived as irrelevant and above all needed to be practical. However, patients and patient organisation representatives did mention the hospital setting as a barrier for patients and tended to prefer a neutral location.
It’s not about the surroundings, it’s about the person you’re talking to. (Patients with early RA, P5)
Types of communication
Opinions on the form of communication in peer mentoring varied among focus groups. Patients and nurses suggested a combination of one-on-one contact and group contact, either online via a forum or face to face by means of group sessions, or even via email or by phone in case of very specific questions. Peer mentoring in group form was perceived as pragmatic by patients, because it would provide a range of experiences. Afterwards, a one-on-one match between patient and peer mentor could be useful. Additionally, it was emphasised by patients that a care provider should be ideally present as a moderator if the peer mentoring takes place in a group. Patient representatives preferred one-on-one contacts in person or by modern technologies. Rheumatologists once more expressed their concerns with one-on-one peer-mentorship contacts in case the peer mentor would stress their subjective opinion. Finally, all stakeholders agreed the ideal form of communication would be person dependent.
You have some that go to the computer, but you have some that go to the phone for contact, you have some that go to group meetings… Only in this way can you reach as many people as possible. (Patient organisation representative, PO5)
Frequency of contact moments
Only limited data were provided about the ideal frequency of peer-mentoring contacts. However, rheumatologists deemed repeated contact important to establish a relationship of trust.
Such a one-off conversation, I don't know if that will really pay off. I think that there is also a kind of relationship to be built up, as with the rheumatology nurse or doctor. A relationship of trust with someone you’ve never seen before [is impossible] … (Rheumatologist, R7)
Moreover, although the idea to involve partners or relatives, as proposed in the interview guide, was expected to have value in some cases, it was agreed by all stakeholders not to be a standard part of a peer-mentoring programme.
Criteria for peer mentors
Training
All stakeholders stressed the importance of adequate training for peer mentors. For instance, patient representatives suggested a ‘coaching’ course to provide specific communication and guidance skills to mentors, and similar suggestions were made by patients and rheumatologists.
Moreover, rheumatologists recommended to train mentors in conflict-avoidance strategies and in the recognition of ‘red flags’ to timely refer patients when needed.
They [Peer mentors] can also be trained for red flags. If there is a problem somewhere they say yes, you have to go further with that…(Rheumatologist, R5)
Selection
All stakeholders emphasised the need to carefully select adequate peer mentors and would prefer to retain certain restrictions on who would be allowed to take up this role. Rheumatologists particularly indicated to require a sufficient degree of confidence in the peer mentor.
Characteristics of an ideal peer mentor
All stakeholders had similar views on the characteristics an ideal peer mentor should exhibit. The peer mentor should possess communication skills, disease insight and knowledge, be able to function with the disease, and remain professional. However, what it means to be able to function with the disease was perceived differently between stakeholder groups. For instance, rheumatologists would choose mentors with either limited disease or a more severe RA that eventually had a positive outcome, while patient representatives considered adequate physical functioning, defined as not going through a disease flare, as a criterion.
Discussion
This qualitative study is, to our knowledge, the first to bring together the vision of rheumatologists, nurses, patient organisations and patients with early RA about incorporating peer mentoring in an integrative management of patients with early RA. We also investigated the practical and substantive requirements for an effective and meaningful peer-mentoring programme. The analysis of the different focus groups revealed many similarities, but also differences in perceptions among stakeholders. Since successfully implementing peer mentoring programmes remains a complex intervention, these insights might provide essential guidance to support the implementation process.
All stakeholders agreed that peer mentoring should be an option and should not be mandatory in managing patients with early RA, as the need for peer-mentorship is patient-specific, as well as dependent on the patient’s stage of life and disease. This opinion echoes results of studies on the use of specific validated instruments like the ENAT to explore the individual needs of patients with arthritis.4 However, while such instruments do assess the need for support systems, self-help measures and health professional treatments, among others, they unfortunately do not explore the wish for peer-to-peer interventions.
