Article Text

Statistics from Altmetric.com
Early recognition followed by treatment of rheumatoid arthritis (RA) helps to maintain joint integrity and functional capacity,1 suggesting it may be beneficial to intervene in patients with arthralgia before RA develops. Anticitrullinated protein antibodies (ACPA) and rheumatoid factor (RF) are established predictive markers,2 ,3 but only 20–40% of ACPA and/or RF positive patients with arthralgia develop RA within 2 years.4 Recently, we have demonstrated that the type I interferon (IFN) signature correctly identifies 52% of patients with arthralgia who will develop RA within 2 years.5 ,6 Our previous study suggested that a B cell related gene signature was associated with protection against arthritis development,6 and could aid in the prediction of arthritis development. We therefore studied the clinical value of the B cell signature, comprising CD19, CD20, CD79α and CD79β, for the prediction of arthritis development in an independent cohort of 115 ACPA and/or RF positive patients with arthralgia followed for median 22 months5 and explored the phenotypical nature of this B cell signature. In total, 44 patients (38%) developed arthritis (defined as one or more swollen joints) within 2 years. Of these, 4 patients had undifferentiated arthritis and 40 patients fulfilled the 2010 American College of Rheumatology (ACR)/ European League Against Rheumatism (EULAR) criteria for RA. Patients were stratified into B cellhigh and B celllow based on receiver operating characteristics analysis using a cut-off that resulted in 73% specificity and 47% sensitivity (a high B cell score is associated with protection against arthritis). 73% of B cellhigh versus 54% of B celllow individuals did not develop arthritis (χ2, p="0.040). In a Cox-regression analysis a B cellhigh signature revealed protection compared with a B celllow signature (HR 0.50, 95% CI 0.26 to 0.98, p=0.042). Significance was lost after correction for RF and ACPA status (HR 0.63, 95% CI 0.32 to 1.3, p=0.19).
Combining the previously described IFN with the B cell signature correctly classified 82% (9 out of 11) of patients developing arthritis based on their IFNhighB celllow profile and 81% (25 out of 31) of the patients not developing arthritis based on the IFNlowB cellhigh profile (χ2, p<0.001). Patients with an IFNhighB celllow profile have an increased risk compared with patients with an IFNlowB cellhigh profile, even after including ACPA and RF status (HR 5.6; figure 1A) and was considerably higher compared with the original IFNhigh profile alone (HR 2.4, p=0.008).5 No significant association was found with age, C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) in any of the analyses.

Combination of the type I interferon (IFN) and B cell signatures at inclusion in patients with arthralgia in relation to arthritis development. (A) Cox-regression analysis revealed that patients with the IFNhighB celllow profile had a significantly higher risk of developing arthritis (HR 5.6) compared with the IFNlowB cellhigh profile, corrected for anticitrullinated protein antibodies (ACPA) and rheumatoid factor (RF) status. (B) Receiver operating characteristics (ROC)-curve analysis of ACPA, RF, IFN and B cell score for 115 patients within a time-window of 2 years. The area under the curve (AUC) for ACPA and RF of 0.62 increased to a good AUC of 0.79 when only the IFN score is included or when the IFN and the B cell scores are included. (C) ROC-curve in 25 seropositive IFNhigh patients revealed an AUC of 0.82 for ACPA and RF, which increased to a very good AUC of 0.90 after including the B cell score. (D) ROC-curve in 90 seropositive IFNlow patients revealed an AUC of 0.60 for ACPA and RF and this increased to a good AUC of 0.73 after including the B cell score.
Clinical relevance of the biomarkers was established by receiver operating characteristics analyses. For ACPA and RF the area under the curve (AUC) was 0.62, combined with the IFN-score this increased to 0.79. Adding the B cell score did not improve the AUC (0.79; figure 1B). However, a two-step analysis, in which RF and/or ACPA positive patients were first stratified in an IFNhigh group (to predict arthritis development) and an IFNlow group (to predict not developing arthritis), revealed an AUC for ACPA and RF of 0.82 and 0.60, respectively, which increased to 0.90 and 0.73 after adding the B cell score (figure 1C, D).
