Article Text

Abstract
Immunomodulatory therapy for rheumatoid arthritis (RA) carries risk for infectious complications. Understanding the risks of different therapeutic options is essential for making treatment decisions and appropriately monitoring patients. This review examines data on the risks for serious infections and other key infections of interest for the major classes of agents in use for RA: glucocorticoids, conventional synthetic disease-modifying antirheumatic drugs (DMARDs), biologics and Janus kinase (JAK) inhibitors. Conventional synthetic DMARDs have an excellent safety profile with recent data available supporting the relative safety of methotrexate. Tumour necrosis factor (TNF) inhibitors are associated with an increase in the risk of serious infections. Risk with other biological agents and with JAK inhibitors varies somewhat but overall appears similar to that of TNF inhibitors, with JAK inhibitors also associated with a greater risk of herpes zoster. Glucocorticoids have a dose-dependent effect on serious infection risk—at higher doses risk of infection with glucocorticoids is substantially greater than with other immunomodulatory therapies, and even low-dose therapy carries a risk of infection that appears to be similar to that of biological therapies.
- arthritis
- rheumatoid
- glucocorticoids
- biological therapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Patients with rheumatoid arthritis are at increased risk for infection related to disease activity, comorbidities and immunomodulatory therapy.
Biological therapies are associated with a greater risk for serious infections, although the magnitude of this risk is modest.
Janus kinase inhibitors demonstrate similar risk of serious infections compared with biological disease-modifying antirheumatic drugs but an increased risk of herpes zoster, especially in patients also receiving glucocorticoids.
High-dose glucocorticoids carry the greatest risk for severe infections and opportunistic infections including Pneumocystis jirovecii pneumonia, and low-dose glucocorticoids increase risk for serious infection at a similar magnitude to biologic therapies.
Introduction
Infections are a common, costly and morbid complication for patients with rheumatoid arthritis (RA), with disease activity, multimorbidity and immunosuppressive medications all contributing to infection risk. Given that concerns about infection may influence treatment decisions for providers and patients, and that knowledge of potential risks is important for monitoring and management, a thorough understanding of the risks associated with different medications is important for rheumatologists, infectious disease specialists and generalists caring for patients with RA in the inpatient and outpatient setting.
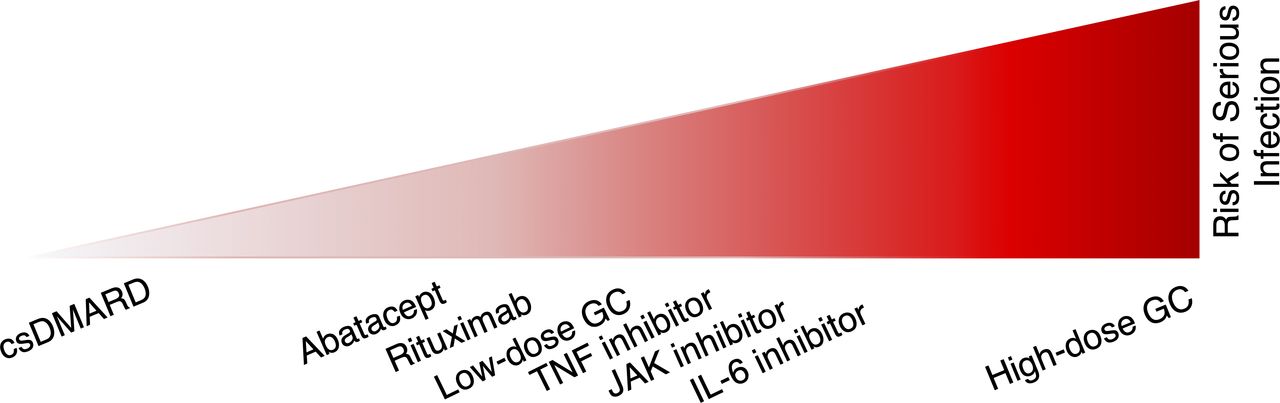
This review will review current evidence on the risk of serious infections as well as other key infections of interest for the major classes of agents in use for RA: glucocorticoids (GC), conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), biological DMARDs and Janus kinase (JAK) inhibitors. Serious infections in the literature can be variably defined, but in more recent trials have been defined as an infection leading to death, requiring hospitalisation or requiring intravenous antibiotics; the data presented in the paper are summarised in figure 1 and table 1.1 Tracking of rare infections has also improved in recent trials including documentation of herpes zoster (HZ), opportunistic infections (OIs) and tuberculosis (TB).2 For other rare conditions such as hepatitis B reactivation or Pneumocystis jirovecii pneumonia (PJP), patient registries and insurance databases become necessary sources of information.3

{kind=link}
Serious infection risk by pharmacological class. Visual depiction of risk of serious infection, with therapies on the right associated with highest risk of serious infection. Differences between various biological therapies and JAK inhibitors are uncertain and likely small. Combination therapy with csDMARDs and biologics appears to have similar risk compared with biological monotherapy. csDMARD, conventional synthetic disease-modifying antirheumatic drug; GC, glucocorticoids; IL, interleukin; JAK, Janus kinase; TNF, tumour necrosis factor.
