Article Text

Abstract
Introduction Tofacitinib is an oral Janus kinase inhibitor for the treatment of rheumatoid arthritis (RA). Tofacitinib monotherapy was previously shown to inhibit structural damage, reduce clinical signs and symptoms of RA, and improve physical functioning over 24 months in methotrexate (MTX)-naive adult patients with RA. In this post hoc analysis, we compared efficacy and safety of tofacitinib in patients with early (disease duration <1 year) versus established (≥1 year) RA.
Methods MTX-naive patients ≥18 years with active RA received tofacitinib monotherapy (5 or 10 mg two times a day, or MTX monotherapy, in a 24-month Phase 3 trial.
Results Of 956 patients (tofacitinib 5 mg two times a day, n=373; tofacitinib 10 mg two times a day, n=397; MTX, n=186), 54% had early RA. Baseline disease activity and functional disability were similar in both groups; radiographic damage was greater in patients with established RA. At month 24, clinical response rates were significantly greater in patients with early versus established RA in the tofacitinib 5 mg two times a day group. Both tofacitinib doses had greater effects on clinical, functional and radiographic improvements at 1 and 2 years compared with MTX, independent of disease duration. No new safety signals were observed.
Conclusions Treatment response was generally similar in early and established RA; significantly greater improvements were observed at month 24 with tofacitinib 5 mg two times a day in early versus established RA. Tofacitinib 5 and 10 mg two times a day demonstrated greater efficacy versus MTX irrespective of disease duration. No difference in safety profiles was observed between patients with early or established RA.
Trial registration number NCT01039688; Results.
- DMARDs (synthetic)
- Early Rheumatoid Arthritis
- Rheumatoid Arthritis
- Methotrexate
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Previous studies suggest that the early stages of rheumatoid arthritis (RA) may offer a therapeutic window of opportunity during which it may be possible to prevent joint damage.
In methotrexate (MTX)-naive patients with RA, tofacitinib monotherapy is associated with inhibition of structural damage, reductions in clinical signs and symptoms of RA and improvements in physical functioning, over a period of 24 months.
What does this study add?
Tofacitinib 5 mg two times a day appeared more effective in achieving clinical outcomes in early (disease duration <1 year) versus established RA (disease duration ≥1 year).
We observed that compared with MTX, tofacitinib monotherapy (5 or 10 mg two times a day) significantly improved signs and symptoms and physical function, and inhibited the progression of structural damage in MTX-naive patients regardless of disease duration.
How might this impact on clinical practice?
The diagnosis of RA should be made, and treatment started, as early as possible after the development of symptoms.
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disease characterised by synovial inflammation and joint damage that may lead to significant disability.1 The goal of treatment is disease remission or, if remission is unattainable, the lowest disease activity possible, to improve the signs and symptoms, reverse functional disability and halt radiographic progression.2
It has been reported that disease duration has an impact on the effectiveness of treatment, and that comprehensive early treatment may offer an opportunity to preserve physical function and prevent disability.3–6 It has been postulated that the early stages of RA may, therefore, offer a therapeutic window of opportunity in which to prevent joint damage from occurring;7 ,8 it has been suggested that this window may exist from 3 months to 2 years following the onset of symptoms.9 ,10 Much of the evidence for this has been suggested by trials of conventional synthetic disease-modifying antirheumatic drugs (csDMARDs) and tumour necrosis factor inhibitors (TNFi), which have demonstrated that their use in patients with early RA is associated with better outcomes than in patients with established RA.11–14
Tofacitinib is an oral Janus kinase inhibitor for the treatment of RA. The efficacy and safety of tofacitinib 5 and 10 mg two times a day administered as monotherapy or in combination with csDMARDs, mainly methotrexate (MTX), in patients with active RA, has been demonstrated in Phase 215–19 and Phase 320–25 trials of up to 24 months' duration, and in long-term extension studies with up to 84 months of observation.26 ,27
The ORAL Start study (NCT01039688)23 was a 24-month, Phase 3, randomised, double-blind, parallel-group, multicentre study, which compared tofacitinib monotherapy (5 or 10 mg two times a day) with MTX monotherapy in MTX-naive adult patients with RA.23 The results of the primary analysis are reported elsewhere.23 In brief, tofacitinib monotherapy was associated with statistically significant reductions in radiographic progression (measured using van der Heijde modified total Sharp score (vdHmTSS)), reductions in clinical signs and symptoms of RA, and improvements in physical functioning versus MTX monotherapy at month 6, with similar results at months 12 and 24, thus demonstrating durability of response.23 Safety observations were consistent with prior Phase 2 and Phase 3 clinical trials of tofacitinib in patients with RA, and included infections (eg, herpes zoster), gastrointestinal disorders, lymphoma and other malignancies; no new safety signals were identified.23
The objective of this post hoc analysis was to compare the efficacy and safety of tofacitinib monotherapy in MTX-naive patients with early or established RA in the Phase 3 ORAL Start study. For the purposes of this analysis, early RA was defined as disease duration <1 year, and established RA as disease duration ≥1 year from disease diagnosis. These boundaries were chosen to be within the window suggested by the literature, and allowed for an even split of patient data between the two groups.
