Article Text

Abstract
Objectives To document the current training, implementation and role of modern musculoskeletal imaging techniques: ultrasound, magnetic resonance imaging, computed tomography and positron emission tomography, among rheumatologists in the member countries of the EULAR.
Methods English-language questionnaires for each imaging modality developed by a EULAR task force were sent out to national and international scientific societies as well as imaging experts in the given modalities involved in research and/or training. The surveys were distributed via an online survey tool (SurveyMonkey). Simple descriptive and summary statistics were calculated from the responses.
Results More than 90% of ultrasound (US) experts reported the availability of a US unit in their department. Suspicion of rheumatoid arthritis and spondyloarthritides were the main clinical indications for performing US for diagnostic purposes. Suspicion of sacroiliitis and degenerative spine disease were the most common indications to perform magnetic resonance imaging (MRI) or computed tomography (CT) for diagnostic purposes, while positron emission tomography was mainly performed to diagnose large vessel vasculitis and to investigate fever of unknown origin. The reported percentage of rheumatologists performing US was highly variable, ranging from more than 80% in 6% of countries to less than 10% in 15% of countries. The majority of experts (77%) reported that their national rheumatology societies organise musculoskeletal US courses, while courses in MRI or CT organised by the national rheumatology societies were less commonly reported (29% and 8%, respectively).
Conclusions Rheumatologists in Europe utilise modern imaging techniques; however, access to the techniques and training offered is varied.
- health services research
- MRI
- ultrasonography
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Emerging musculoskeletal imaging techniques are indispensable tools both in clinical practice and in research in rheumatology.
What does this study add?
This is the first survey on the use of ultrasound, MRI, CT and positron emission tomography among rheumatologists in EULAR countries.
While modern imaging techniques are available to rheumatologists in EULAR countries, access to the techniques and training offered is varied.
How might this impact on clinical practice?
Data provided by our study may help to design an educational strategy for EULAR.
Intoduction
Over the past decade, emerging musculoskeletal imaging techniques have become indispensable tools both in clinical practice and in research in rheumatology.1 2 While conventional radiography is performed generally by radiologists (but interpreted also by rheumatologists), modern imaging methods, that is, ultrasound (US), magnetic resonance imaging (MRI), computed tomography (CT) and positron emission tomography (PET), are increasingly utilised and requested by rheumatologists. US machines are commonly applied as diagnostic and monitoring tools in rheumatological departments and private practices.3–5 While PET, CT and MRI are generally operated and performed by radiologists; there are dedicated MRI (eg, extremity MRI) and micro-CT units in individual rheumatological centres solely under the control or catering specifically to the needs of rheumatology departments.6–8 In addition, there is a growing network of European centres performing research on the use of PET (both PET–MRI or PET–CT) in rheumatic diseases.9 Appropriate training is highly important to ensure skilled use and accurate interpretation of findings by rheumatologists. The EULAR has facilitated a number of educational efforts on modern imaging techniques, including publications on education, curriculum and competency,10–12 a range of online and live courses dedicated to imaging, a structured competency assessment system for musculoskeletal US (MSUS) in rheumatology (www.eular.org), as well as the EULAR Imaging Library (https://esor.eular.org).
The uptake and use of these techniques developed very differently across Europe and data are scarce and limited exclusively to US3–5 on their present impact on rheumatology for individual European countries.13–16
The objective of this task force was, therefore, to document the current implementation, role and training in modern MS imaging techniques among rheumatologists in EULAR countries.
Methods
Study design
English-language questionnaires for each imaging modality developed by a EULAR task force composed of rheumatologist experts in imaging were sent out to national and international organisations: (i) national rheumatology societies of EULAR (No.: 45); (ii) national societies of the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) (No.: 29); (iii) national societies of the European Federation of Societies for Magnetic Resonance in Medicine and Biology (No.: 13) and (iv) EULAR Emerging Network country liaisons (No.: 45). In addition, the questionnaires were sent to European rheumatologist experts (201 selected as follows: persons designated by national societies responsible for education and training in imaging, contact persons/conveners of EULAR Network of Imaging Research and Training Centers, EFSUMB representatives for MSUS in rheumatology, delegates (national and co-opted) of the EULAR Standing Committee of Musculoskeletal Imaging, faculty members on at least three official EULAR or EULAR-endorsed MSUS courses in the last 5 years, faculty members of the EULAR Imaging Course, and experts in CT, MRI and PET–CT/MRI involved in research and/or training known as steering committee members. The surveys were distributed via an online survey tool (SurveyMonkey) in late 2017 to early 2018. The questionnaire was accompanied by an explanation regarding the purpose of the survey. Non-responding persons and organisations were sent a reminder after 8, 12 and 26 weeks.