Summary of serious infection risk and other infectious considerations by pharmacological class
Underlying risk for infection in patients with RA
Prior to a discussion of the infection risk for immunomodulatory therapy, it must be acknowledged that patients with RA appear to be at increased risk for infection compared with the general population, independent of immunomodulatory medications.4 5 Among patients with RA, higher disease activity is associated with greater risk for infection, independent of treatment.6 7 Thus, the potential risks of therapy must be balanced with the benefits of controlling RA disease activity. For many patients, comorbidities and other risk factors for infections may be more important than the risks posed by their RA therapies.
Pharmacological class and serious infection
Conventional synthetic DMARDs
The backbone of current maintenance therapy for RA continues to be csDMARDs, including methotrexate, sulfasalazine, leflunomide and hydroxychloroquine. Hydroxychloroquine and sulfasalazine have perhaps the best safety profile and are not thought to be associated with infection risk.
Recent data have provided information about infection risk with methotrexate. Results from systematic reviews and meta-analyses of observational studies and randomised trials have shown conflicting results; some have found no elevated risk of infection, serious infection or OI, but others have demonstrated a modest increase in risk.8 9 The recently published Cardiovascular Inflammation Reduction Trial enrolled 9300 patients for secondary prevention of cardiovascular disease using 15–20 mg methotrexate compared with placebo and showed no difference in the risk of serious infection (2.2 vs 2.5/100 person-years (pyrs), p=0.5) and a modest increase in general infection risk (16.5 vs 14.4/100 pyrs, p=0.02).10 11 Taken together, this trial and observational data suggest that there may be a small increase in non-serious infections with methotrexate, but minimal increase in the risk of severe infections. The risk of infection with leflunomide is not well described, but a Cochrane review of RCTs for leflunomide demonstrated no significant difference in infection risk between placebo, methotrexate, sulfasalazine or leflunomide.12 Combination therapy with a biologic and csDMARD does not appear to be associated with additional serious infectious risks compared with biological monotherapy.13 14
Biologics
A continually expanding array of biological DMARDs target a variety of cytokines and cell signalling pathways. Despite the differences in the targets of these drugs, they are often grouped in the literature. In a large-pooled network meta-analysis looking at infection risk for all biologics, there was a 1% absolute risk increase for serious infection compared with placebo, but different mechanisms of action lead to different risks.1 This section will focus on the data for the originator biologics approved for RA, as there are limited data on the long-term safety for biosimilar compounds. Although large biosimilar safety studies have not been performed, infection risk with biosimilars is expected to be similar. The following sections will review infection risk with TNF inhibitors (TNFi) and then examine data for other biological therapies.
TNF inhibitors
The most detailed safety data exist for TNFi. A large observational cohort study comparing patients initiating TNFi therapy to those initiating a csDMARD showed an increased risk of serious infection with TNFi (HR of 1.9, 95% CI 1.3 to 2.8), with the highest risk within the first 6 months of therapy initiation.15 A safety review of 49 observational studies found that patients on a TNFi in general had a higher risk of serious infections compared with csDMARDs (HR ranging from 1.1 to 1.8).16 Although no randomised head-to-head studies exist, some observational studies have suggested a higher risk for infection with infliximab compared with other TNFi and a lower risk with etanercept, although these results are not consistent across studies and the potential for confounding remains.17–19
While individual trials are under-powered for safety, meta-analyses of these trials have been done to look at safety data and risks of severe infection. Meta-analyses of the relevant trial data for the individual TNFi for RA have been performed and suggest an HR of 1.31 (95% CI 1.09 to 1.58) for standard-dose biological DMARDs, corresponding to an increase of approximately one serious infection for every 100 patients treated for 1 year.1
Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) fusion proteins
Abatacept is the first generation CTLA-4 fusion protein approved for RA. In a Cochrane meta-analysis of trial data, there was an increase in serious infections seen in patients treated with abatacept compared with control patients (OR 1.91, 95% CI 1.07 to 3.42), but after removing patients co-treated with etanercept the results were no longer statistically significant (OR 1.82, 95% CI 1.00 to 3.32).20 A retrospective cohort study comparing serious infection risk across biologics using Medicare data found the lowest incidence rates with abatacept at 13.1 per 100 pyrs versus 15.9 per 100 pyrs with etanercept (adjusted HR 1.24, 95% CI 1.07 to 1.45) and 17.0/100 pyrs with infliximab (adjusted HR 1.39, 95% CI 1.21 to 1.60).18 Taken together, abatacept may have a favourable risk profile compared with other biologics for serious infectious risk, although differences are likely small.