The ultimate goal of this analysis was to provide insight into the optimal therapeutic window of opportunity during which tofacitinib may be used, thereby improving clinical and radiographic outcomes for patients with RA.
Methods
Study design
This was a 24-month, randomised, Phase 3, double-blind, parallel-group trial conducted in 151 centres worldwide. The full methodology used in this study, with inclusion and exclusion criteria, has been reported elsewhere.23
The study was conducted in accordance with applicable legal and regulatory requirements, as well as the general principles set forth in the International Ethical Guidelines for Biomedical Research Involving Human Subjects, International Conference on Harmonization Guidelines for Good Clinical Practice, and the Declaration of Helsinki. The study protocol and informed consent documentation were approved by the institutional review board or independent ethics committee at each investigational centre. All patients provided written, informed consent.
Patients
Patients were aged ≥18 years, with a diagnosis of RA as defined by American College of Rheumatology (ACR) 1987 criteria,28 and who had ≥3 distinct joint erosions on posteroanterior hand and wrist or foot radiographs (locally read), or a positive test for rheumatoid factor, or antibodies to cyclic citrullinated peptide. Eligible patients also had ≥6 painful or tender joints, ≥6 swollen joints and an erythrocyte sedimentation rate (ESR) >28 mm/hour by Westergren method or high sensitivity C reactive protein (hsCRP) levels >7 mg/L. Patients were excluded if they received >3 weekly doses of MTX, or if ≤3 weekly doses had been received but MTX had been stopped due to an MTX-related adverse event (AE). Patients were randomised in a 2:2:1 ratio to one of three parallel treatment arms: tofacitinib 5 mg two times a day, tofacitinib 10 mg two times a day or MTX weekly. MTX was initiated at a dose of 10 mg/week and, if well tolerated, increased by 5 mg/week every 4 weeks up to 20 mg/week by week 8 for the duration of the study.
We performed a post hoc subgroup analysis using the final 24-month data in patients with early and established RA.
Efficacy of treatment
Effects on signs and symptoms of RA were evaluated using ACR response rates (ACR20, ACR50 and ACR70) and Disease Activity Score in 28 joints (DAS28-4(ESR) <2.6 (remission) and ≤3.2 (low disease activity)). Physical function was assessed using the Health Assessment Questionnaire-Disability Index (HAQ-DI), in which a score <0.5 is considered a normal value, 0.5 to ≤1 mild-to-moderate disability, >1 to ≤2 moderate-to-severe disability and >2 to 3 severe/very severe disability.
Joint structural preservation was assessed using the vdHmTSS29 (range 0–448), with higher scores indicating greater joint structural damage, and an evaluation of the proportion of patients with no radiographic progression, defined as change from baseline in vdHmTSS≤0.5.
In order to assess the sensitivity of findings on the selection of the time points for defining early RA, key efficacy parameters were also calculated for patients with disease duration <6 and ≥6 months.
Safety
The incidence and severity of all AEs was recorded, as previously described.23 The incidence of treatment-emergent AEs (TEAEs), discontinuations due to AEs, AEs of special interest (SIEs), serious AEs (SAEs) and deaths were compared in patients with early and established RA.
Statistical analyses
Unless otherwise stated, efficacy analyses were based on the Full Analysis Set, which included all patients who received at least one dose of study drug and for whom data were available from at least one postbaseline assessment. Binary end points (eg, achievement of ACR20 response) were compared between tofacitinib (5 or 10 mg two times a day) and MTX in a post hoc analysis using the normal approximation to the binomial distribution. Missing values were computed using the non-responder imputation method. Continuous end points, such as change from baseline in HAQ-DI scores, were analysed using a linear mixed-effect model for repeated measures. Treatment, visit, treatment-by-visit interaction and baseline were included as fixed effects, and with patients as a random effect. Estimates of mean changes from baseline for each treatment, as well as mean differences versus MTX were obtained from the model as least squares (LS) means, with corresponding SEs. For vdHmTSS, missing values due to patient discontinuation were linearly extrapolated based on the baseline value and postbaseline value prior to discontinuation. The binary variable of progression/non-progression was obtained from linearly extrapolated imputation data. Observed case data were used in any descriptive analyses. ORs with 95% CI, comparing early versus established disease for each treatment group, were provided for each end point of interest. If the 95% CI did not contain the value 1.0, the difference between the two groups was considered statistically significant at the 5% significance level. No preservation of type I error or multiple-comparisons correction was applied to p values, as statistical significance defined as p<0.05 was exploratory in nature.