Questionnaire design
The questions contained in the questionnaires were divided into three broad sections: demographics, practice of imaging methods, and training and education in the methods available to rheumatologists. Questions on demographics requested information concerning the country of the responder. Questions on clinical use and on training and education requested information concerning the country of the responder as well as the responder as an individual. Each survey contained between 41 and 45 questions, the majority of which were multiple choice questions, while a minority were simple choice or open-ended questions. With regard to the analysis of questions on the use of the techniques at the country level, in case of countries where more than one participant filled the questionnaire, a representative participant (ie, respondent delegated by the national society or senior expert as identified by the steering committee) was chosen. Simple descriptive and summary statistics were calculated from the questionnaire responses.
Results
When considering all imaging techniques combined, we have received a response from 34 out of 45 (76%) EULAR countries: 76% (34/45) for US, 69% (31/45) for MRI, 53% (24/45) for CT and 56% (25/45) for PET. An email containing the links to all four surveys were sent to a total of 279 imaging experts, of whom 188 filled one or more survey, resulting in a total number of 278 surveys filled. Five participants filled the same survey twice, and one survey was sent by a participant outside of Europe, therefore resulting in a final number of 272 surveys analysed. Distribution of respondents according to the country is shown in online supplementary file 1.
Supplemental material
Musculoskeletal ultrasound
A total of 138 surveys were collected from 132 experts in US (five respondents filled the survey twice and one survey was filled by a respondent out of the region), from 34 out of 45 (76%) countries of EULAR. The total number of surveys analysed was 132. The overwhelming majority of respondents, 94% (124/132), were rheumatologists, and had ≥5 years of experience in US (online supplementary file 2). About 98% (129/132) had access to a US unit in their department and more than two-thirds (92/132) are certified in US by EULAR (online supplementary file 2). Rheumatoid arthritis and spondyloarthritides were the main clinical indications for performing US in their clinical practice for both diagnostic and management purposes (figure 1). The most commonly examined structures were the wrist, knee, shoulder, finger and ankle joints, while the most common target structures for US-guided intervention were the shoulder, wrist, knee, elbow, ankle and hip (online supplementary files 3 and 4).
Supplemental material
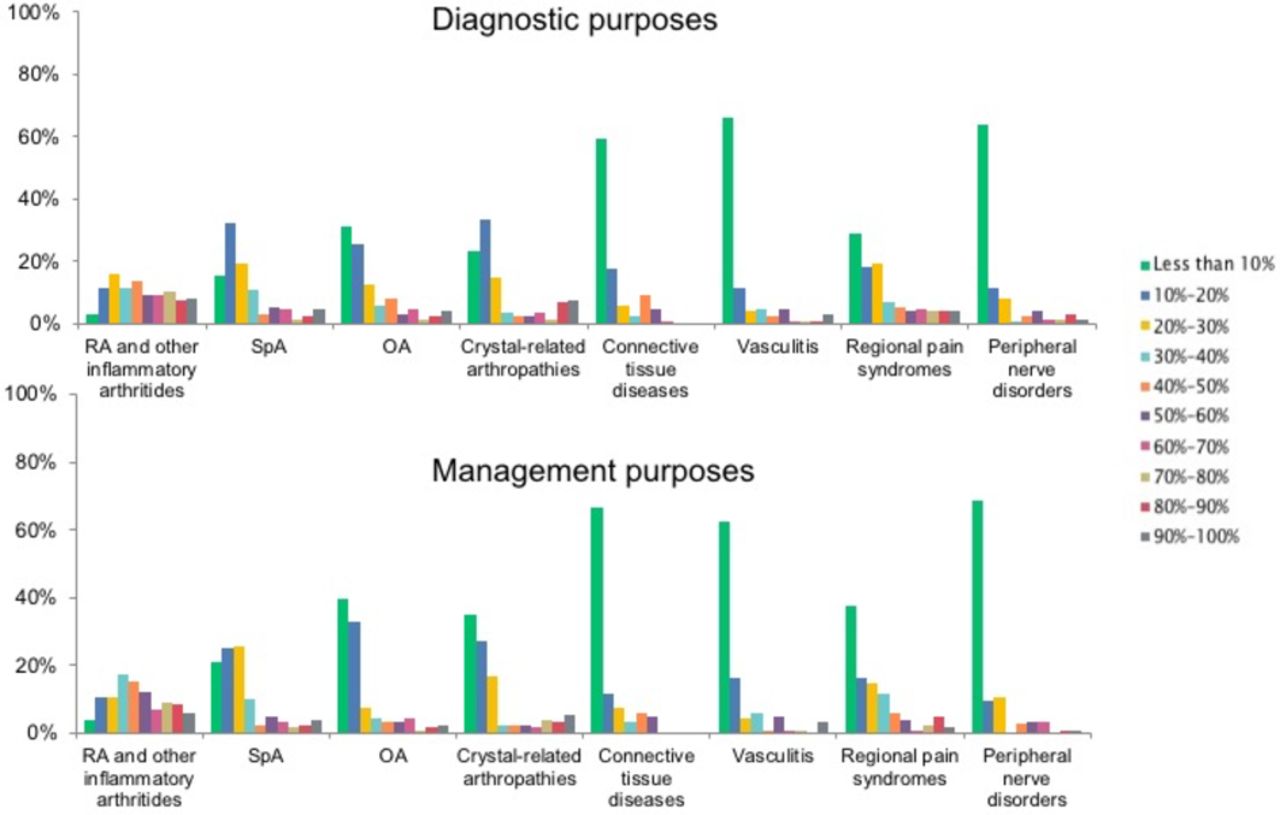
Percent of patients with suspected or confirmed rheumatic disease in which musculoskeletal ultrasound is performed for diagnostic or management purposes. OA, osteoarthritis; RA, rheumatoid arthritis; SpA, spondyloarthritis.
