Article Text

Abstract
Purpose To analyse trends in hip fracture (HF) rates in patients with rheumatoid arthritis (RA) over an extended time period (17 years).
Methods This observational retrospective survey was performed by reviewing data from the National Surveillance System for Hospital Data, which includes more than 98% of Spanish hospitals. All hospitalisations of patients with RA and HF that were reported from 1999 to 2015 were analysed. Codes were selected using the Ninth International Classification of Diseases, Clinical Modification: ICD-9-CM: RA 714.0 to 714.9 and HF 820.0 to 820.3. The crude and age-adjusted incidence rate of HF was calculated by age and sex strata over the last 17 years. General lineal models were used to analyse trends.
Results Between 1999 and 2015, 6656 HFs occurred in patients with RA of all ages (84.25% women, mean age 77.5 and 15.75% men, mean age 76.37). The age-adjusted osteoporotic HF rate was 221.85/100 000 RA persons/ year (women 227.97; men 179.06). The HF incidence rate increased yearly by 3.1% (95% CI 2.1 to 4.0) during the 1999–2015 period (p<0.001) and was more pronounced in men (3.5% (95% CI 2.1 to 4.9)) than in women (3.1% (95% CI 2.3 to 4.1)). The female to male ratio decreased from 1.54 in 1999 to 1.14 in 2015. The average length of hospital stays (ALHS) decreased (p<0.001) from 16.76 days (SD 15.3) in 1999 to 10.78 days (SD 7.72) in 2015. Age at the time of hospitalisation increased (p<0.001) from 75.3 years (SD 9.33) in 1999 to 79.92 years (SD 9.47) in 2015. There was a total of 326 (4.9%) deaths during admission, 247 (4.4%) in women and 79 (7.5%) in men (p<0.001).
Conclusion In Spain, despite the advances that have taken place in controlling disease activity and in treating osteoporosis, the incidence rate of HF increased in both male and female patients with RA.
- Osteoporosis
- Rheumatoid arthritis
- Trend
- Hip fracture
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Patients with rheumatoid arthritis (RA) are at increased risk of osteoporosis and osteoporotic fractures.
RA is a risk factor for bone fracture in both men and women, with comparable risks of fractures at the vertebrae and hip.
What does this study add?
The trend of hip fractures rate in patients with RA in Spain is increasing.
This increase is more pronounced in men than in women.
There is a different epidemiological pattern in the incidence of hip fractures in patients with RA versus the general population: age-adjusted hip fracture rates in women versus men are near the unit; hip fractures in patients with RA occur, on average, 6 years earlier than in the general population.
How might this impact on clinical practice?
Patients with RA are to be monitored more closely to control bone loss and prevent fracture.
Introduction
Rheumatoid arthritis (RA), a systemic autoimmune disorder that primarily affects the synovial tissues, is one of the most debilitating types of arthritis and affects approximately 0.5%–2% of the world′s population.1 RA is characterised by functional disability, joint damage, reduced quality of life and premature mortality. The incidence of RA is two to three times more common in women than in men.2
Patients with RA are at increased risk of osteoporosis and osteoporotic HFs.3–6 Clinical studies have shown that the incidence of osteoporosis among patients with RA is two times higher than those without RA.6 Bone loss in RA has been associated with many factors, among which these three stand out: chronic inflammation, use of glucocorticoids and physical inactivity. The release of proinflammatory cytokines such as interleukin 1 (IL-1), IL-6 and tumour necrosis factor-α may cause the abnormal production of osteoclasts, thus disrupting the equilibrium between bone resorption and bone formation.5 7 Secretion of receptor activator of nuclear factor kappa B ligand by activated T lymphocytes has also been shown to induce the differentiation of synovial macrophages into osteoclasts, thereby leading to bone loss.8 9 Oral glucocorticoids, commonly used to suppress RA-induced inflammation, can promote the loss of bone mass by inhibiting the differentiation and activity of osteoblasts by blocking bone morphogenetic protein 210 or Wnt/beta-catenin pathways.11 In addition, immobility resulting from RA-induced inflammation, muscle pain, weakness and swelling may increase the risk of falling to a certain extent,12 thus raising the rate of bone fractures.
During the past 15 years, treatments for RA have significantly progressed due to the fact that they are applied much earlier and are more intensive in nature. Advances in the understanding of RA pathogenesis have significantly evolved during this period and have led the introduction of biological therapies and new strategies in the management of RA known as ‘treat to target’ (T2T).13 The use of osteoporosis treatments in patients with RA (especially bisphosphonates) has also become widely adopted, as has the development of new molecules (eg, teriparatide and denosumab), which have been incorporated into the therapeutic arsenal for patients with RA.14
For all of these reasons, it seems reasonable to venture that this new RA treatment paradigm may positively impact the incidence rate of HF in patients with RA. As far as we know, there is no study that has assessed the trend of HF in patients with RA.
