Article Text

Abstract
Aim To explore the effects of exercise (water-based or land-based) and/or manual therapies on pain in adults with clinically and/or radiographically diagnosed hip osteoarthritis (OA).
Methods A systematic review and meta-analysis was performed, with patient reported pain assessed using a visual analogue scale (VAS) or the Western Ontario and McMaster Universities Arthritis Index (WOMAC) pain subscale. Data were grouped by follow-up time (0–3 months=short term; 4–12 months=medium term and; >12 months=long term), and standardised mean differences (SMD) with 95% CIs were used to establish intervention effect sizes. Study quality was assessed using modified PEDro scores.
Results 19 trials were included. Four studies showed short-term benefits favouring water-based exercise over minimal control using the WOMAC pain subscale (SMD −0.53, 95% CI −0.96 to −0.10). Six studies supported a short-term benefit of land-based exercise compared to minimal control on VAS assessed pain (SMD −0.49, 95% CI −0.70 to −0.29). There were no medium (SMD −0.23, 95% CI −0.48 to 0.03) or long (SMD −0.22, 95% CI −0.51 to 0.06) term benefits of exercise therapy, or benefit of combining exercise therapy with manual therapy (SMD −0.38, 95% CI −0.88 to 0.13) when compared to minimal control.
Conclusions Best available evidence indicates that exercise therapy (whether land-based or water-based) is more effective than minimal control in managing pain associated with hip OA in the short term. Larger high-quality RCTs are needed to establish the effectiveness of exercise and manual therapies in the medium and long term.
- Osteoarthritis
- Hip
- Physiotherapy
Statistics from Altmetric.com
Introduction
Hip osteoarthritis (OA) is characterised by structural and functional failure of the femoroacetabular joint. Radiologically, hip OA is evident by joint space narrowing, bony sclerosis, osteophyte formation and deformity of the femoral head and acetabulum.1 Clinically, hip OA results in pain, globally reduced hip range of motion, altered gait, decreased lower limb proprioception and balance and weakness of the surrounding musculature.2 These physical impairments contribute to reduced productivity through increased rates of absenteeism, poor physical function and fatigue secondary to sleep disturbance.3
International guidelines recommend that non-pharmacological treatments be included as a first-line strategy for the initial management of hip OA.4 In particular, exercise and manual therapies are frequently introduced to manage the pain associated with hip OA.5 ,6 Previous systematic reviews have synthesised available evidence to explore the efficacy of manual7 ,8 and exercise8 ,9 therapies in reducing pain in populations with hip OA. However, these reviews were hampered by a limited number of hip OA specific randomised clinical trials (RCTs) available for analysis at the time. Since a number of RCTs investigating the effects of manual and exercise therapies for hip OA have been recently published, it is timely to conduct an updated high-quality systematic review. The aim of this systematic review was to examine the short-term, medium-term and long-term efficacy of land-based and water-based exercise therapies and manual therapies in the reduction of pain in patients with hip OA.
Method
Identification and selection of studies
The systematic review protocol was developed and executed according to the guidelines supplied by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) statement.10 The following databases were searched: MEDLINE, EMBASE, CINAHL, PEDro, SCOPUS and the full Cochrane Library. Search terms included those related to the hip, arthritis, rehabilitation and randomised controlled trial. The full details of the search strategy used for MEDLINE, and adapted for all other databases, are included in online supplement 1. Publications from the earliest record until July 2014 were considered for inclusion. The database searches were conducted independently by two investigators (LB and KMC), who also retrieved article abstracts. A grey literature search was also conducted of: Google Search Engine; Clinical Trial registers in the USA, UK, Australia and the Netherlands; and online-first journals. Reference lists of published systematic reviews were searched to confirm the retrieval of appropriate studies.
Title and abstracts were screened for eligibility by at least two investigators (from JW, PF, SJW and KMC), with full texts obtained if necessary. Any discrepancies were resolved during a consensus meeting with a third reviewer. The criteria for inclusion of studies are presented in box 1. Studies may have compared exercise therapy and/or manual therapy with a control intervention, or compared between manual therapy and exercise therapy, or compared different types of manual therapies or exercise therapies. Studies were excluded if they only investigated postarthroplasty care or presented combined hip and knee OA data where data for the hip OA group could not be extracted or obtained. Studies were also excluded if they: (1) presented results that duplicated those reported previously; (2) did not report pain on one of the outcome measures presented in box 1, or; (3) had a high risk of bias (see next section).