The stakeholders in this study had no unambiguous picture about the precise details of a peer-mentoring programme. However, of critical importance were the peer mentors themselves. Pivotal peer-mentor characteristics were thought to include communicative skills, insight and knowledge about the disease, objectivity or professionalism and having a good physical functionality. Since it was assumed that an individual mentor could influence the patient both positively and negatively with regards to the outcome of their intervention, nurses and particularly rheumatologists underlined their fear for loss of focus by the mentor. Specifically, they strongly felt the need to be able to trust the peer mentor as a partner in patient management. Therefore, most stakeholders, with the exception of some patients, agreed that not everyone should be able to assume a peer-mentoring role. Consequently, it is not surprising that training peer mentors in several key domains was deemed mandatory by most stakeholders. In diabetes, such training with an aim to increase knowledge, empowerment-based facilitation, active listening and self-efficacy, has already shown to be feasible and successful, with 75% of aspiring peer mentors meeting the requirements to lead diabetes self-management support interventions at the first attempt.19
Within our study, different sensitivities were uncovered in the respective stakeholder groups. First, the role of a peer mentor partially overlaps with specialist nurses in rheumatology, necessitating a clear task allocation to mitigate this sensitivity. Second, a legal framework for the role of a peer mentor does not exist In Belgium, nor in many other countries. This seems crucial however, as the peer mentor should also be protected in the performance of their duties. Third, financing of a peer mentor is currently not regulated. However, positive experience has been gathered in Belgium for over 20 years in the context of the Patient Partner Programme. This programme consists of trained patients with RA, who successfully educate medical students, physicians, and other health professionals. Recently the Patient Partners adapted their programme to incorporate specific patient perceptions into the subject matter provided.29 This organisation might serve as an example to train and engage peers to participate in the management of rheumatic diseases. For the education of medical students and health professionals much effort is being put in the standardisation of the programme. Patient partners are also trained to deal with ‘difficult’ personalities during the sessions they provide. However, an additional challenge of peer mentoring will be to train the mentors to address patients as much as possible at their individual educational level, while ensuring the message of the peer mentoring programme remains consistent for all patients.
Our study has some limitations. First, only one focus group per type of stakeholder was conducted, except for two patient groups. Furthermore, focus groups were held with distinct stakeholder groups, meaning that interaction between different stakeholder groups was not possible. However, efforts have been made to make the groups as heterogeneous as possible, including individuals from three different patient organisations and rheumatologists from private centres, non-academic and academic hospitals. Second, although we aimed to include all important stakeholders for a peer-mentoring programme, it could be noted that the perceptions of general practitioners, patient’s relatives and healthcare professionals other than nurses would have been of additional interest. Third, our results are specifically related to the Belgian situation. However, since experience with peer-mentoring programmes in rheumatology practice is rather limited in many countries, healthcare professionals, patient organisations and researchers from different healthcare settings could use the findings from our study relevant to their particular objectives.
A strength of our study is the application of a rigorous method of qualitative analysis, guided by the QUAGOL as a framework and applied by an interdisciplinary research team. As a result, this team was involved in a structured way in analysing the results, but also in testing the interview guide and concepts after each interview. Additionally, the involvement of patient researchers at multiple stages in this study is an important strength. Their personal experience in living with RA was a valuable addition to the scientific perspective of the researchers.
The rich results of our study can now be used as a basis for pilot projects aiming to train peer mentors and involve them in the care for specific patients. Our results show that specific needs for peer mentoring in the treatment of early RA should be individually tailored, and our findings could also be of use to avoid certain pitfalls in implementing such a complex intervention.
Conclusion
The concept of peer mentoring and how to implement this in practice remains vague, particularly for healthcare providers. Patients and patient organisation representatives did feel that peer mentoring has potential to provide newly diagnosed patients with RA with support and pragmatic information on how to cope with their disease early on. However, nurses and particularly rheumatologists saw less immediate benefits in a peer-mentoring programme. They felt particularly concerned about the information the peer mentor would provide, since they assumed that they would have limited control over it. Appropriate education, selection, coaching and supervision of peer mentors was considered essential as well as matching them to specific patients and integrating them in the multidisciplinary care team. Under these conditions, a peer-mentoring programme could constitute a currently missed opportunity to improve the lives of patients with recently diagnosed RA.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. The data source is available on reasonable request to the authors.
Ethics statements
Patient consent for publication
Ethics approval
The Ethical Committee of the KU Leuven approved this study. Participants had to indicate to have read and accept an information letter before starting this anonymous survey.
Acknowledgments
We would like to thank all participants of this study.
References
Footnotes
KVdE and DDC are joint first authors.
Twitter @DiederikDeCock
Contributors KVdE, DDC, RW and PV designed the study, LB, LP, KVdE and DDC acquired the study data. DDC drafted the final manuscript. All authors helped in the analyses of the study and approved the last draft of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.