Methods
A retrospective study using the national information system for hospital data (Minimum Basic Data Set (MBDS) or Conjunto Mínimo Básico de Datos (CMBD)) from the Ministry of Health was performed. This system contains information about the admission date, discharge date, age, sex, geographical region, diagnosis, clinical procedures and discharge status (eg, in-hospital death and recovery) for all hospitalisations in Spain. The CMBD uses clinical codes from the Spanish version of the Ninth International Classification of Diseases, Clinical Modification (ICD-9-CM), and it includes an estimated 98% of public hospital admissions, covering 99.5% of the Spanish population.15 We assumed that the remaining population and hospitalisation information not included in the study followed the same epidemiological characteristics.
The unit of analysis were all hospital discharges related to RA (ICD-9-CM: 714.0 to 714.9). All cases of proximal third of femur fractures corresponding to ICD-9 codes 820.0 to 820.9 were identified yearly over the study period. Only osteoporotic fractures were considered. Pathological fractures (733.1 to 733.19) (metastases, bone metabolic diseases such as Paget′s disease (M89.9), fractures of another femur location (ICD-9 821) or acetabular-pelvic fractures (ICD-9 808.0 to 808.9) were excluded, as well as fractures related to road accidents (V87.9). Readmissions within 30 days after discharge were eliminated, assuming that they were due to the same HF. For each case, specific data were gathered including demographic data (age, sex, place of residence), patient risk factors, comorbidities and complications during their hospital stay (secondary diagnoses), as well as the key diagnostic techniques used and surgical procedures performed.15 The following patient age groups were established: 20–39 years old, 40–59 years old, 60–79 years old and older than 80 years of age.
Statistical methods
The annual hospital admission rate (HAR) by sex, age group and year for the population at risk (see below) was calculated as the number of hospital discharges per 100 000 inhabitants/year. The numerators were the cases registered in the MBDS and the denominators were the population at risk (see below). Additionally, the age-adjusted incidence rates were estimated with 95% CI using the population at 2015 as the reference population. The study period covered (1 January 1999 through 31 December 2015) was divided into four periods: in three 4-year periods (the first from 1999 to 2002, the second from 2003 to 2006, the third from 2007 to 2010) and the fourth the 5-year period from 2011 to 2015). The population at risk was estimated based on the national census provided by the National Institute of Statistics and assumed a prevalence of RA of 0.5% (both sexes); specifically, 0.8% in women and 0.2% in men. This prevalence of RA is the one estimated in the EPISER study, the last national epidemiological study conducted in our country.16 The ALHS was the number of hospitalisation days averaged across all hospital discharges. The in-hospital case-fatality rate (CFR) was calculated as the number of deaths during the hospital stay divided by the total number of hospital discharges (percentage), and 95% CIs were calculated. The change in annual rates was analysed by generalised linear models (GLM) with Poisson distribution or negative binomial distribution, in cases of overdispersed data. The models were thus used to estimate the age-adjusted incidence rate ratio of the variable ‘year’ with 95% CI; the p-value of the association was noted as the result of the trend test. An interaction effect for age group and year was included to analyse differences in trends. The significance level was established at 1% to account for the use of aggregated data.
The following data were collected: gender, age, place of residence (nursing home or community), type of primary fracture (intracapsular or extracapsular), time to intervention and hospital length of stay. Additionally, the following risk factors for HF were identified using ICD-9-CM codes in any secondary diagnosis field: Cardiac Disease: ICD-9-CM:398.91, 404, 402.11, 402.91, 428–428.9; Dementia: ICD-9-CM: 290–290.9; Delirium ICD-9-CM: 298.9, 293.0, 293.9, 293.8; Chronic pulmonary disease ICD-9-CM: 490–496, 500–505, 506.4; Cancer ICD-9-CM: 140.0–172.9, 174.0–195.8, 200–208.9, V10.0–V10.9; Metastasic cancer: ICD-9-CM:196.0–199.99; Cerebrovascular disease ICD-9-CM: 430–438; Malnutrition: ICD-9-CM: 260–263.9; Diabetes: ICD-9-CM: 250.00–250.99; Myocardial infarction: ICD-9-CM: 410–410.9; Chronic renal failure: ICD-9-CM: 585–586.99, 582.0–582.9, 583.0–583.7, 588.0–588.9 and Anaemia: ICD-9-CM: 280.00–285.99. The age-adjusted Charlson Comorbidity Index (CCI) was computed for each patient. This index reflects the number and importance of comorbid diseases, relies on ICD-9-CM categories and was used to adequately adjust for severity of illness. Quantitative data are described by the mean and SD or median and IQR. Categorical data are expressed by counts and percentages. Differences by sex were tested with χ2 test, Student’s t-test and Mann-Whitney tests, as appropriate. In all tests, the significance level was p<0.05.