Inclusion criteria
Design
Randomised trial
Published in English
Participants
Adults with clinically and/or radiographically diagnosed hip OA
Intervention
Exercise (water-based or land-based) and/or manual therapies
Outcome measures
Patient-reported pain scores on a visual analogue scale (VAS), numerical rating scale (NRS) or the Western Ontario and McMaster Universities Arthritis Index (WOMAC) pain subscale
Assessment of characteristics of studies
A modified PEDro rating scale with 15 criteria was used to rate the methodological quality of included studies (see online supplement 2). The modified scale has previously been used with high inter-rater reliability in systematic reviews.11 ,12 Two investigators (from JW, JLK and PF) independently evaluated included studies on the 15 criteria, with any discrepancies resolved by a third independent reviewer (KMC). Once consensus was reached, a final rating out of 14 was calculated by summing the criteria with a positive score. The maximum score was 14 as criterion 1 (specification of eligibility criteria) was not counted as it influences trial external validity, but not internal or statistical validity.
The six PEDro rating criteria that satisfy the requirements of the PRISMA statement13 were used to determine the risk of bias. These criteria were: (1) adequacy of randomisation (criterion 4); (2) allocation concealment (criterion 5); (3) between-group baseline comparability (criterion 6); (4) blinding of outcome assessors (criterion 9); (5) adequate follow-up (>85%) (criterion 11) and; (6) intention-to-treat analysis (criterion 12). The criterion related to lack of participant or therapist blinding were not considered to be a high source of bias due to the difficulties inherent in blinding for physical interventions such as exercise therapy and manual therapy. Studies scoring positively on ≥5 of the 6 criteria were classified as having a low risk of bias, while those scoring 3–4 were classified as having a moderate risk. Studies scoring ≤2 were considered to have a high risk of bias and were excluded from the review.
Data analysis
Inter-rater reliability of modified PEDro ratings for both overall agreement and each criterion was evaluated by calculating percent of initial agreement and kappa (κ) coefficients. Patient reported pain scores were converted to a 100-point scale. Convention for the WOMAC is to assign 0 points to the worst score and 100 points to a perfect score. The scale was reversed in this review to provide directional consistency with VAS and NRS data. Data were grouped by follow-up time (≤3 months or 13 weeks=short term, 4–12 months=medium term and >12 months=long term), with some studies providing data at multiple follow-up times. Data at the latest time point was used for studies reporting multiple follow-up times within an individual time point window.
Review Manager (RevMan) 5.314 was used to compute standardised mean differences (SMD), and their 95% CIs, to indicate intervention effect sizes on pain. The SMD was calculated using follow-up scores and SDs if baseline data was comparable. Email was used to contact authors for additional data, or means and SDs were obtained from published meta-analyses, when not provided in the original publication. Effect sizes were considered to be being nearly perfect (SMD <−4), very large (−4 to −2), large (−2 to −1.2), moderate (−1.2 to −0.6), small (−0.6 to −0.2) and trivial (−0.2 to 0),15 with negative values favouring the intervention of interest. Significance was set at p<0.05. Study data were pooled using a random effects model when interventions and comparative groups were deemed similar and used the same patient-reported outcome measure (VAS or WOMAC) and follow-up time (short, medium or long term). Heterogeneity was confirmed by calculating χ2 (>0.05) and I2 (<50%) scores. To determine if studies investigating exercise therapy prior to total hip arthroplasty affected the pooled results, a sensitivity analysis was performed excluding presurgical studies.
Results
Flow of studies through the review
The search identified 7016 papers of which 68 were retrieved in full-text (figure 1). Forty-five full-text papers were excluded based on the exclusion criteria, with six of these excluded because data from individuals with hip OA could not be separated from those with knee OA (see online supplement 3 for the excluded papers). Twenty-three papers were rated on the PEDro scale for risk of bias, with four excluded due to a high risk of bias (see online supplement 4 for ratings for PEDro scores for the papers with high risk of bias). No papers were excluded for not reporting pain on the VAS, NRS or WOMAC pain subscale. Inter-rater agreement on overall modified PEDro score was very high (κ=0.90; 95% agreement) and inter-rater reliability for individual items ranged from very high agreement (κ=0.74) for criterion 9 to perfect agreement (κ=1.00) for criteria 1 and 4. Consensus was reached on all criteria after initial discussion.