There was considerable variability in the percentage of rheumatologists performing US among the EULAR countries. About 29% (10/34) of participating EULAR countries reported that US is performed by 10%–20% of rheumatologists, 26% (9/34) reported that it is performed by 20%–40%, 18% (6/34) reported that it is performed by 40%–60%, 15% (5/34) reported that it is performed by less than 10%, 6% (2/34) reported that it is performed by 60%–80% and 6% (2/34) reported that it is performed by more than 80% of rheumatologists (figure 2). Likewise, the use of US-guided injections was highly variable among these countries. About 44% (15/34) of participating EULAR countries reported that US-guided interventions are performed by 10%–20% of rheumatologists, 26% (9/34) reported that it is performed by less than 10% of rheumatologists, 9% (3/34) reported that it is performed by 40%–60%, 6% (2/34) reported that it is performed by 20%–40%, 3% (1/34) and 3% (1/34) reported that it is performed by 60%–80% and more than 80%, respectively, and 9% (3/34) reported that it is unknown (online supplementary file 5). The percentage of rheumatologists who have been trained in US in EULAR countries is shown in online supplementary file 6. Overall, the countries those reported a high percentage of rheumatologists performing US also reported a high percentage trained in the method.
Supplemental material
Supplemental material
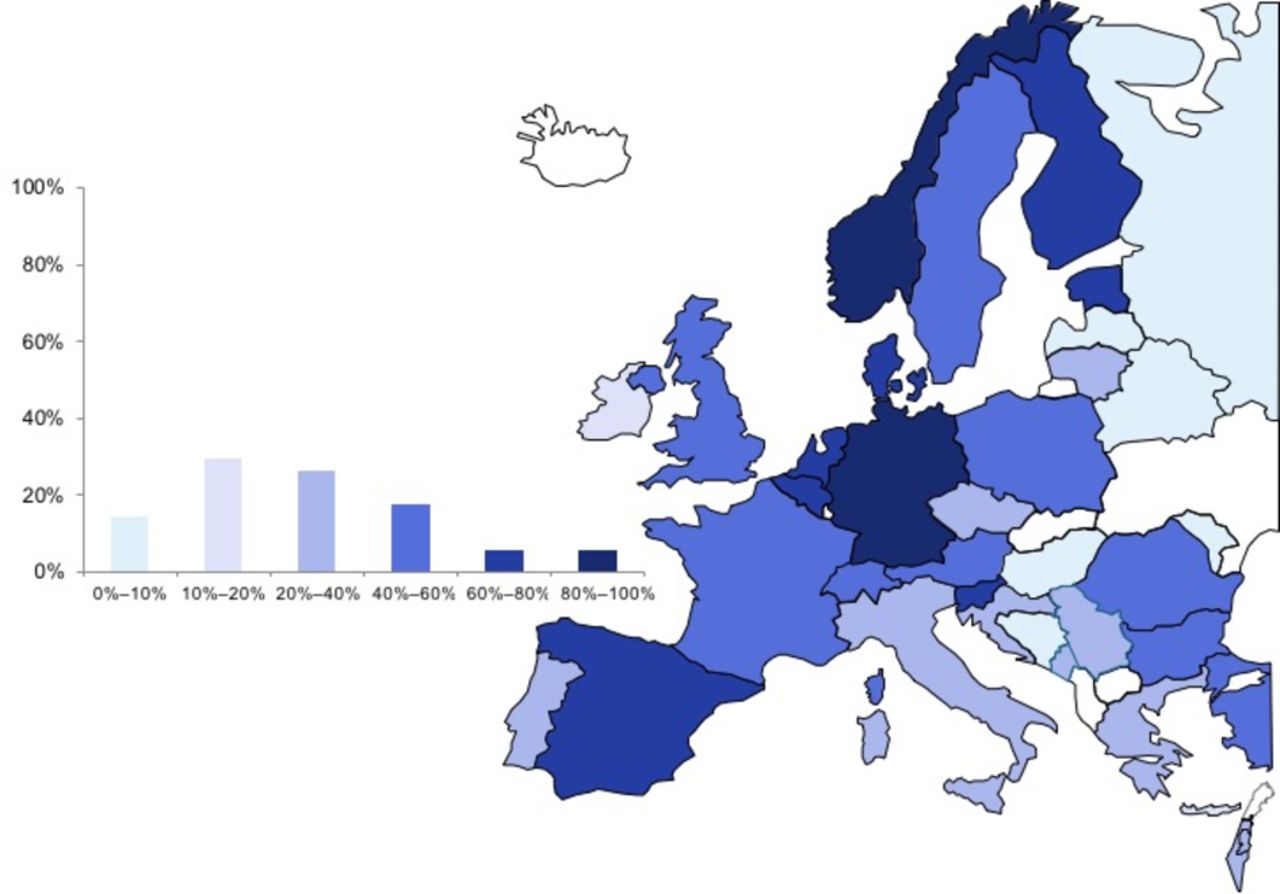
Percentage of rheumatologists performing musculoskeletal ultrasound among member countries of the European League Against Rheumatism.