Statistical analyses were performed using IBM SPSS V.24.0, Epidat V.4.2 and Stata V.14 computer packages.
The present study received a waiver for informed consent from the local ethics committee (Comité de Ética de Investigación del Hospital U. Fundación Alcorcón). Patient information was anonymised and deidentified prior to the analysis.
Results
A total of 338 343 hospital admissions were reported for patients with RA during the 17-year study period. The 338 343 admissions corresponded to a total of 176 097 patients (117 985 women and 58 112 men).
Of the total hospital admissions, 6657 (2%) were due to HF. A number of 5609 (82.25%) out of this total occurred in women and 1048 (15.75%) in men. The mean patient age was 77.54 years (SD 9.6), 77.76 (SD 9.4) in women and 76.37 (SD 11.5) in men (p<0.001). The ALHS was 13.96 (SD 12.8), 13.98 (SD 12.2) in women and 13.82 (SD 15.8) in men (p=0.716). The mean value of the CCI was 1.66 (SD 1.08), 1.59 (SD 0.7) in women and 2.03 (SD 1.48) in men (p<0.001). A number of 6383 (95.9%) patients were admitted from the emergency room. There was a total of 326 (4.9%) deaths, 247 (4.4%) in women and 79 (7.5%) in men (p<0.001) (table 1).
Description of the patients with RA who suffered a hip fracture episode in Spain, between 1999 and 2015 and a comparison by sex
The HAR was 221.85/100 000 RA patients/year (95% CI 216.52 to 227.18) during the study period. Table 2 shows the HAR for each year (both genders), and table 3 shows the specific results by sex. As supplementary material, the HARs are shown by age-range and sex (online supplementary tables 1–3). The HAR increased exponentially with age (online supplementary figure 1). The curves were similar by sex. The HAR was higher in females, 304.83/100 000 RA patients/year (95% CI 277.81 to 333.77) versus 268.50/100 000 RA patients/year (95% CI 217.73 to 327.54) in males (p<0.001). Using GLM, an annual increase of 3.2% (95% CI 2.1 to 4, p<0.001) was observed for both sexes. In models stratified by gender, this increase was 3.1% (95% CI 2.3 to 4.1, p<0.001) in women and 3.5% (95% CI 2.1 to 4.9, p<0.001) in men (figure 1). Trends were different by age groups with interaction effect statistically significant. HAR increased in both men and women older than 80 years with an annual increase of 5.4% (95% CI 4 to 6.8, p<0.001), and in 60–80 years, this increase was 1.1% (95% CI 0.3 to 1.9, p=0.007). In 20–40 years and 40–60 years, HARs estimated a decrease of 2.7% (95% CI 1.3 to 4.1, p<0.001) and 3% (95% CI 2.1 to 3.8, p<0.001), respectively (figure 2). The female to male ratio decreased during the study period (from 1.54 in 1999 to 1.14 in 2015), reflecting the difference in the increased rates (table 3).
online supplementary material.