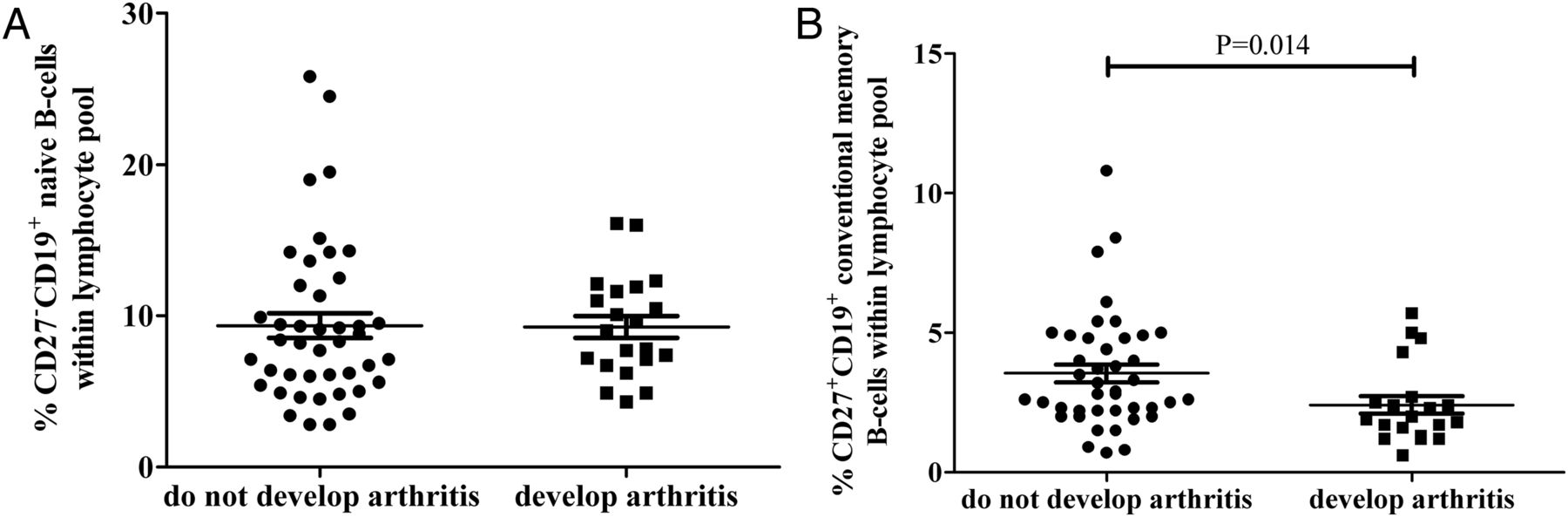
Flow cytometry analysis, in a representative subgroup (n=63; ie, flow cytometry measurements were included at approximately the second half of cohort, but characteristics are similar to the whole cohort) showed a positive correlation between the B cell score and the absolute B cell number (ρ=0.73, p<0.001). While the proportion of CD27−CD19+ naive B cells did not differ between the groups, the proportion of CD27+CD19+ conventional memory B cells was significantly higher in the non-converting patients (p=0.014; figure 2A, B). In conclusion, the combination of the B cell and previously described type I IFN signature represents a clinically useful biomarker to predict arthritis development in seropositive patients with arthralgia. The B cell score corresponds to conventional memory B cell numbers in the periphery which might indicate that this B cell subset plays a critical role in the preclinical phase of arthritis.
{kind=link}
{kind=link}
B cell subsets measured by flow cytometry in 63 patients with arthralgia. (A) Scatter plot of the CD27−CD19+ naive B cells within the lymphocyte pool revealed no differences between patients with arthralgia who develop arthritis and patients with arthralgia who do not develop arthritis. (B) Scatter plot of CD27+CD19+ conventional memory B cells within the lymphocyte pool revealed that patients with arthralgia who do not develop arthritis had a significantly higher percentage of memory B cells than patients with arthralgia who develop arthritis.
Acknowledgments
The authors thank S de Ridder of the inflammatory disease profiling unit, department of Pathology, for contributing to flow cytometry data conversion. The authors also thank technicians of the Unit of Medical Immunology, department of Pathology, for their help with flow cytometry data collection.
Footnotes
Funding This research was performed with support from the ‘TRACER’ consortium in the framework of the Center for Translational Molecular Medicine (CTMM) (http://www.ctmm.nl)
Competing interests DvS and CLV are inventors on a patent application, where the use of the gene signatures for the diagnosis of preclinical RA is described.
Patient consent Obtained.
Ethics approval Centrale Commissie Mensgebonden Onderzoek Slotervaartziekenhuis en Reade.
Provenance and peer review Not commissioned; externally peer reviewed.