About 92% (121/132) of respondents educate rheumatologists and other specialists in the use of US and 74% (98/132) perform research in US. Training in US is included in the national training curricula for rheumatologists in 65% (22/34) of participating countries, while competency is assessed in 70% (16/23) (figure 3). In the majority of countries, 68% (23/34) of the national rheumatology societies organises courses in US, the overwhelming majority of which are multilevel courses (figure 3). Competency, however, is assessed in only 54% (14/26) of such courses. Rheumatologists (in public and/or private practice) receive reimbursement for US in 62% (30/34) of countries. In 15% (5/34) of countries, there are national registers of rheumatologists performing US and 53% (18/34) reported that there is a committee/subgroup in the national society of rheumatology responsible for practice and/or training in US.

Training opportunities in musculoskeletal ultrasound among member countries of the European League Against Rheumatism. (A) Inclusion of training in musculoskeletal ultrasound in the national training curricula for rheumatologists; (B) Training course(s) in musculoskeletal ultrasound organised by the National Rheumatology Society and (C) Available levels of training in musculoskeletal ultrasound as provided by the National Rheumatology Society.
Magnetic resonance imaging
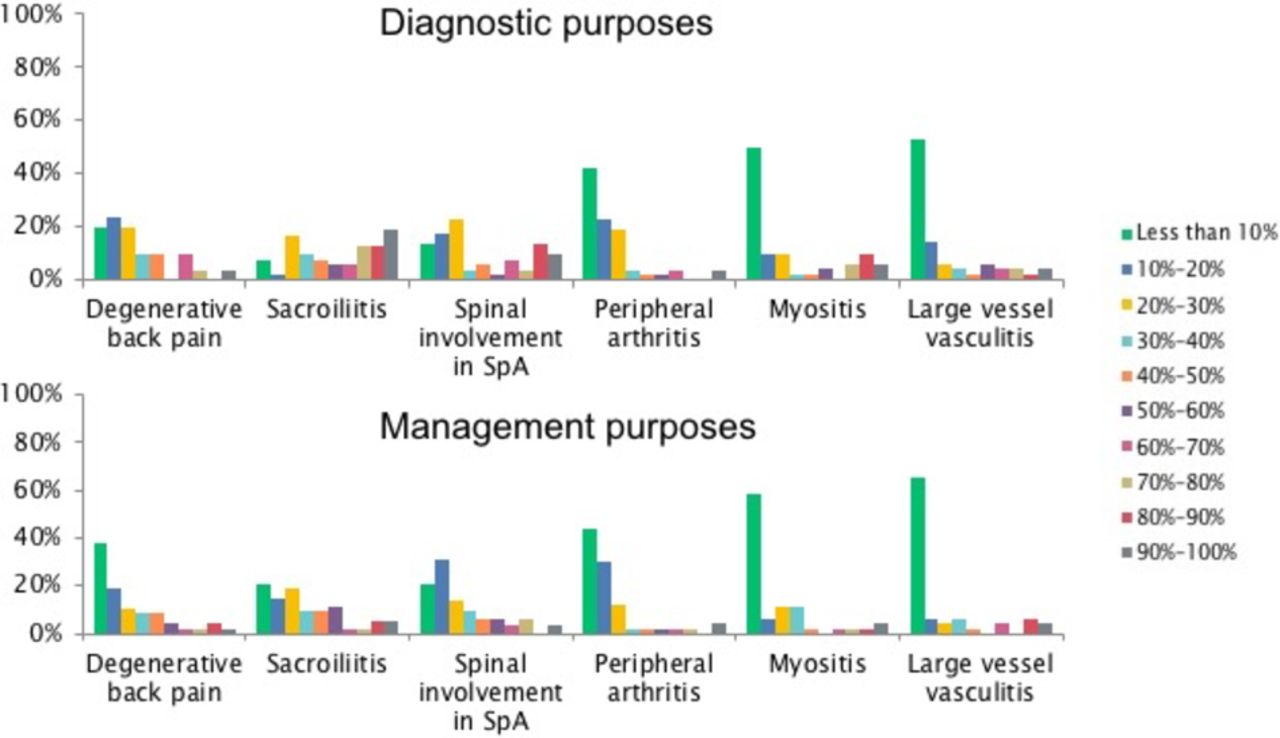