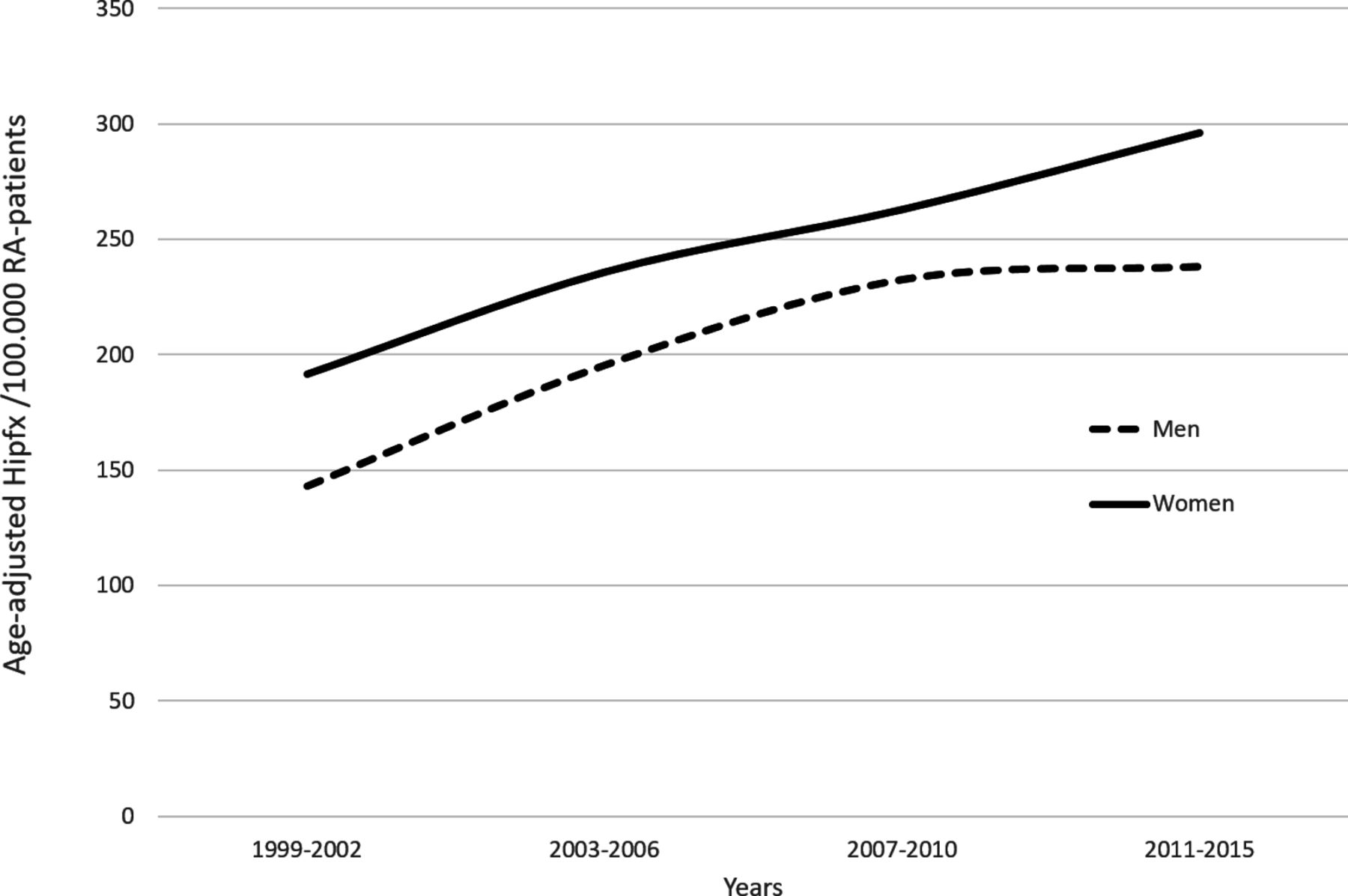
Age-adjusted hospital admission rate (HAR) (per 100 000 RA patients/year) during 1999–2015. RA, rheumatoid arthritis.
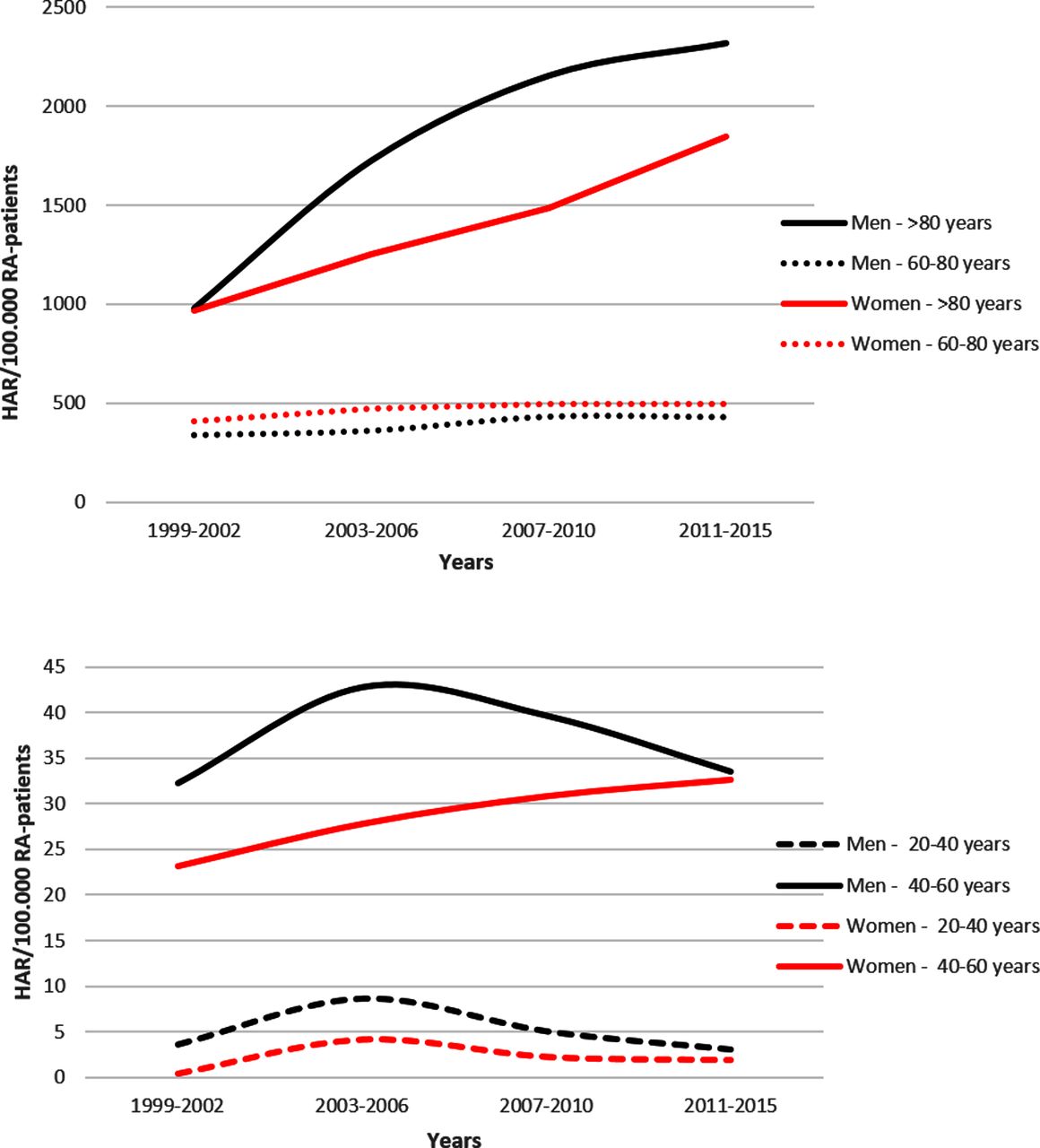
Hospital admission rate (HAR) of hip fractures (per 100 000 RA patients/year) by age range and sex. RA, rheumatoid arthritis.
Crude and age-adjusted HARs of hip fractures per 100 000 RA patients (of both sexes) by year
Crude and age-adjusted HAR of hip fractures per 100 000 RA patients by year and sex
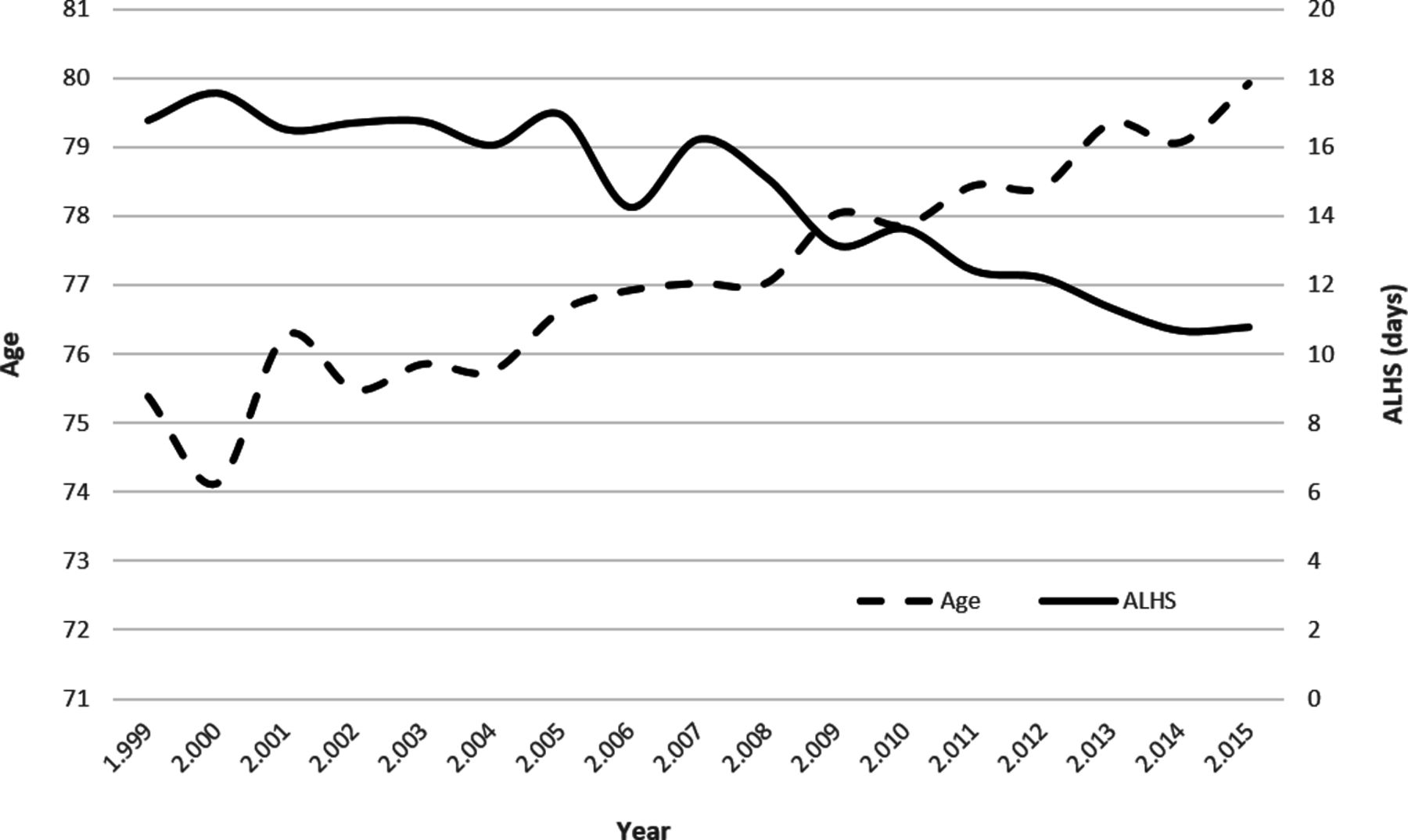
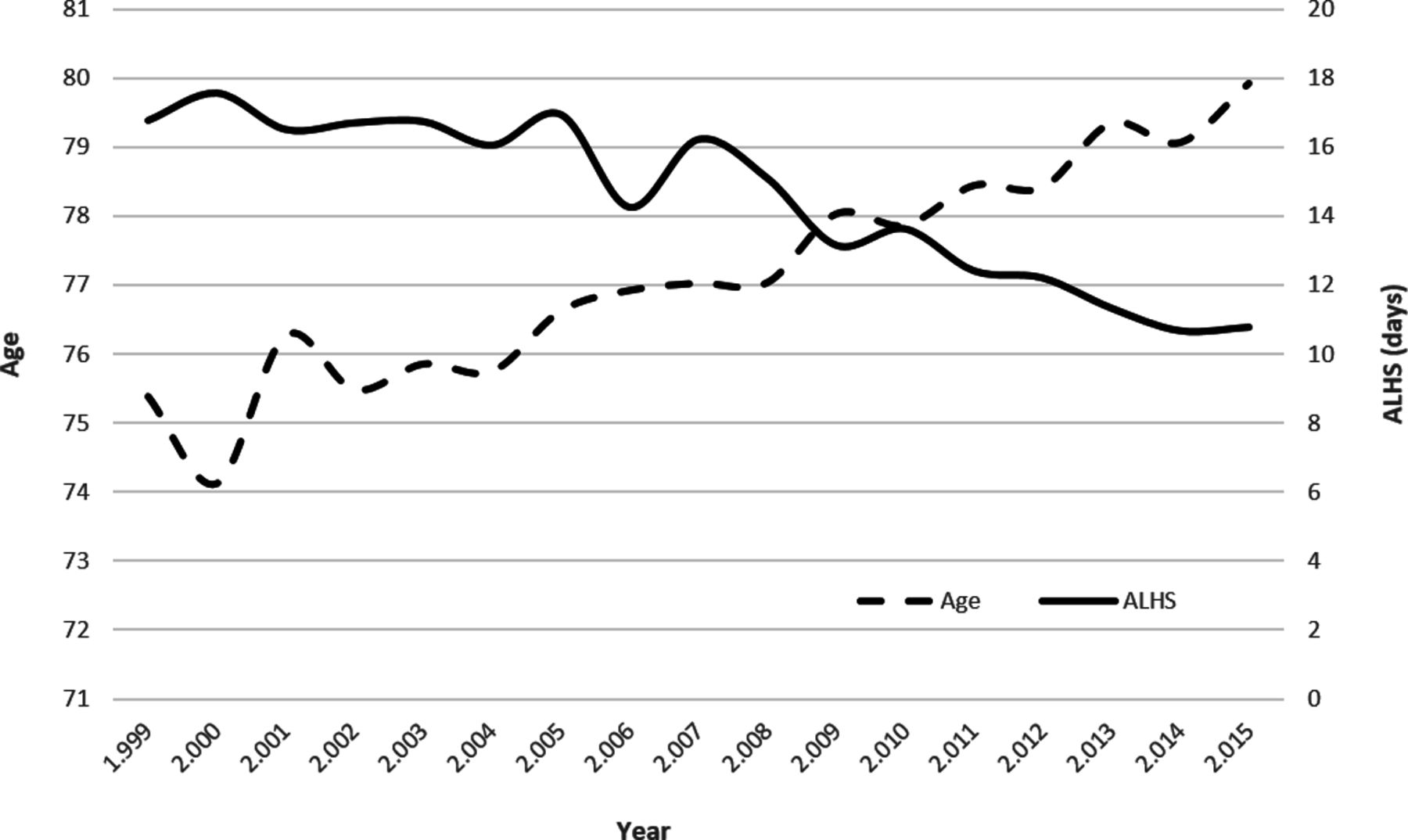
The ALHS significantly decreased (p<0.001) from 16.76 days (SD=15.3 days) in 1999 to 10.78 days (SD=7.72 days) in 2015 (figure 3 and online supplementary table 4). Moreover, age increased (p<0.001) from 75.3 years (SD=9.33) in 1999 to 79.92 years (SD=9.47) in 2015 (figure 3 and online supplementary table 4). The in-hospital CFR was 4.9% (4.4% in women and 7.5% in men, p<0.001). The in-hospital CFR remained stable throughout the study period (online supplementary table 5 and figure 2).