Analyses of safety data were based on observed cases. Incidence rates (IRs; unique patients with events per 100 patient-years of observation) for SIEs were based on the number of patients with an event, and the total exposure time censored at time of event, death or discontinuation from the study, and compared between treatment groups. Exact Poisson 95% CIs adjusted for exposure time were calculated for IRs.
Results
Demographics
Baseline patient demographics and disease characteristics are summarised in table 1. Approximately half the 956 patients treated (54% (515/956)) had a disease duration of <1 year; the proportions of patients with RA of duration <1 and ≥1 year were similar between treatment groups (table 1). The majority of patients in the study were women and Caucasian (table 1). Baseline disease activity (DAS28-4(ESR), tender and swollen joint counts) and functional disability (HAQ-DI) in each treatment group were similar in patients with RA duration of <1 and ≥1 year, whereas baseline vdHmTSS and erosion scores, as expected, were higher in patients with longer duration of disease (table 1).
Baseline patient demographics and disease characteristics by disease duration
Clinical responses
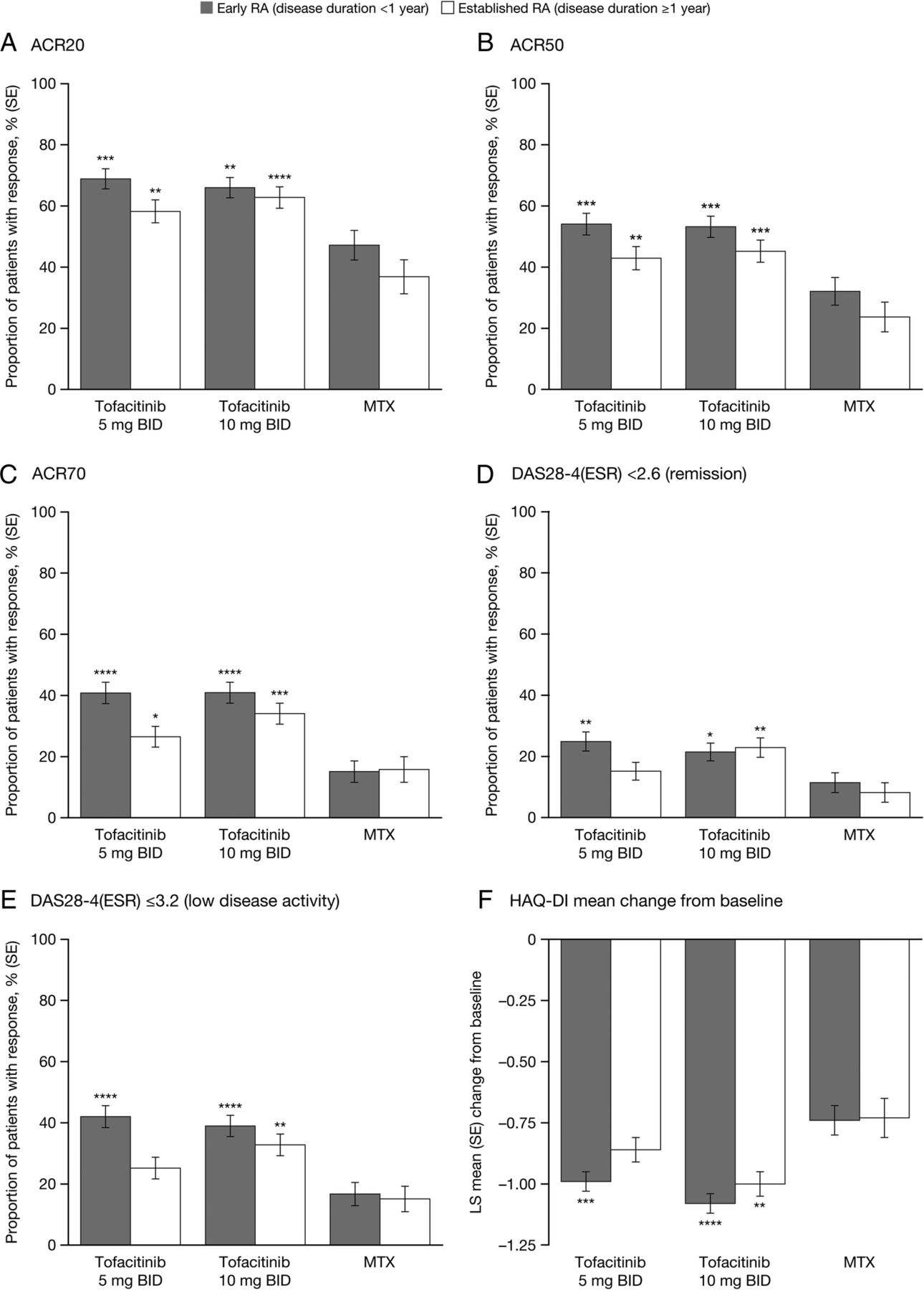
ACR response rates, DAS28-4(ESR) <2.6 and DAS28-4(ESR) ≤3.2 responses at month 24 were generally numerically higher in tofacitinib-treated patients, both 5 and 10 mg two times a day, with early RA versus those with established disease (figure 1). ACR response rates, DAS28-4(ESR) <2.6 and DAS28-4(ESR) ≤3.2 responses were generally statistically significantly higher in patients treated with tofacitinib 5 or 10 mg two times a day compared with MTX, irrespective of disease duration stratification (figure 1). Similar trends in clinical responses were observed at month 12, with higher response rates in tofacitinib-treated patients with early versus established disease, and higher response rates in patients treated with tofacitinib 5 or 10 mg two times a day compared with MTX, irrespective of disease duration stratification (see online supplementary figure S1). Mean DAS28-4(ESR) levels at months 12 and 24 are presented in online supplementary table S1.