A total of 55 surveys from 55 experts in MRI from 31 out 45 (69%) EULAR countries were collected and analysed. The overwhelming majority of respondents, 85% (45/55), were rheumatologists, and had ≥5 years of experience in reading MRI (online supplementary file 7). About 75% (41/55) of experts had access to an MRI unit in another department (eg, radiology) in their centre, and 22% reported having an MRI unit in their department (12/55 respondents, 6 of whom, however, were radiologists) (online supplementary file 7). About 47% (26/55) of respondents reported that their MRI is read by a radiologist, 40% (22/55) reported that both the radiologist and the rheumatologist read the MRI and only 13% (7/55) reported reading the MRI themselves (online supplementary file 7). In clinical practice, the respondents reported local or joint-level diagnosis followed by global or patient-level diagnosis, and making decisions on systemic therapy as the most common reasons for requesting musculoskeletal MRI (online supplementary file 8). With regard to medical conditions, sacroiliitis and degenerative spine disease are the most common indications to request MRI for both the diagnostic and management purposes (figure 4). About 53% (29/55) of respondents educate rheumatologists and other specialists in the use of MRI and 56% (31/55) perform research in MRI.
Supplemental material
Supplemental material
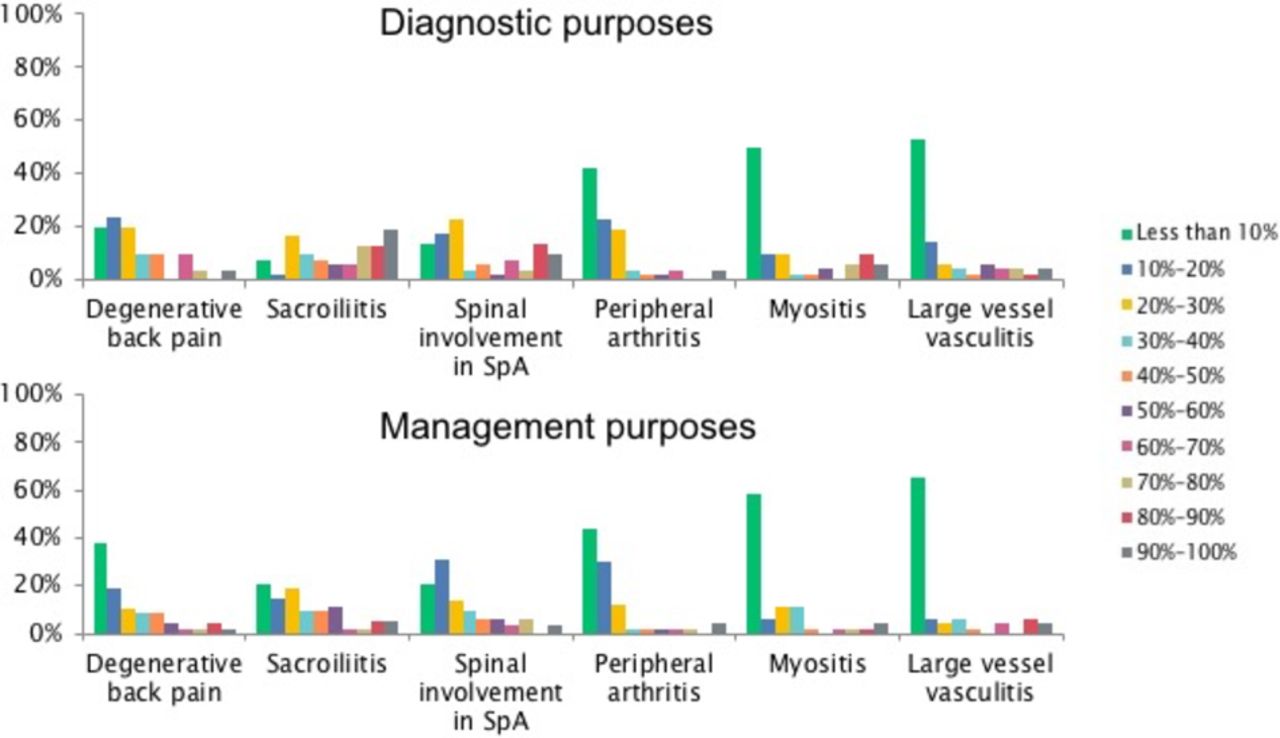
Percent of patients with suspected or confirmed rheumatic disease in which MRI is performed for diagnostic or management purposes. SpA, spondyloarthritis.
