Article Text

Statistics from Altmetric.com
Hepatitis C virus (HCV) infection is prevalent worldwide and is associated with cirrhosis and hepatocellular carcinoma. Although antitumour necrosis factor (anti-TNF) α agents may affect the competence of the immune system against viral infection,1 some studies have demonstrated that TNF-α inhibitors may be safe in patients with chronic HCV infection.2 ,3 A recent randomised clinical trial showed that rheumatoid arthritis (RA) patients with chronic HCV were treated successfully with etanercept without elevation of transaminases and HCV viral load.4 However, rituximab (RTX) is associated with increasing HCV RNA levels in lymphoma patients undergoing RTX combined with chemotherapy.5 ,6 RTX-related HCV reactivation was also observed in RA patients.7 Therefore, biological therapies of different mechanism of action may influence on HCV replication differently. To test this hypothesis, we conducted a retrospective safety profile review of RA patients with concomitant HCV infection treated with TNF-α inhibitors and RTX.
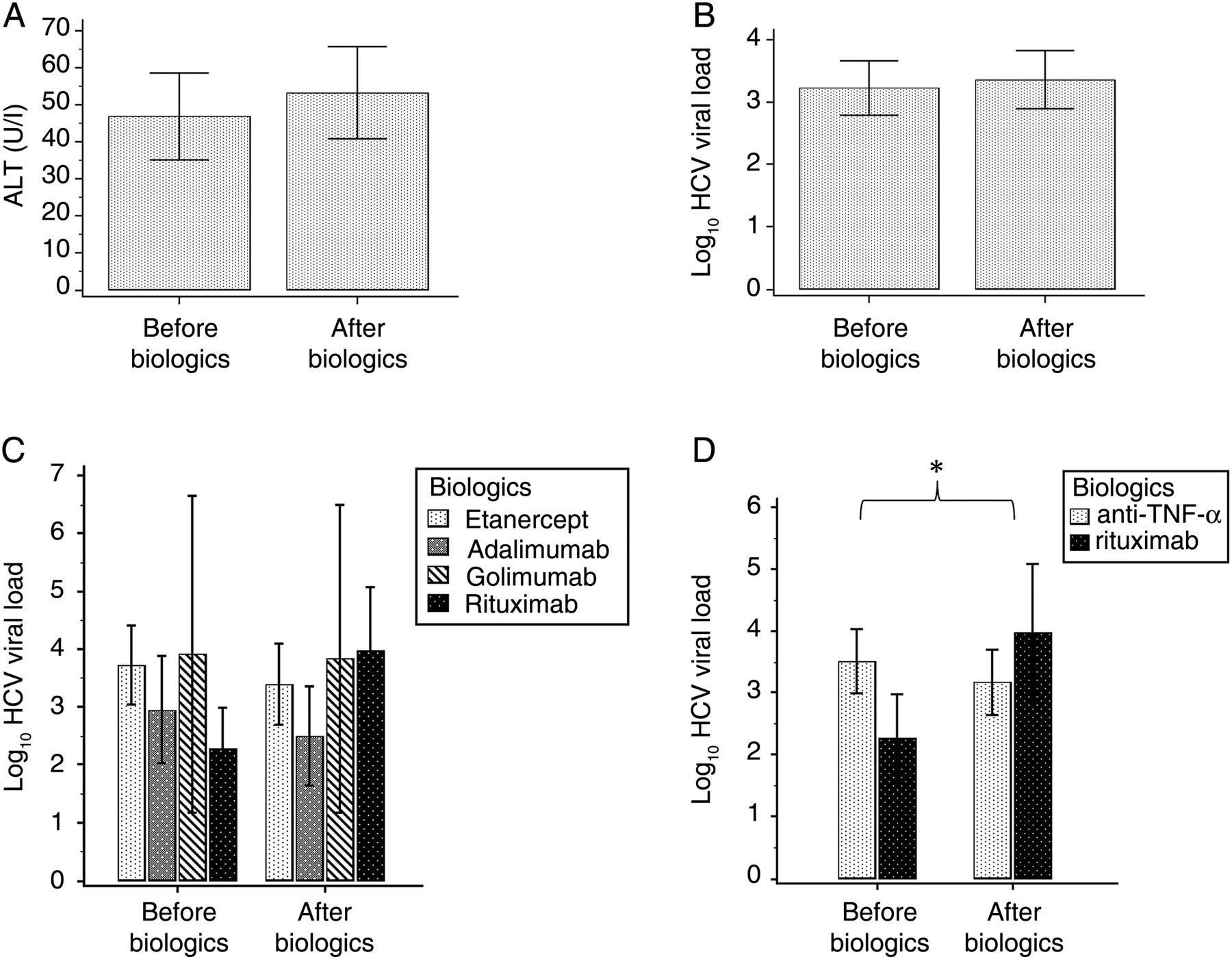
In total, 26 patients who fulfilled the 1987 revised criteria of the American College of Rheumatology (ACR) for RA and HCV infection were enrolled (table 1). Most of them had high disease activity.8 Anti-TNF-α agents were used in 20 patients (etanercept 12, adalimumab six and golimumab two), while six of them received RTX treatment. Serum alanine aminotransferase (ALT) and HCV viral load were measured before and after biological therapy. The mean duration of biological treatment was 25.8±16.7 months. There were no significant differences of serum ALT and HCV viral activity between baseline and the end of biological treatment (figure 1A). HCV viral loads before and after various biological treatments are shown in figure 1B, C. When categorising biologics by mechanism of action, there was a statistically significant difference in changes of HCV viral load between anti-TNF-α treatment and RTX therapy (figure 1C, p=0.003). The HCV viral load increased after RTX therapy. However, anti-TNF-α treatment did not seem to affect HCV viral replication.
Demographic data and laboratory findings of rheumatoid arthritis (RA) patients with HCV infection receiving anti-TNF-α and rituximab therapy*

{kind=link}