Supplemental material
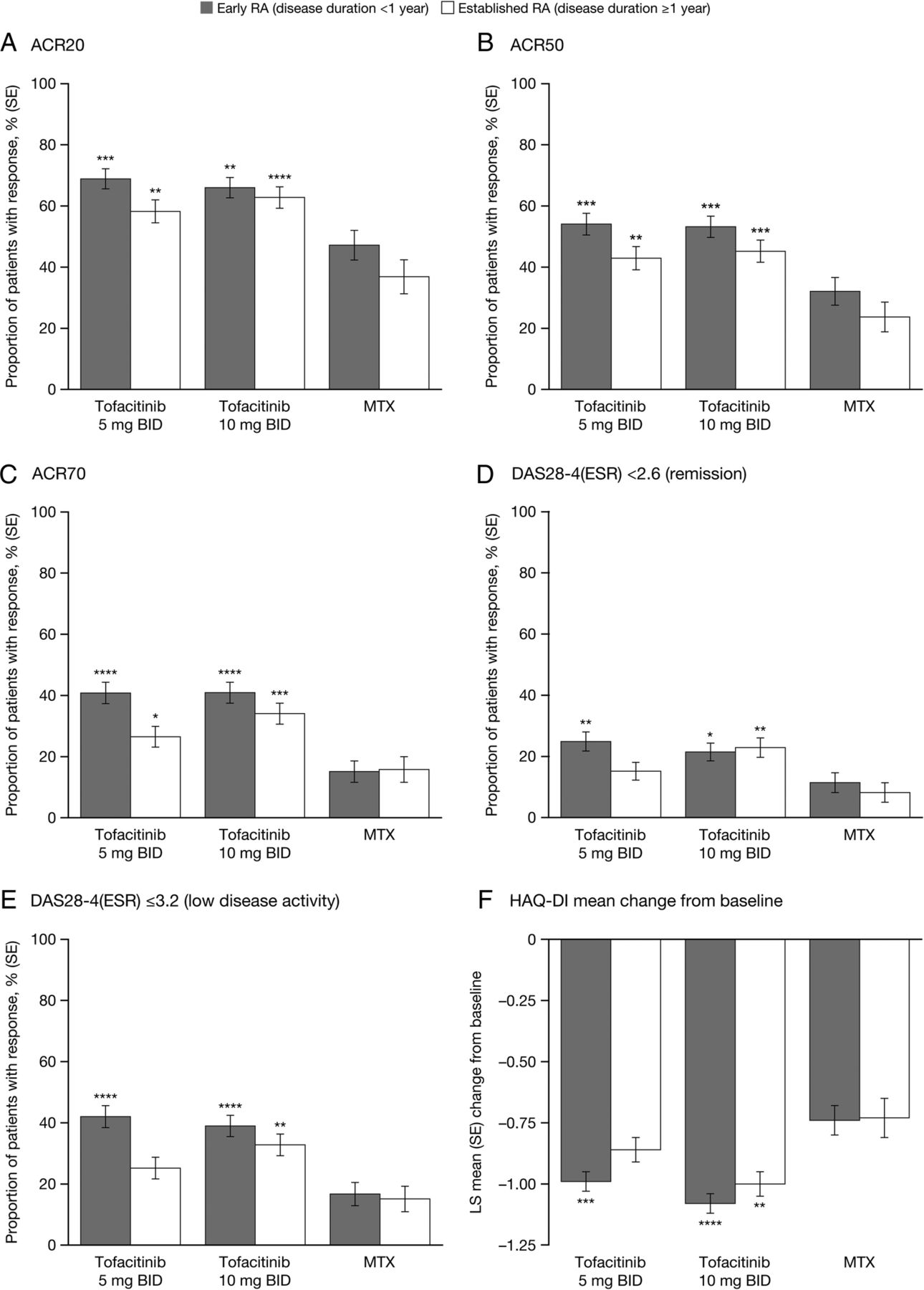
Clinical response in patients with early and established RA at month 24. *p<0.05; **p<0.01; ***p<0.001; ****p<0.0001 vs MTX within disease duration category. Early and established RA are defined as disease duration <1 and ≥1 year, respectively. ACR, American College of Rheumatology response criteria; DAS28-4(ESR), Disease Activity Score in 28 joints, erythrocyte sedimentation rate; HAQ-DI, Health Assessment Questionnaire-Disability Index; LS, least squares; MTX, methotrexate; RA, rheumatoid arthritis.