The majority of participating EULAR countries, 65% (20/31), reported that 80%–100% of rheumatology departments in the country have access to MRI, and only 13% (4/31) reported less than 10% of rheumatology departments having access to MRI (figure 5). Training in MRI is included in the national training curricula for rheumatologists in only 10% (3/31) of participating countries, and competency is not assessed. About 29% (9/31) of national rheumatology societies of EULAR countries organise courses in MRI; however, competency is assessed in only 17% (2/12) of countries (online supplementary file 9). A single country (Serbia) reported that rheumatologists receive reimbursement for reading MRI in private practice. None of the countries reported having a national register of rheumatologists reading MRI. Three countries (Austria, Netherlands and Poland) reported having a committee/subgroup in the national society of rheumatology responsible for practice and/or training in MRI.
Supplemental material

Percentage of rheumatologists reading MRI (A) and CT (B) among member countries of the European League Against Rheumatism.
Computed tomography (including dual-energy and micro-computed tomography)
A total of 39 surveys from 39 experts from 24 out of 45 (53%) countries of EULAR were collected and analysed. The majority of respondents 90% (35/39), were rheumatologists, and had ≥5 years of experience in this imaging modality (online supplementary file 10).
Supplemental material
About 85% (33/39) reported having easy access to a CT unit in another department (eg, radiology department) in their centre, 10% reported having a CT unit in their department (four respondents, three of whom, however, were radiologists) and 5% (2/39) reported having no access to CT (online supplementary file 10). About 69% (27/39) of respondents reported that their CT is read by a radiologist, 21% (8/39) reported that both the radiologist and the rheumatologist read the CT and only 10% (4/39) reported reading the CT themselves (online supplementary file 10). Sacroiliitis and degenerative spine disease are the most common indications to request CT for both the diagnostic and management purposes (online supplementary file 11).
Supplemental material
The majority of participating EULAR countries, 63% (15/24), who responded to our survey, reported that 80%–100% of rheumatology departments in the country have access to CT, and only 4% (1/24) reported that less than 10% of rheumatology departments have access to CT (figure 5). Training in CT is included in the national training curricula for rheumatologists in only 4% (1/24) of participating countries (competency is not assessed), and only 8% (2/24) of national rheumatology societies of EULAR countries organise courses in CT (competency is not assessed) (online supplementary file 12).
Supplemental material
Positron emission tomography
A total of 46 surveys from 46 experts in PET (both PET/MRI and/or PET/CT) from 25 out of 45 (56%) EULAR countries were collected and analysed. The majority of respondents, 80% (37/46), were rheumatologists, and had ≥5 years of experience in this imaging modality (either performing the technique in their department or collaborating with a centre performing PET (eg, nuclear medicine department) (online supplementary file 13). The overwhelming majority of experts, 95% (41/43), utilise PET–CT, 9% (4/43) utilise PET–MRI and 12% (5/43) utilise standalone PET (respondents were allowed to indicate more than one option). About 93% (39/42) of experts request or perform whole-body PET, while 10% (4/42) reported targeted examinations (eg, detailed scans of joints or spine/pelvis depending on the research question or clinical indication). Large vessel vasculitis, fever or increased erythrocyte sedimentation rate of unknown origin were the most common indications to request PET for diagnostic purposes (figure 6). For the purpose of decisions on systemic therapy, large vessel vasculitis was the most commonly reported indication (figure 6). Other indications not listed but reported by the experts included sarcoidosis, immunoglobulin G4-related disease, total joint replacement, constitutional symptoms, suspicion of malignancy, polymyalgia rheumatica and suspicion of osteomyelitis. About 52% (24/46) of respondents reported doing research in PET. The majority of experts, 80% (38/46), reported having no access to training courses in PET. Access to PET technique was varied in EULAR countries (online supplementary file 14).
Supplemental material
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percent of patients with suspected rheumatic disease in which positron emission tomography is performed for diagnostic purposes or for making decisions on systemic therapy. ESR, erythrocyte sedimentation rate; LVV, large vessel vasculitis.