Comparisons of (A) serum alanine aminotransferase (ALT) and (B) hepatitis C virus (HCV) viral load before and after biological therapy by Wilcoxon signed-rank test. Biological treatments were categorised by (C) individual biologics and (D) mechanism of action. Data are mean±1 SEM. HCV viral loads were expressed as log10 of the detected values. *p=0.003 by generalised estimating equation.
Our study demonstrated B cell target therapy may influence HCV viral activity to a greater extent than TNF-α inhibitors. This preliminary result supports the 2012 update of the 2008 ACR recommendations for the use of etanercept in RA patients with history of hepatitis C.9 Our results showed that the use of adalimumab or golimumab for more than 2 years did not increase HCV viral replication. Further study is necessary to clarify whether anti-TNF-α agents other than etanercept are safe in this clinical setting.
Previous controlled trials have shown the good safety profile of RTX plus pegylated interferon-α and ribavirin in HCV-related cryoglobulinemia.10 However, consistent with previous studies of lymphoma,5 ,6 our results demonstrated a potential safety alert of using RTX plus traditional disease-modifying antirheumatic drugs in RA patients with HCV infection in absence of combination antiviral therapy. Although increased HCV viral load was not associated with elevated serum ALT levels, we observed a different impact on viral replication between anti-TNF-α agents and RTX. In our study, RTX patients were numerically older and treated with biologics for longer period of time but less likely to receive methotrexate than anti-TNF-α patients. All patients receiving RTX in this study had previous exposure to anti-TNF-α therapies in line with the reimbursement guidelines of the Taiwan National Health Insurance. Old age and prolonged immunosuppression therapy could also impair host immunity against HCV.
In conclusion, use of anti-TNF-α agents seems to be safe in RA patients with HCV infection. Careful monitoring of HCV viral load is suggested with RTX treatment if combination antiviral therapy for HCV is not given.
Acknowledgments
The authors are grateful to the Biostatistics Task Force of Taichung Veterans General Hospital, Taiwan, for assistance with statistical analysis.
References
Footnotes
-
Contributors All authors made substantial intellectual contributions to the conception of the work, analysis and interpretation of the data, and drafting and revising the manuscript.
-
Funding None.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The Ethics Committee of Taichung Veterans General Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.