Flow of studies through the review.
Characteristics of included studies
The overall modified PEDro score and characteristics of the 19 included studies are shown in online supplements 5 and 6. Thirteen studies compared exercise therapy +/− education to a minimal control,13 ,16–27 four compared different types of exercise therapy,16 ,18 ,28 ,29 three compared manual therapy and exercise therapy to exercise therapy alone,20 ,22 ,30 four compared manual and exercise therapy to a minimal control,20 ,22 ,30 ,31 two compared manual therapy to exercise therapy,20 ,32 and one compared different types of manual therapy.33 The mean age of participants in included studies ranged from 52 to 77 years, mean body mass index ranged from 21.7 to 33.8 kg/m2, and hip OA mean symptom duration ranged from 24 months to 102 months.
Effect of exercise therapy on pain in patients with hip OA
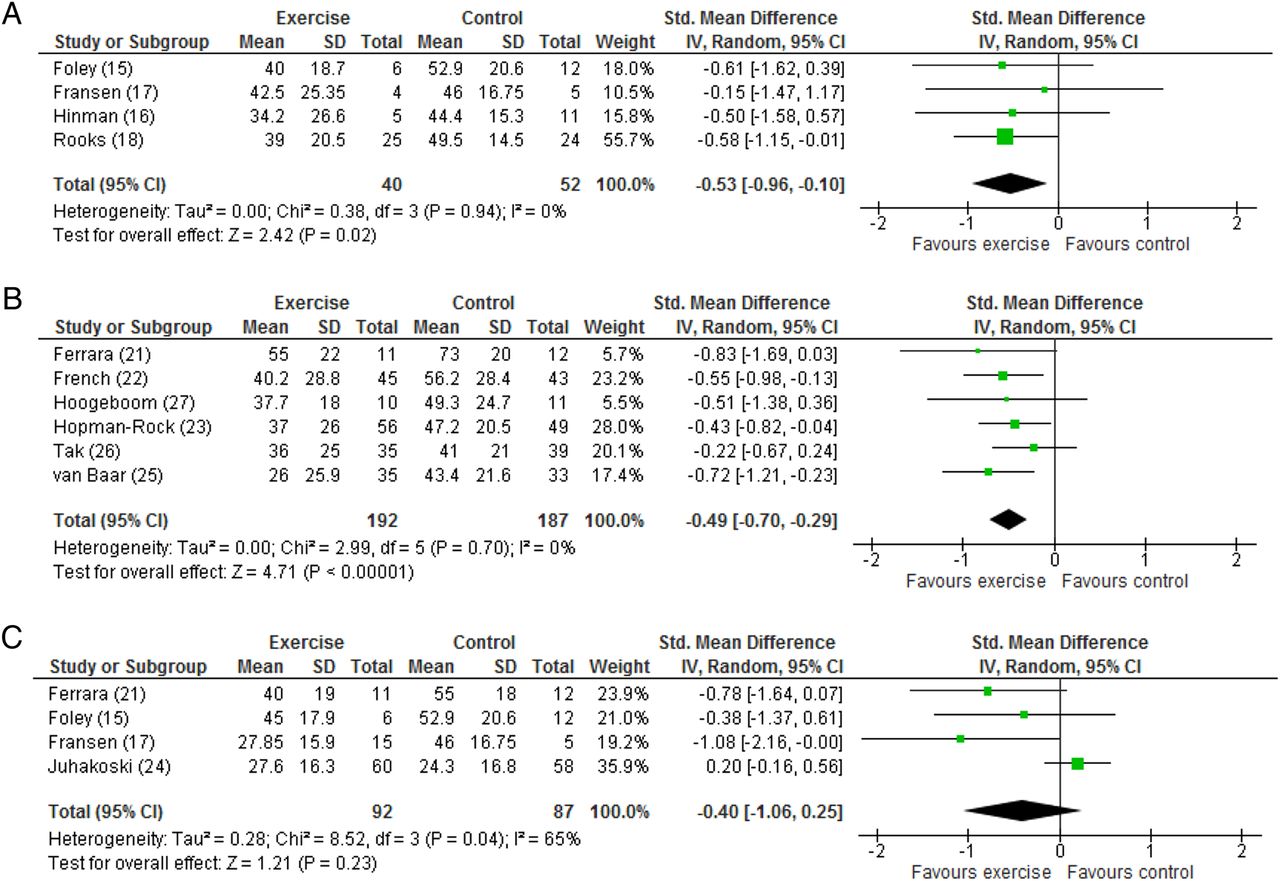
There was mixed evidence from the different time points regarding the role of exercise therapy compared to minimal control in the management of hip OA pain (see online supplement 5). At the short-term time point (≤3 months or 13 weeks), Hinman et al17 reported no significant benefit for water-based exercise compared to control when using the VAS to assess pain (SMD −0.13, 95% CI −1.18 to 0.93). In contrast, pooled data from four studies16–19 involving 92 participants showed significant benefits favouring water-based exercise over minimal control when pain outcomes were assessed using the WOMAC pain subscale (SMD −0.53, 95% CI −0.96 to −0.10; I2=0%, χ2=0.38; p=0.94; figure 2A). No studies examined the medium-term or long-term benefits of water-based exercise.