Interleukin-6 (IL-6) inhibitors
Tocilizumab and sarilumab are potent IL-6 receptor inhibitors. Initial trials were not powered to detect safety but did report cases of severe Epstein-Barr virus reactivation, zoster and limb abscess.21 With initial trials showing elevated LDL cholesterol, a cardiovascular safety trial randomised 3080 patients to tocilizumab or etanercept. While there was no difference in cardiovascular outcomes, there was a significantly higher risk of serious infections with tocilizumab, with 4.5 serious infections/100 pyrs for tocilizumab compared with 3.2/100 pyrs for etanercept (HR 1.39, 95% CI 1.08 to 1.79).22 One observational study from insurance databases showed a small difference in the rate of a composite outcome including serious bacterial infection, diverticulitis, and skin and soft tissue infections in tocilizumab compared with TNFi (HR 1.19, 95% CI 1.07 to 1.33), and showed larger differences compared with abatacept (1.40, 95% CI 1.2 to 1.63).23 A separate observational study showed similar risk of serious infection with tocilizumab compared with TNFi.18 Overall the risk for infection with IL-6 inhibitors seems similar or perhaps slightly greater than the risk with TNFi, although more data are needed to better quantify this risk.
CD20 targeting for B cell depletion
Rituximab is a monoclonal antibody targeting CD20 which leads to B cell depletion. The data regarding the risk of serious infections in rituximab are generally favourable. Pooled analysis of cohort and randomised studies showed no significant differences between rituximab and other treatment groups both in overall infections and in serious infections (4.1% vs 4.6%; OR 1.05; 95% CI 0.84 to 1.31).24 A Cochrane review of eight trials in rituximab in conjunction with methotrexate for RA compared with methotrexate alone showed no significant difference in the risk of all infections (relative risk [RR] 1.1, 95% CI 0.95 to 1.30) or serious infections (RR 0.68, 95% CI 0.42 to 1.10).25 One observational study suggested a higher risk of infection with rituximab compared with other biologics, although this has not been found in other observational studies.18 19 26 27 The risk for serious infection with rituximab does not seem substantially different from other biologics, with some studies even suggesting a risk similar to csDMARDs.
JAK inhibitors
The most recent additions to the armamentarium for RA are JAK inhibitors, including tofacitinib, baricitinib and upadacitinib. As newer agents, less safety data exist; even meta-analyses of existing trials are underpowered to assess serious infection risk, although the rates of infection were overall similar to those seen in trials of other RA therapies (2–3 serious infections/100 pyrs).28 In a head-to-head trial of upadacitinib versus abatacept for RA, there were no significant differences in serious infection (1.0% vs 0.3%) or OIs (1.3% vs 0.3%), although the study was not powered to detect differences in these outcomes.2 A multi-database cohort study using insurance databases including more than 130 000 patients with RA sought to compare the risk of infections with tofacitinib compared with biological DMARDs. The serious infection risk for tofacitinib was similar to TNFi and abatacept.29 Overall, current data support similar risk of serious infection with JAK inhibitors compared with biological DMARDs, although continued safety assessments will be needed over time.
Glucocorticoids
Despite the rapid expansion of effective therapeutics in RA, GC remain a common and important treatment. Although most guidelines recommend limiting use when possible to short-term bridging therapy in patients starting or changing DMARDs, 30%–60% of patients with RA remain on GC long term, although this practice is highly variable among rheumatologists.14 30–32 Risk of infection with GC is dependent on both dose and duration of use, with long-term use of doses >10 mg/day known to be associated with a more than doubling of the risk of serious infections.7 13 14 33 34 Risk of higher doses of GC appears to be substantially greater than that seen with csDMARDs, biologics or JAK inhibitors.