The mean improvement from baseline in HAQ-DI at month 24 was numerically greater for tofacitinib-treated patients (5 or 10 mg two times a day) with early RA versus those with established disease (figure 1). The mean improvement from baseline in HAQ-DI at month 24 was significantly greater for tofacitinib 10 mg two times a day compared with MTX for both disease duration subgroups, and for tofacitinib 5 mg two times a day for patients with early RA (figure 1). Mean improvements from baseline in HAQ-DI were also numerically greater for patients treated with tofacitinib 5 or 10 mg two times a day in early RA compared with established disease, at month 12 (see online supplementary figure S1). Mean improvement from baseline in HAQ-DI was greater at month 12 for both tofacitinib doses compared with MTX, but achieved statistical significance only for patients with early RA (p<0.001 for both tofacitinib 5 and 10 mg two times a day). Mean HAQ-DI scores at months 12 and 24 are presented in online supplementary table S1.
Radiographic assessments
There was significantly greater inhibition of radiographic progression in patients with early RA who received tofacitinib 5 or 10 mg two times a day compared with MTX at month 24; for patients with established RA, there was numerically greater inhibition of radiographic progression in both tofacitinib groups versus MTX at month 24, but the difference was statistically significant in the 10 mg two times a day group only (figure 2A).Within treatment groups, changes from baseline in vdHmTSS scores at month 24 were similar between patients with early RA and established RA (figure 2A). The proportion of patients with no radiographic progression at month 24 was greater versus MTX in those with early RA who received tofacitinib 5 mg two times a day, and in those with early and established RA who received tofacitinib 10 mg two times a day (figure 2B). Within treatment groups, the proportion of patients with no radiographic progression at month 24 was similar between patients with early RA and patients with established RA (figure 2B). Findings at month 12 were similar (see online supplementary figures S2A, B). Mean vdHmTSS scores at months 12 and 24 are presented in online supplementary table S1.

Radiographic parameters assessed at month 24 in patients with early RA and established RA. *p<0.05; **p<0.01; ***p<0.001; ****p<0.0001 vs MTX within disease duration category. Early and established RA are defined as disease duration <1 and ≥1 year, respectively. The proportion of patients without radiographic progression was determined based on a change in vdHmTSS≤0.5. LS, least squares; MTX, methotrexate; RA, rheumatoid arthritis; vdHmTSS, van der Heijde modification of the total Sharp score.
Treatment differences with tofacitinib versus MTX
Treatment differences (tofacitinib vs MTX) with 95% CIs for all clinical and radiographic assessments at month 24 are shown in figures 1⇑–3. Across all end points, treatment differences versus MTX were generally larger for patients with early RA who received tofacitinib (5 or 10 mg two times a day) than for corresponding patients with established RA, although CIs overlapped (figure 3).

Treatment differences versus MTX in patients with early and established RA at month 24. (A and B) tofacitinib 5 mg two times a day; (C and D) tofacitinib 10 mg two times a day. Early and established RA are defined as disease duration <1 and ≥1 year, respectively. ACR, American College of Rheumatology response criteria; DAS28-4(ESR), Disease Activity Score in 28 joints, erythrocyte sedimentation rate; HAQ-DI, Health Assessment Questionnaire-Disability Index; LS, least squares; MTX, methotrexate; RA, rheumatoid arthritis; vdHmTSS, van der Heijde modification of the total Sharp score.
In patients with early RA, differences in clinical end points with tofacitinib (5 or 10 mg two times a day) were statistically significant versus MTX (all p<0.01, except for DAS28-4(ESR) <2.6 in patients who received tofacitinib 10 mg two times a day, p<0.05). For patients with established RA, statistically significant treatment differences were more frequently observed in the tofacitinib 10 mg two times a day group (all comparisons statistically significant vs MTX at the p<0.05 level), compared with the tofacitinib 5 mg two times a day group (four out of eight comparisons were statistically significant vs MTX at the p<0.05 level). For ACR responses, DAS28-4(ESR) <2.6 and DAS28-4(ESR) ≤3.2, larger treatment differences for tofacitinib 5 mg two times a day versus MTX were observed in patients with early RA versus established RA (figure 3). Corresponding treatment differences at month 12 are presented in online supplementary figure S3.