Discussion
This is the first survey aiming to encompass all modern imaging methods commonly utilised by rheumatologists in EULAR countries. While there have been previous surveys focusing on the use of US in European countries3–5 by rheumatologists, no survey has been performed on the use of other techniques, such as MRI, CT and PET, among rheumatologists. By including questions concerning both national societies and individual responders, the surveys allowed us to gain an understanding of both practice and training in the techniques. When considering the distribution and number of participants who have filled our survey, with some exceptions, this corresponds roughly to activity in imaging research and education among the different countries.
Compared with the previous surveys on MSUS,3 4 the results of our survey demonstrate a growing uptake in the use of MSUS by rheumatologists, both in terms of rheumatologists performing MSUS, as well as MSUS-guided interventions, as well as in the training in both the MSUS and MSUS-guided interventions.3 In 2010, 56% of EULAR countries who participated in the survey reported less than 10% of rheumatologists performing MSUS routinely as compared with 15% reporting less than 10% in our current study (figure 2).3 In 2009–2010, MSUS was an obligatory or optional/recommended part of the curricula in 23%–35% of EULAR countries, being competency, however, assessed in only 19%.3 Currently, training in MSUS is included in the national training curricula in 65% of participating countries, while competency is assessed in 70% (figure 3A and B). About 68% of national rheumatology societies organises courses in MSUS, the overwhelming majority of which are multilevel courses, as compared with 40% of countries reported in our previous study, mostly consisting of one-level training4 (3C). Competency is assessed in 54% of courses, up from 20%.4
CT and MRI are generally accessible to rheumatologists in most EULAR countries, while access to PET is varied. Only a small fraction of rheumatologists read their MRIs and CTs themselves, although a sizeable fraction reported reading these examinations in addition to being read by radiologists. This scenario may be related to the fact that, compared with US, training in MRI, CT or PET is still quite limited for rheumatologists. Further efforts in education in these imaging modalities, which have become essential in the field of rheumatology, would possibly facilitate the more efficient use of these techniques by rheumatologists in clinical practice.
Our survey shows an updated overview on the use of imaging by rheumatologists in Europe with a considerable representation of experts and countries. Certain limitations, however, could not be avoided. Due to the fact that we surveyed imaging experts, participation bias could not be avoided, which may have led to an overestimation of the use and impact of modern imaging methods in rheumatology. Additionally, the high interest among responders in a given imaging technique (in particular, CT, MRI and PET, which are generally not directly controlled by rheumatologists) could have also led to overestimated or skewed practice characteristics within the countries. Despite a good overall response, a number of countries have not provided information, and in many countries, we received information from only single experts in a given imaging technique, which introduces bias to the results. In order to enhance the response rate, we had to limit the overall length and themes covered by the surveys, which meant that we could not explore among others, the use of imaging in paediatric rheumatology. Furthermore, we did not collect data on the type or technical level of imaging equipment available, which would have enriched the results on implementation. More detailed queries on available courses and the quality and quantity of training required by the national curricula may have provided more insight into training in imaging methods.
EULAR has recently launched a number of initiatives those provide training in modern imaging techniques. These include the EULAR Online Course on Imaging in Rheumatic and Musculoskeletal Diseases; participants of this course also have the option to attend the EULAR Advanced Hands-On Imaging Workshop, a practical case-based event prior to the EULAR Annual Congress. In addition, EULAR also organises the EULAR Imaging Course, a comprehensive new course on conventional radiography, MRI, CT and MSUS. For the past 25 years, EULAR has been offering its own multilevel US course and also endorses numerous courses in MSUS worldwide. Nevertheless, based on the results of our survey, we can certainly conclude that a greater offer of training in imaging modalities (particularly non-MSUS) would be beneficial to improve the utilisation and use of modern imaging techniques among rheumatologists in Europe.
In conclusion, data provided by this survey may help to design an educational strategy for EULAR aiming at achieving homogeneous, high-quality performance and use of modern imaging modalities across its member countries, which is consistent with, and would enhance the mission of this organisation.