Accumulating data has also suggested that even low-dose therapy ≤5 mg/day is associated with a clinically meaningful increase in serious infection risk. Existing randomised trials of GC are not powered to assess for serious infection risk with low-dose GC, but several different observational studies have found similar risks with low-dose therapy. A case-control study by Dixon et al, modelled recent and prior GC exposure and found a significant risk of infection with long-term doses ≤5 mg/day (HR 1.32, 95% CI 1.06 to 1.63).34 Several observational cohort studies have demonstrated similar associations.6 35 A recent observational study examining patients with RA on stable DMARDs in two large administrative databases found that use of ≤5 mg/day of GC was associated with significant serious infection risk in both cohorts (HR 1.29, 95% CI 1.25 to 1.34 and HR 1.32, 95% CI 1.18 to 1.47), representing approximately 1–2 additional serious infections among 100 patients treated for 1 year—a small but clinically meaningful effect.14 Notably, this infection risk is similar in magnitude to infection risk with TNFi.1 14 GC risks were similar in patients receiving biologics and in patients receiving csDMARDs.14
Herpes zoster
Several studies have demonstrated that the risk of HZ is approximately doubled among patients receiving biological therapies, with no major differences across biological classes.36 Among DMARDs, JAK inhibitors have consistently been found to be associated with the greatest risk for HZ, with risk especially high among patients receiving both JAK inhibitors and GC.28 37 The majority of HZ events are localised with rare disseminated HZ events.38 Studies have also shown that rates of HZ vaccination remain low in patients with RA.36 Now, with the availability of a more effective, recombinant (non-live) vaccine, HZ vaccination should be prioritised in patients with RA, particularly those at greater risk of HZ reactivation.
COVID-19
Determining whether certain medications increase the risk of becoming infected with SARS-CoV-2 and developing COVID-19 has become an area of intense interest. Studying COVID-19 risk is challenging because social distancing behaviours, local COVID-19 activity and testing may all have significant effects on who develops and is diagnosed with COVID-19. Several studies have examined patients diagnosed with COVID-19 to determine whether certain medications are associated with severe disease. Most of the existing studies have not found associations between csDMARDs or biologics and the risk of severe COVID-19.39 40 Some studies have even suggested a reduced risk of hospitalisation in patients receiving TNFi, although residual confounding or selection bias could affect these findings.41 In contrast, several studies have found associations between GC use and severe COVID-19.39–41 These findings might seem initially at odds with the RECOVERY (Randomised Evaluation of COVID-19 Therapy) trial, which showed that dexamethasone reduced mortality in patients with severe COVID-19, but the effects of chronic GC use may be different from short-term use for COVID-19 treatment. Additionally, the RECOVERY trial found trends towards harm with dexamethasone in patients with mild COVID-19, and it is possible that early on in disease, GC could contribute to worsening of COVID-19.42 Similarly, although IL-6 inhibitors and JAK inhibitors are being studied for the treatment of COVID-19, the implications for patients on these therapies chronically are not clear.
Opportunistic infections
Quantifying the frequency of rare OIs beyond serious bacterial infections poses a major challenge in assessing the risk of immunomodulatory agents. Randomised trials are not designed to capture these rare events, though recent trials have made sure to capture and report these events when they occur.2 The best source of data for monitoring for rare events are drug monitoring programmes and patient registries. From the British Society for Rheumatology Biologics Register for RA, they reported 134 total non-TB OIs, at a rate of 134 cases/100 000 pyrs. This registry, and others, have documented rare infections seen infrequently in trials (table 2).3 The following sections will highlight common OIs seen in clinical practice for patients with RA on immunosuppression, namely TB, PJP, hepatitis B and progressive multifocal leukoencephalopathy (PML). The rare infections listed in this review (table 2) have limited data available on incidence and are outside the scope of this review.
List of opportunistic infections observed in patients with rheumatoid arthritis on immunosuppressive therapy
TB reactivation
Patients with latent TB (LTB) can have reactivation of the mycobacteria; some cases of reactivation can be associated with the use of immunosuppression. Importantly, rates of reactivation of LTB are more common in endemic areas; these rates are generally much lower in the USA, Europe and other areas with low prevalence of TB.3 43 Evaluation of registry data has demonstrated an increased risk for TB and TB reactivation for TNFi compared with other biologics though overall incidence rates are low (0.02–0.065 cases of TB/100 pyrs on TNFi).3 43 44 Screening for LTB allows for identification of patient who can be treated with extended-duration antibiotics and prevent reactivations. For patients with RA treated with TNFi, an approach involving the screening and treatment for LTB with a 9-month isoniazid regimen led to a decrease in active TB by 83% and a return of risk to the baseline RA population.43
Pneumocystis jirovecii pneumonia
Data on incidence and prevention of PJP for non-HIV related immunosuppression are best established for solid organ transplant recipients, bone marrow transplant recipients and patients with malignancy undergoing chemotherapy.45 There are limited data for the incidence of PJP in patients with RA. Registry data suggest a higher risk of infections with rituximab compared with TNFi.3 Retrospective data for RA suggest that GC play a significant role in the risk for PJP, which is supported by data from other populations.46 47 There are also limited data on the use of PJP prophylaxis for patients with RA, but both retrospective and prospective cohort analysis support the use of prophylaxis for patients with RA at risk for PJP.46 47 More robust data would be beneficial to support the use of prophylaxis for this patient population.