{kind=link}
{kind=link}
{kind=link}
Trend of age and average length of hospital stay (ALHS) during 1999–2015.
Discussion
In the present study, an extended period of time (1999–2015) was analysed. This allowed us to investigate trends in osteoporotic HFs in patients with RA throughout Spain. The main findings of our study are as follows: first, the trend of HF rate in patients with RA in Spain is increasing. This increase is more pronounced in men than in women; second, a different epidemiological pattern is apparent in the incidence of HFs in patients with RA versus the general population, which we discuss below.
In our study, we found an increased incidence of age-adjusted HFs. We estimate an increase of 3.2% per year for both sexes, being more significant in men (3.5%) than in women (3.1%). As far as we know, this is the first study to evaluate the HF rate trend in patients with RA. Several studies have observed a reduction in the use of healthcare resources in patients with RA during different periods of time. This has been found mainly in the number of total joint replacement17–22 and in the number of hospital admissions,23 24 although the relationship vis-à-vis the introduction of T2T and biological treatments is weak.25 The initial hypothesis of our study was to evaluate whether the introduction of new therapeutic strategies in the treatment of patients with RA, such as the T2T, biological therapies and antiosteoporotic drugs (bisphosphonates, denosumab and teriparatide) during the last 20 years has had a favourable impact on the HF rate. Based on our analysis, the answer is no. The only data we found that might indicate a favourable evolution concerns the fact that throughout the study period the average age of patients with HFs significantly increased from a mean age of 75.3 years in the period 1999–2002 up to 79.03 in the period 2010–2015. On the other hand, our results contrast with those of other international26–30 and national studies31 32 that examined general populations. In these studies, a downward trend in the incidence of HF was observed over the last decade. In the general Spanish population, the rate of age-adjusted HF has slowed in recent years, especially in women younger than 75 years.31–33 The most likely explanation as to why we have seen an increase in the incidence of HF during the study period is the increasing life expectancy of ageing patients with RA. In a different analysis of the MBDS, based on a total of 345 000 hospital admissions and 18 000 deaths in RA, we found that the average age of both the patients admitted to the hospital and the age at which they died had increased by about 5 years throughout the study period (data not shown).
Another explanation, closely related to the previous one, is the ageing of the Spanish population. During the study period, the absolute number of people over 85 years of age doubled: in 1999, there were 652 680 people over the age of 85 and in 2015, there were 1327 014.