Supplemental material
Supplemental material
Acknowledgments
The task force acknowledges the work of the colleagues who offered their time and filled the surveys, mentioned as follows: Erik Aarntzen, Elke A Aarts, Aleksandr Aleshkevich, Raquel Almodovar, Ish Atchia, Juan J de Agustin de Oro, Nestor Avgoustidis, Marina Backhaus, Artur Bachta, Alexandra Balbir-Gurman, Peter V Balint, Dubravko Bajramovic, Asta Baranauskaite, Marko Barešić, Anastas Batalov, Florian Berghea, Daniel Blockmans, Mihai Bojinca, Hans-Peter Brezinschek, Elisabeth Brouwer, Kristyna Bubova, Marco Canzoni, Emma Beltrán Catalán, Paraskevi Charalambous, Christoph Charwat-Pessler, Sarang Chitale, Christakis Christodoulou, Maria C Cid, Marco A Cimmino, Melanie-Ivana Čulo, Berit Dalsgaard Nielsen, Nemanja Damjanov, Christian Dejaco, Andrea Delle Sedie, Elena Deseatnicova, Theo Dimitroulas, Nurten Duru, Iris Eshed, Cristina Estrach, João Madruga Dias, Christina Duftner, Sandra Falcao, Emilio Filippucci, Georgios Filippou, Maria Filkova, Stephanie Finzel, Daniela Fodor, Jan Freeston, Floris van Gaalen, Frederique Gandjbakhch, Philippe Gaudin, Dana Georgescu, Andor Glaudemans, David Glinatsi, YPM Goekoop-Ruiterman, Benoit Le Goff, Robbert Gokoop, Anja Tea Golubić, Miguel A Gonzalez-Gay, Winfried Graninger, Walter Grassi, Simeon Grazio, Cees Haagsma, Espen Haavardsholm, Hilde-Berner Hammer, Wolfgang Hartung, Ellen-Margrethe Hauge, Ida K Haugen, Ahmed Ould Hennia, Alojzija Hocevar, Christian Høili, Iztok Holc, F Hoffmann, Jana Hurňáková, Nevsun Inanc, Iustina Janta, Pavel Jeremias, Aleksandra Juszkiewicz, Georgios Kampakis, David Kane, Lars F Karoliussen, Zunaid Karim, Dimitrios Karokis, Gkikas Katsifis, Herbert Kellner, Yogan Kisten, Arnd Kleyer, Erik af Klint, Rainer Klocke, SM Van der Kooij, Marion C Kortekaas, Juhani M Koski, Karin Laas, Katerina Laskari, Damien Loeuille, Rik Lories, Riitta Luosujärvi, Marta Madej, Clara Malattia, Oliveira Margarida, Stefan Mariacher-Gehler, Isabel Martínez Rodríguez, Helena Marzo-Ortega, Jean Pierre Mattei, Yves Maugars, Miroslav Mayer, Hermann Mayr, Neil Mckay, Adam Mester, Mihaela Micu, Eugenio De Miguel, Anna Mihailova, Radovan Milenkovic, Yair Molad, Victoria Navarro-Compán, Rodina Nestorova, Spyros Nikas, Sarah Ohrndorf, Andrea Österbauer, Ivan Padjen, Øyvind Palm, Ellinas Panagiotis, Evgenia Pavlovskaya, Salih Pay, Katja Perdan-Pirkmajer, Joaquim Polido Pereira, Porin Peric, Tzvetanka Petranova, Andres Pille, Laura Pirilä, Philip Platt, Denis Poddubnyy, René P Poggenborg, Sergio Prieto-González, Ioannis Raftakis, Amalia Raptopoulou, Darina Renčková, Doron Rimar, Charlene Rinkin, Ana Rodríguez, Krešimir Rukavina, Adeline Ruyssen-Witrand, Carlo Salvarani, Fernando Saraiva, Judith Sautner, Wolfgang Schmidt, Carlo A Sciré, Verena Schönau, Teodora Serban, Russka Shumnalieva, Caterina Siagkri, Inês Silva, Maria MRM Silva, Riemer Slart, Sekib Sokolovic, Miguel Sousa, Irina Starodubtseva, Maria Stoenoiu, Marcin Szkudlarek, Iwona Sudoł-Szopińska, Sofia Symeonidou, Allister Taggart, Giorgio Tamborrini, Ai Lyn Tan, Ender Terzioglu, Jacqueline Uson, Isabelle Chary-Valckenaere, Maja Vida, Marijne Vis, Violeta M Vlad, Jelena Vojinovic, Alexander Volkov, Paraskevi Voulgari, Florentin Vreju, Sakari Vuoristo, Richard J Wakefield, Wassenberg, Claudia Weidekamm, Volkmar Weiler, Ruth Wittoek, Rafal Wojciechowski, Zulfugar Yusifov, Jakub Závada, Pedro Zarco, Michael Ziegelasch, Hans-Rudolf Ziswiler, Pascal Zufferey and Robert Zwolak.
References
Footnotes
Contributors PM and EN contributed to the study design, managed the study, collected and interpreted clinical data, drafted the manuscript and approved the final version. AC, PGC, XB, MAD, AI, CJvdL and MO contributed to the study design, interpretation of data, revised the manuscript and approved the final version.
Funding Funding for the SurveyMonkey account was provided by the EULAR (Project number: IMG014).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.