Forest plots of the short-term (<3 months or 13 weeks) effects of exercise therapy on pain associated with hip OA. (A) Effect of water-based exercise compared to minimal control when pain outcomes were assessed using the WOMAC pain subscale. (B) Effect of land-based exercise compared to minimal control when pain outcomes were assessed using the VAS. (C) Effect of land-based exercise compared to minimal control when pain outcomes were assessed using the WOMAC pain subscale. Data are presented as standardised mean difference, with differences <0 favouring exercise therapy. OA, osteoarthritis; VAS, visual analogue scale; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
Pooling data from six studies21–23 ,25–27 involving 379 participants demonstrated a benefit of land-based exercise compared to minimal control in the short-term (≤3 months or 13 weeks) when pain outcomes were assessed using the VAS (SMD −0.49, 95% CI −0.70 to −0.29; I2=0%, χ2=2.99; p=0.70; figure 2B). The additional study using the VAS that could not be pooled did not support an exercise therapy benefit.24 Since two studies in the pooled analysis included participants who were on waiting lists for total hip arthroplasty,21 ,27 a sensitivity analysis was conducted to determine their impact. The pooled data from the four remaining studies22 ,23 ,25 ,26 supported a similar positive benefit of land-based exercise (SMD −0.47, 95% CI −0.69 to −0.25; I2=0%, χ2=2.37; p=0.50). Four studies16 ,18 ,21 ,24 involving 179 participants showed no benefit of land-based exercise compared to minimal control in the short term when pain outcomes were assessed using the WOMAC pain subscale (SMD −0.40, 95% CI −1.06 to 0.25; I2=65%, χ2=8.52; p=0.04; figure 2C).
At the medium-term time point (4–12 months), pooled data from three studies13 ,20 ,22 involving 237 participants revealed no significant benefit for exercise therapy compared with control when pain outcomes were assessed using the WOMAC pain subscale (SMD −0.23, 95% CI −0.48 to 0.03; I2=0%, χ2=0.85; p=0.65; figure 3A). Similarly, pooled data from two studies13 ,24 involving 191 participants and long-term follow-ups (>12 months) reported no benefits of exercise when pain outcomes were assessed using the WOMAC pain subscale (SMD −0.22, 95% CI −0.51 to 0.06; I2=0%, χ2=0.21; p=0.65; figure 3B).
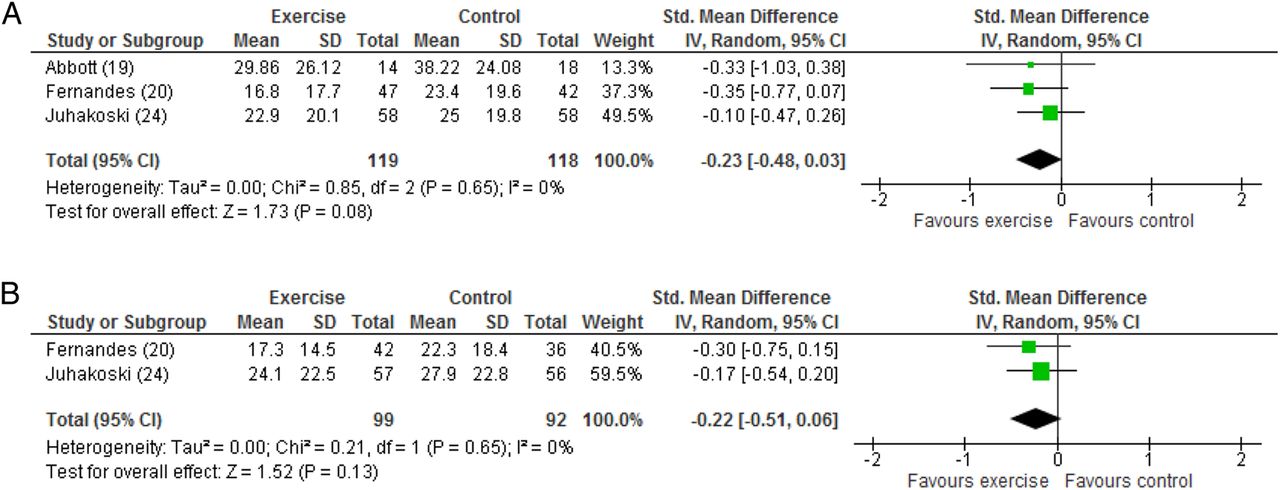
Forest plots of the: (A) medium-term (4–12 months) and (B) long-term (>12 months) effects of land-based exercise therapy compared to minimal control on pain associated with hip OA when pain outcomes were assessed using the WOMAC pain subscale. Data are presented as standardised mean difference, with differences <0 favouring exercise therapy. OA, WOMAC, Western Ontario and McMaster Universities Arthritis Index.