In other studies, done in our country, such as the national subanalysis of the COMORA study34 35 and the EMAR study,36 we know that the management of osteoporosis seems to have improved over the years, but it remains suboptimal. While in 2002, screening for osteoporosis was infrequent in patients with RA and bone mineral density measurement was performed only in 10.8%36; 12 years later in the COMORA study, bone density was performed in 36.6% of patients younger than 50 years and in 58.6% of those aged 50 years and older.35 On the other hand, we know that in 2002 antiresorptive drugs were infrequently prescribed, and 9.4% of patients in the EMAR study received treatment with bisphosphonates.36 Ten years later, in another study with the same design, EMAR2 study,37 36.2% of patients received treatment with bisphosphonates. In the COMORA study, the prescription of antiresorptive drugs was not analysed, but vitamin D supplementation, however, was more frequent in patients younger than 50 years (93.3%) than in those aged 50 years and above (75%). And only over half of patients (55.2%) were supplemented with vitamin D during prednisone treatment, even in patients at high risk for osteoporosis.35
Another finding of our study is a different epidemiological pattern of HF from that usually found in the general population. First, the age-adjusted HF rates in women are only slightly higher versus those of men. In our study, 85% of HFs were in women versus 15% in men. If we only take into account the absolute number, it might seem that the female to male rate is even greater than in the general population. However, if we take into account the prevalence of RA in Spain,16 which has been estimated at 0.5% and with a female to male ratio of 4:1, we observe that the age-adjusted HF rates are only slightly higher in women versus men, with a 1.23:1 female to male ratio. In Spain, in the general population with HF, the female to male ratio is 3.6:1.31 38 In addition, as the increased incidence of HF was greater in men than in women, the female to male ratio approaches unity, measuring 1.14:1 in 2015. On the other hand, these results suggest that the estimate in the EPISER study16 of a prevalence of RA in men of 0.2% in our country is underestimated. Second, in our study, the incidence of HF rises exponentially in men with ageing, as it does in women, and at the same age as in women (online supplementary figure 1). While in the general population in Spain, the age at which the increase begins is slightly older (∼5–10 years) in men.31 Third and last, in our study we observed that the average age at which the HF occurs is 77.5 years, while in studies conducted in the general population in our country the average is 83.8 years.31 38 Therefore, HFs in patients with RA occur, on average, 6 years earlier than in the general population. It is also important to note that while in the general population the average age at which the HF occurs has remained stable at 83 years, and in patients with RA the average of age has increased from 75.38 years in 1999 to 79.92 years in 2015. This has led to a narrowing of the gap between the general population and patients with RA from 8.2 years in 1999 to only 3.81 years in 2015.
As in studies conducted with the general population, our study shows that men present a higher mortality (7.5% vs 4.4%) and a higher CCI (2.03 vs 1.59) than women.
Our study has both strengths and limitations. The main strength lies in the large sample size over an extended period of time and standardised methodology, which was maintained throughout the study period and that was previously used to investigate HF hospital admissions in Spain.31 32 38 39 We believe that the length of the study period and the exhaustive data provided by the CMBD provide sufficient internal validity, which, in quantitative terms, is seen in the constant frequency of episodes detected every year and, in qualitative terms, in the identification of the age groups at the greatest risk.
We should underscore the limitations of our work. It is an observational study, of retrospective nature, and we cannot therefore establish a causal relationship with the results found. Even if the CMBD provides information from a network of hospitals that covers more than 99% of the population living in Spain,40 some fractures may have escaped the capture area provided by the public hospital discharge registry and there may be coding problems. It is also possible that there are cases of HF in patients with RA in whom RA has not been coded, which would imply an underestimation of our results. Another important limitation is that the Spanish National Hospital Discharge Database (CMBD) does not include any data regarding patient treatments or drug consumption. Another relevant constraint on this paper is the lack of similar studies to analyse trends on the incidence of HF in patients with RA. There are no studies that thereby allow us to compare and discuss our results.
In summary, in Spanish patients with RA we observed an upward trend in the incidence of HF, both in men and in women. We also observed different epidemiological patterns than in the general population: a male to female ratio near unit, an exponential increase with age in both men and women with no age delay in men and an age-at-occurrence that was, on average, 6 years earlier than in the general population. A delay in the age of the fracture and a decrease in the hospital stay were observed. Mortality during admission was stable (about 5%) during the study period.
Acknowledgments
The authors thank the staff of the Research Unit of the Spanish Society of Rheumatology for their support in the editing and translation of the manuscript. To my good friend Caligula who faithfully accompanies me in my research work.
References
Footnotes
Funding This work has a help for the research provided by the Society of Rheumatology of the Community of Madrid (SORCOM).
Competing interests None declared.
Ethics approval Comité Etico del Hospital Universitario Fundación Alcorcón.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent Not required.
Contributors RM and NC-V designed research; EPF, RM, NC-V and JQ-D analysed data. ME, MP,CM-V, JLM-H, CM-P, VV, IMQ, OG-I, CB, MFP, HG, AHV, MGI contributed with the CMBD of their respective hospitals; RM, AG-V and GRC wrote the paper.
Data sharing statement None.