For patients with early RA, differences in LS mean change from baseline in vdHmTSS, and the proportion of patients without radiographic progression, observed with tofacitinib (5 or 10 mg two times a day) versus MTX at month 24 were significant at the p<0.01 level (figure 3). In patients with established RA, the LS mean change from baseline in vdHmTSS with tofacitinib 10 mg two times a day was significant versus MTX at the p<0.05 level, and the proportion of patients with no radiographic progression was significant versus MTX at the p<0.05 level with tofacitinib 5 and 10 mg two times a day (p=0.0199 and p=0.0039, respectively). Treatment differences for radiographic assessments at month 12 are presented in online supplementary figure S3.
Odds ratios for clinical and radiographic responses in early versus established RA
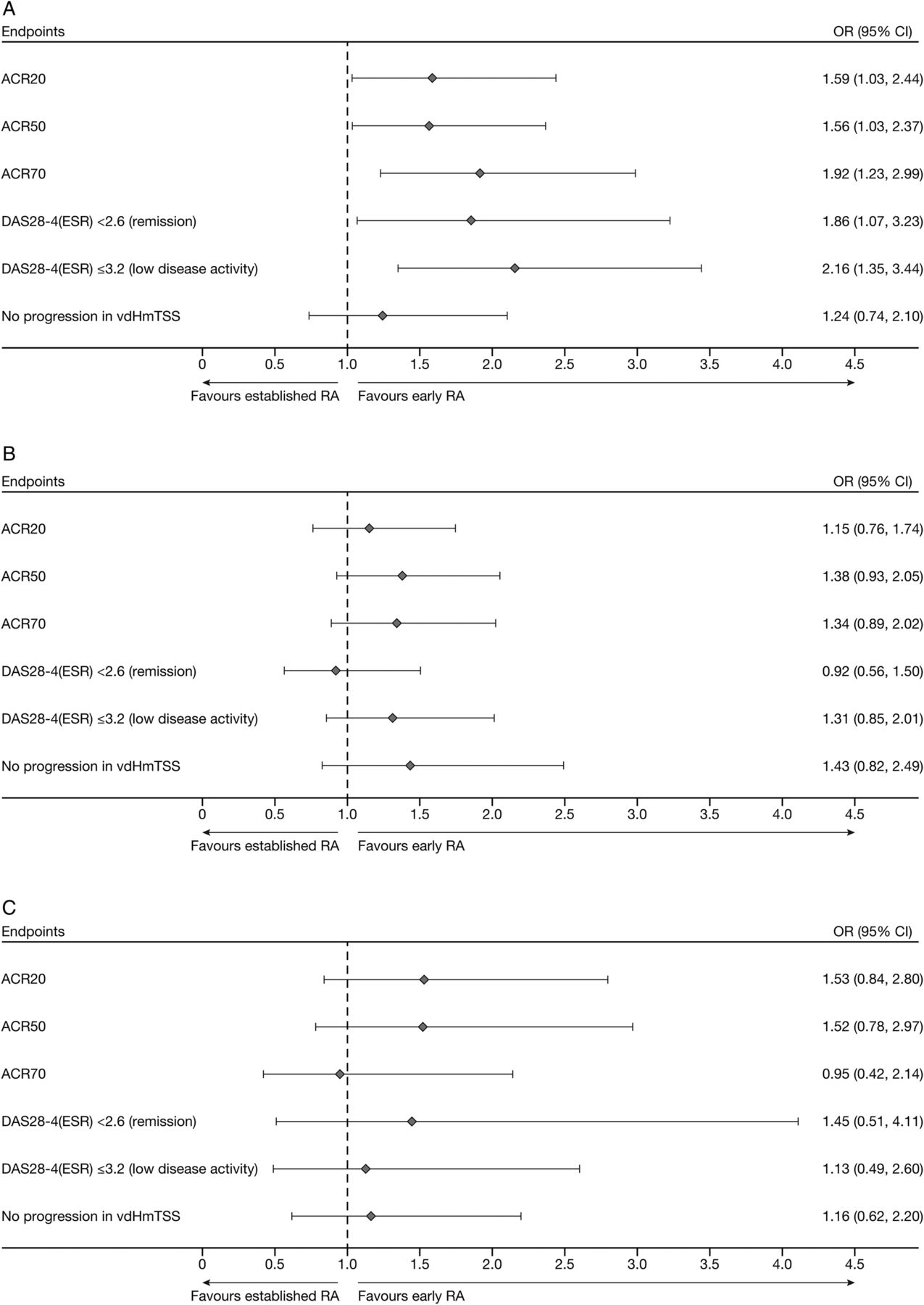
At month 24, patients with early RA had numerically greater odds of achieving ACR20, ACR50, ACR70, DAS28-4(ESR) <2.6, DAS28-4(ESR) ≤3.2 and no radiographic progression compared with those who had established RA, regardless of the study treatment received, with the exception of DAS28-4(ESR) <2.6 for tofacitinib 5 mg two times a day and ACR70 for MTX (figure 4). These differences were significant in patients who received tofacitinib 5 mg two times a day for ACR20, ACR50, ACR70, DAS28-4(ESR) <2.6 and DAS28-4(ESR) ≤3.2 (figure 4A). The corresponding 95% CI of the OR for no progression in vdHmTSS with tofacitinib 5 mg two times a day included 1 (figure 4A). For patients receiving tofacitinib 10 mg two times a day or MTX, 95% CI for ORs included 1.0 for all clinical and radiographic parameters (figure 4B, C). At month 12, similar trends were observed in the tofacitinib 5 mg two times a day treatment group; however, the 95% CI did not include 1.0 for ACR70 and DAS28-4(ESR) <2.6, indicating statistical significance. ORs for clinical and radiographic assessments at month 12 are shown in online supplementary figure S4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Clinical and radiographic end points ORs at month 24 for patients with early and established RA. (A) tofacitinib 5 mg two times a day; (B) tofacitinib 10 mg two times a day; (C) MTX. Early and established RA are defined as disease duration <1 and ≥1 year, respectively. ACR, American College of Rheumatology response criteria; DAS28-4(ESR), Disease Activity Score in 28 joints, erythrocyte sedimentation rate; MTX, methotrexate; RA, rheumatoid arthritis; vdHmTSS, van der Heijde modification of the total Sharp score.
Sensitivity analysis
At month 24, patients with disease duration of <6 months who received tofacitinib (5 or 10 mg) had higher ACR response rates (with the exception of ACR20) and rates of DAS28-4(ESR) <2.6 and DAS28-4(ESR) ≤3.2 than those who had a disease duration of ≥6 months. In addition, ACR response rates, DAS28-4(ESR) <2.6 and DAS28-4(ESR) ≤3.2 responses were higher in patients treated with tofacitinib 5 or 10 mg two times a day compared with MTX, irrespective of disease duration stratification (data not shown).