Four studies16 ,18 ,28 ,29 compared different types of exercise therapies (see online supplement 5). Pisters et al29 compared a 12-week behavioural graded activity approach focusing on individually tailored exercises aimed at a patients’ functional complaints to usual exercise therapy. They reported small and moderate effect sizes at 3 and 9 months in favour of behavioural graded activity when pain outcomes were assessed using the WOMAC pain subscale, respectively; however, benefits were not maintained at the long-term (5 year) follow-up. Fukumoto et al28 compared high and low velocity home-based resistance training finding no significant group difference in VAS-assessed pain after 8-weeks. Similarly, Foley et al16 and Fransen et al18 found no differences between water-based and land-based exercises when pain outcomes were assessed in the short term using the WOMAC pain subscale.
Effect of manual therapy with or without exercise on pain in patients with hip OA
Individual studies provided some evidence regarding the role of manual therapy in the management of hip OA pain (see online supplement 6). However, pooled evidence from three studies22 ,30 ,31 (248 participants) found no significant effect of combined manual and exercise therapy over minimal control in the short term (≤3 months or 13 weeks) when pain outcomes were assessed using the VAS (SMD −0.38, 95% CI −0.88 to 0.13; I2=74%, χ2=7.76; p=0.02; figure 4A). Similarly, pooled evidence from two studies30 ,31 reported no medium-term (4–12 months) benefit of combined manual and exercise therapy over minimal control when pain outcomes were assessed using the VAS (SMD −0.07, 95% CI −0.50 to 0.36; I2=42%, χ2=1.74; p=0.19; figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots of the: (A) short-term (≤3 months or 13 weeks) and (B) medium-term (4–12 months) effects of combined manual and exercise therapy over minimal control, and (C) short-term (≤3 months or 13 weeks) of combined manual and exercise therapy over exercise therapy alone when pain outcomes were assessed using the VAS. Data are presented as standardised mean difference, with differences <0 favouring exercise therapy. VAS, visual analogue scale.
Comparing manual therapy against exercise therapy revealed no benefits. Pooled data from two studies (158 participants) found no short-term effect of combined manual and exercise therapy compared to exercise therapy alone when pain outcomes were assessed using the VAS (SMD −0.48, 95% CI: −1.55 to 0.59; I2=91%, χ2=10.74; p=0.001; figure 4C).22 ,30 Likewise, individual data from two studies20 ,32 comparing manual therapy with exercise therapy reported no group differences. Only one study compared two types of manual therapy techniques, reporting no additional short-term benefit of chiropractic lower limb full kinetic chain (including lumbar spine and lower limb) manipulation compared with targeted hip manipulation.33
Discussion
Our systematic review identified 19 RCTs evaluating the efficacy of exercise and manual therapies on pain associated with hip OA. Meta-analyses indicate that both land-based and water-based exercise programmes were superior to a control intervention in the short term; however, no benefits of land-based exercise therapy were seen at a medium-term or long-term follow-up. There were no benefits of manual therapy when either combined with exercise or introduced in isolation.