Hepatitis B
Hepatitis B virus (HBV) is a DNA virus that can cause acute hepatitis as well as chronic hepatitis. Some patients develop latent infections that can reactivate in the setting of immunosuppression and cause fulminant disease. Rituximab appears to have the highest risk; one retrospective study showed that in 50 RA patients at risk for reactivation, four developed HBV reactivation, two of whom developed clinically significant hepatitis and one died as a result of their illness.48 There does not seem to be a significant difference in risk of reactivation with non-rituximab biologics or methotrexate therapy.49 Considering these risks of reactivations, the American Gastroenterology Association (AGA) and the American College of Rheumatology recommend routine screening for patients with RA treated with immunosuppressives.50 51 The AGA has issued guidelines for treatment as well as for prophylaxis for at risk patients. High-risk patients—those who are HBsAg and HBcAb positive treated with high-dose GCs (>20 mg prednisone equivalent dose for 4 weeks or more) or HBcAb positive patients treated with rituximab—are recommended to take antiviral prophylaxis while on treatment and up to at least 6 months after treatment.50
Progressive multifocal leukoencephalopathy
PML is a severe central nervous system infection caused by human polyomavirus 2 (JC virus). PML is classically associated with advanced HIV, and has been reported as a complication of leucocyte adhesion inhibitors used in multiple sclerosis. The British Biologics Registry did not report any cases of PML in patients with RA with over 100 000 pyrs of patient follow-up for patients on biologics.3 Other studies have found rates of PML in patients with RA receiving rituximab of approximately 1–2 per 100 000 patients—higher the background population but lower than rates in patients with chronic lymphocytic leukaemia or non-Hodgkin’s lymphoma treated with rituximab (approximately 10 per 100 000 patients); it is thought that this higher rate of infection is related in part to concomitant chemotherapy.52 Based on this data, the Food and Drug Administration has issued a black box warning related to the risk of PML and rituximab. Given the very rare nature of these events, however, it is generally felt that the benefits of rituximab outweigh these rare risks for patients with RA.
Conclusions
Patients with RA are at increased risk for infection related to disease activity, comorbidities and immunomodulatory therapy. The risk profile of csDMARDs is excellent. Biological therapies are associated with a greater risk for serious infections, although the magnitude of this risk is modest. Some studies suggest that the risk with abatacept may be somewhat less than with other biologics. JAK inhibitors demonstrate similar risk of serious infections compared with TNFi but an increased risk of HZ, especially in patients also receiving GC. Improving HZ vaccination has the potential to mitigate this risk. Among immunomodulatory therapies, higher dose GC carry the greatest risk for severe infections and OIs including PJP. Even low-dose GC therapy seems to be associated with a risk for serious infections with a magnitude similar to that of biological therapies (figure 1, table 1).
Limitations in the current data are related to the rare nature of the events studied. Randomised controlled trials have the lowest risk for bias and confounders, but are often under-powered to detect differences in serious infectious risk or OIs. While large patient registries and health insurance databases can generate sufficient sample sizes to detect differences in serious infection risk or OIs, the risk of confounders limit the strength of recommendations that can be made from this data. The design of safety trials and the application of rigorous multivariate demonstrate paths forward for future research in this field. Continued evaluation of emerging therapies is critical to ensure the safety for patients.
At the same time, these therapies can provide substantial benefit for controlling RA and limiting long-term disability, improving quality of life and also potentially reducing infection risk. It is important to recognise that in many cases comorbidities may contribute more to infection risk than immunomodulatory therapies. Understanding the magnitude of infection risk with different therapies can help clinicians and physicians weigh the risks and benefits of different treatment approaches.
References
Footnotes
Contributors TRR and MDG both were involved in the conception of the review, identification and evaluation of literature, drafting of the manuscript and final approval of the finished manuscript.
Funding MDG is supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases K23-AR073931-01.
Competing interests MDG has previously received research support from Bristol-Myers Squibb for unrelated work.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Not available.