Safety analysis
A comprehensive analysis of safety data from this study has been reported elsewhere.23 Table 2 presents TEAEs, discontinuations due to AEs, SIEs, SAEs and deaths by disease duration. No meaningful differences were observed between patients with early and established RA with respect to all the safety parameters assessed.
Safety data: number of patients with AEs
Discussion
This post hoc analysis, comparing treatment response in MTX-naive patients receiving tofacitinib 5 or 10 mg two times a day monotherapy or MTX monotherapy, has shown that for signs and symptoms, responses at month 24 were statistically significantly greater in patients with early RA versus established RA for patients receiving tofacitinib 5 mg two times a day. In general, numerically similar clinical and functional responses were observed in patients with early RA compared with patients with established RA for those treated with tofacitinib 10 mg two times a day and MTX. Consistent with the results of the primary analysis of all randomised and treated patients,23 we observed that MTX-naive patients with early or established RA showed significant reductions in the signs and symptoms of RA, improvements in physical functioning and inhibition of radiographic progression when treated with tofacitinib monotherapy (5 or 10 mg two times a day) compared with MTX monotherapy. Additionally, there were no meaningful differences in safety parameters seen between patients with early and established RA.
In subgroup analyses of clinical trials of TNFi therapy in patients with RA, better outcomes have generally been demonstrated in patients with early RA compared with those with established RA.12–14 ,30 In the current post hoc analysis, patients with early RA generally showed similar improvements in clinical and radiographic efficacy end points compared with patients with established RA at baseline; however, there were significant improvements in ACR20/50/70 responses, and DAS remission and low disease activity in patients with early RA versus established RA in the tofacitinib 5 mg two times a day group at month 24, consistent with the data generated in clinical trials of TNFi therapy. Patients who received tofacitinib monotherapy had a statistically greater likelihood of achieving clinical response compared with those who received MTX, whichever tofacitinib dose or disease duration was compared. Baseline mean vdHmTSS and erosion scores were observed to be higher in this study in patients with longer compared with shorter disease duration, as expected, with increased joint damage in established RA that has not been treated effectively.