Exercise therapy
Current clinical guidelines recommend exercise therapy in the management of hip OA.4 Exercise therapy, including group exercise, aquatic exercise and home exercise programmes, is commonly utilised by physiotherapists.5 ,6 For land-based exercise, our results are consistent with the recent Cochrane review of land-based exercise for hip OA by Fransen et al.9 Our finding of a similar effect for water-based exercise therapy suggest that exercise therapy may benefit people with hip OA in the short-term irrespective of delivery mode. The majority of exercise therapy interventions in our review included some form of education. Education is an essential component of physiotherapy management, and aims to promote a greater understanding of OA and promote self-management strategies for this degenerative disease. In the current review, the isolated effects of education were not evaluated and education may have contributed to some of the observed benefits of exercise.
Our pooled results for water-based exercise therapy revealed a small effect size for decreasing pain in patients with hip OA in the short term compared to minimal intervention control. Water-based exercise therapy enables buoyancy forces to reduce weight bearing in the lower limbs, thus unloading arthritic joints to provide pain relief. The warmth of the water may also provide pain relief by improving circulation and reducing muscle spasm. The best effects were observed by Rooks et al,19 where exercise programmes were performed three times a week. Treatment frequency may be an important factor when considering exercise for pain relief.
Pooled data for land-based exercise therapy revealed a small significant effect for decreasing pain in the short-term. Two of the pooled studies targeted preoperative improvements in pain,21 ,27 while four investigated a non-surgical group.22 ,23 ,25 ,26 The effect of exercise therapy on pain reduction was not limited by the inclusion of the preoperative studies, where less improvement may be expected, since removal of these studies did not appreciably change the pooled results. The exercise therapy elements of all studies were similar; incorporating hip stretches, strengthening exercises and balance tasks. The additional study that could not be pooled, did not support exercise therapy, which may reflect their use of group therapy rather than individualised treatment.24 In contrast, the RCTs with the best individual results were French et al22 and van Baar et al.25 French22 included a 30 min individually supervised session once a week for 8 weeks and a home programme, where patients were encouraged to do 30 min of aerobic exercise 5 days a week. These recommendations are in line with the Australian and WHO recommendations for exercise in older adults.34–36 van Baar et al25 showed a moderate effect using an individualised exercise programme including muscle strengthening and stretching exercises, ADL modification and a home programme performed one-to-three times a week.
The medium-term and long-term exercise therapy effects were less encouraging. Pooled data from three studies suggest a non-significant tendency (p=0.08) towards positive exercise therapy effects on pain in the medium-term, while long-term exercise therapy effects were not observed in two pooled studies (p=0.13). Adherence to exercise programmes in the medium-term and long-term usually decreases37 and this factor would influence the effectiveness of exercise beyond the short term. Additionally, OA is a progressive, degenerative disease that may naturally worsen over time regardless of intervention. While the best available evidence appears to favour exercise therapy for short-term pain relief, more RCTs are needed to confirm the effect size. Furthermore, the tendency towards a positive medium-term exercise effect could be confirmed with more studies incorporating a longer follow-up. It is also possible that exercise therapies with longer duration, top-up sessions or with adherence strategies may facilitate better effects.
Four studies compared different types of exercise therapies. The study by Pisters et al,29 suggests that a behavioural graded activity approach in an initial 12-week programme plus a series of booster sessions, is effective with small and moderate effect sizes at 3-month and 9-month follow-ups, respectively. The focus on education and behaviour modification, with ‘reminder’ sessions may have assisted long-term change and adherence to the exercise programme; however, the isolated effect of behavioural graded activity versus booster sessions was not explored and warrants further study. In contrast, Fukumoto et al,28 compared high velocity with low velocity training as part of a hip strengthening home exercise programme and found no significant difference in pain outcomes after 8 weeks. This suggests strengthening exercises are more important than speed of performance. The studies by Foley et al16 and Fransen et al18 found no differences between water-based and land-based exercises; however, a lack of statistical power due small sample sizes (≤6 subjects per comparative group) may have contributed to the absence of statistical findings. Ultimately, more studies are required to confirm any superior effects of one type of exercise therapy, or whether individual participant characteristics may predict better outcomes with different types of exercise therapy.
In summary, the best available evidence indicates that alternate forms of exercise therapy delivery, water-based or land-based, appear to result in positive, but small effects. More RCTs are needed to confirm these short-term effects. There is a clear need to evaluate longer term exercise therapy treatments, and those that include individualised exercise therapy and increasing physical activity.