It has been postulated that there is a window of opportunity during which it may be possible to prevent joint damage with early and aggressive treatment of RA.7 ,9 The American College of Rheumatology now defines early disease as symptoms of <6 months;31 however, it should be noted that definitions of early RA vary across clinical trials from <3 months to <3 years.12 ,14 Furthermore, duration of RA may be challenging to assess in clinical trials, and may not be consistent across trials; time may be determined from onset of symptoms, onset of swelling or fulfilment of other classification criteria.10 Additionally, consideration must be given to the duration of this window of opportunity,32 and when it may close.33
Given the varying disease durations used in defining early RA in other studies, results for key efficacy parameters were reviewed for patients with disease duration <6 months compared with those with disease duration ≥6 months, to assess the sensitivity of the results to the selection of the time points for defining early RA. Although this analysis demonstrated that treatment response at month 24 in patients treated with tofacitinib 5 mg two times a day was higher in patients with shorter disease duration, no significant difference between early and established RA was seen in the tofacitinib 10 mg two times a day or MTX treatment groups. Thus, our post hoc analysis did not provide any definitive support for the concept of a window of opportunity. This study was not designed to address differing responses dependent on disease duration, and further investigation of the effect of tofacitinib in early versus established RA is warranted.
In considering these results in terms of clinical practice, it could be concluded, in line with the principle of treating to target, the best results with tofacitinib or MTX are obtained in patients with early RA. Therefore, the diagnosis of RA should be made, and treatment started, as early as possible after the development of symptoms. If after 3 months of aggressive MTX therapy (ie, at least 20–25 mg/week) an adequate response is not observed, or if MTX is not tolerated, then, if possible, the patient could be switched to tofacitinib monotherapy. If a patient has some response to MTX, but not a significant response, it would be reasonable to add tofacitinib to MTX. An ongoing Phase 4 study will evaluate an add-on versus switch strategy in patients with RA with an inadequate response or intolerance to MTX.34
One potential limitation of this post hoc analysis is that disease duration was defined by the reporting of time since diagnosis at baseline by the investigator, rather than any objective criteria. Diagnosis of RA will vary from clinic to clinic, depending on local practice; the fact that the mean duration of disease for patients in the established RA group was around 6 years, but that these patients were still MTX-naive, highlights the potential uncertainty around disease duration for some patients. A further possible limitation is that this analysis was not prespecified; as such, comparison of tofacitinib effects with those of MTX within disease duration groups was not planned. Also, randomisation into the clinical trial was therefore not stratified by disease duration; the distribution of patients between groups is therefore determined by the decision to use disease duration of <1 and ≥1 year to categorise early versus established RA. However, the results of the sensitivity analysis suggest that the selection of 1 year as a cut-off to define early RA was not critical.
Conclusions
Within treatment groups, improvements in signs and symptoms, physical function and inhibition of progression of structural damage were generally similar between patients with early RA and patients with established RA, although statistically significantly greater improvements in signs and symptoms of disease were observed at month 24 with tofacitinib 5 mg two times a day monotherapy in patients with early RA versus those with established RA.
Tofacitinib 5 and 10 mg two times a day monotherapy significantly improved signs and symptoms and physical function, and inhibited the progression of structural damage, in MTX-naive patients with early or established RA, as compared with MTX monotherapy. No meaningful differences in safety end points were observed between early and established RA subpopulations.
Acknowledgments
Editorial assistance was provided by Claire Cridland of Complete Medical Communications, and statistical support was provided by Ermeg Akylbekova of Quintiles; and both were funded by Pfizer.
References
Footnotes
Contributors RMF, BW, RD and KK planned the study, RMF, AFK, TWJH, RFvV, KK, RD and BW analysed the data, KK performed the analysis and RMF, AFK, TWJH, RFvV, KK, RD and BW contributed to the writing of the manuscript. All authors read and approved the final manuscript.
Funding This study and post hoc analysis were supported by Pfizer.
Competing interests RMF has received research grants and consultancy fees from Pfizer. TWJH reports that the department of rheumatology has mutual projects with a number of EFPIA members (see http://www.BTCURE.com), plus grants from the Dutch arthritis foundation, the Dutch NIH and the EU. This author also reports lecture fees/consultancy fees from Merck, UCB, Bristol-Myers Squibb, Biotest AG, Pfizer, Novartis, Roche, Sanofi-Aventis, Abbott, Crescendo Bioscience, Nycomed, Boehringer, Takeda and Eli Lilly, is a paid instructor for Roche and Pfizer, and is on the Speakers Bureau of Roche, Pfizer, Eli Lilly and Bristol-Myers Squibb. A Kavanaugh has received research support from Pfizer. BW, KK and RD are employees and stockholders of Pfizer. RFvV has received grants and/or research support from Pfizer, Abbvie, BMS, GSK, UCB and has acted as a consultant for Pfizer, Abbvie, BiogenIDEC, Biotest, BMS, Celgene, Crescendo, GSK, Jansen, Lilly, MSD, Pfizer, UCB and Vertex.
Ethics approval The study was approved by the institutional review board or independent ethics committee at each investigational centre.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.