Manual therapy
Physiotherapy is recommended for management of hip OA4 and manual therapy is a common component of contemporary physiotherapy.5 ,6 Our current review located five studies investigating manual therapy for hip OA and failed to identify a positive benefit of manual therapy (with or without exercise) when compared to either exercise therapy alone or a minimal control.
Our pooled data indicate that manual therapy when combined with exercise is not an effective intervention for pain from hip OA in the short term. However, there was considerable statistical (I2=74%) and methodological heterogeneity. Hence, more studies are required to have confidence in the pooled results. Manual therapy was not superior to exercise therapy in two studies.20 ,32 Similarly, combined manual and exercise therapy was not superior to exercise therapy alone from three studies.20 ,22 ,32 The only study to compare different manual therapy techniques found no additional benefit of applying chiropractic techniques to the lumbar spine and lower limb compared to treating the hip alone.33
The best available evidence for short-term effects on hip OA pain does not support manual therapy. However, more RCTs are needed to confirm these effects and there is a need to evaluate treatments that extend beyond 3 months.
Strengths and limitations
This study has a number of strengths. Our review investigated a large number of studies (n=19) from an extensive literature search and excluded studies with high risk of bias. We evaluated land-based and water-based exercise therapy separately, as well as manual therapy (although many of the studies did introduce multiple interventions in combination). Importantly, 10 out of the 19 included studies investigated interventions that were designed specifically for people with hip OA, and not a combined hip/knee OA treatment approach. This increases the clarity regarding the specificity of treatment for hip OA; however, there remains a need for additional studies of interventions targeted solely towards hip OA.
Despite the strengths of our study, there are some limitations that should be acknowledged. We did not explore exercise or manual therapy effects on function and only included RCTs in English language, which may have excluded potentially eligible studies with relevant findings. Also, it is recognised that we cannot account for publication bias where non-significant results were not published. The heterogeneity between study populations and interventions may also limit our results. Future studies must be high-quality RCTs fulfilling the criteria for low risk of bias. Also, the studies should include greater participant numbers. A number of studies in this review had <15 subjects per group, making it difficult to establish treatment effects.
Conclusion
In conclusion, this systematic review identified a number of RCTs that evaluated the efficacy of exercise and manual therapies on pain associated with hip OA. From the available data, there is evidence that exercise therapy (whether land-based or water-based) is more effective than minimal intervention control in the short term. No significant benefits of land-based exercise were observed at medium-term or long-term follow-up time points. Similarly, there were no significant benefits for manual therapy at any time point. Ultimately, larger, high-quality RCTs are needed to better elicit the effectiveness of exercise and manual therapies for hip OA.
What are the findings?
Pooled data demonstrated short term (0–3 months) benefits of water-based or land-based exercise over minimal control when assessed using the Western Ontario and McMaster Universities Arthritis Index pain subscale and visual analogue scale assessed pain, respectively.
There were no benefits of exercise therapy when assessed at either a medium-term (4–12 months) or long-term (>12 months) follow-ups.
There were no benefits of manual therapy when either combined with exercise or introduced in isolation.
How might it impact on clinical practice in the future?
Our search indicated a general lack of well-designed clinical trials exploring the benefits of exercise and/or manual therapies specifically targeting individuals with hip osteoarthritis (OA).
Despite the limited number of trials, clinicians can prescribe water-based and land-based exercises to individuals with hip OA with the expectation that short-term benefits should be obtained.
With the execution and publication of further clinical trials, clinicians will be provided with a firmer evidence base as to the short and long-term benefits of exercise and/or manual therapies in individuals with hip OA.
Acknowledgments
Dr Andrew Claus is thanked for his contribution in identifying potentially eligible studies from retrieved titles and abstracts.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
- Data supplement 3 - Online supplement
- Data supplement 4 - Online supplement
- Data supplement 5 - Online supplement
- Data supplement 6 - Online supplement
Footnotes
Twitter Follow Joanne Kemp at @JoanneLKemp
Contributors LB and KMC performed database searches. JW, PF, SJW and KMC screened articles for eligibility. JW, JLK, PF rated article characteristics. SJW and KMC carried out the statistical analyses and drafted the manuscript. All authors were involved in the analysis and interpretation of the data. All authors were involved in study conception and design. All authors provided critical revision of the manuscript, and read and approved the final manuscript. SJW and KMC are the guarantors, and had full access to all of the data and take responsibility for its integrity and accuracy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Warm up