Article Text

Abstract
Objectives Recent studies suggest that implementation of the 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria for rheumatoid arthritis (RA) leads to higher inflammatory activity in seronegative compared with seropositive patients at time of diagnosis. Our aim was to compare the disease course in seronegative and seropositive patients classified according to the 2010 criteria.
Methods DMARD-naïve patients with RA fulfilling the 2010 criteria were included in the treat-to-target ARCTIC trial and followed for 24 months. We stratified patients as seropositive (rheumatoid factor (RF)+, anticitrullinated protein antibodies (ACPA)+ or both) or seronegative (RF– and ACPA–) and compared disease activity, radiographic progression, treatment response and remission rates across groups.
Results 230 patients were included with mean (SD) age 51.4 (13.7) years, and 61% were female. 34 patients (15%) were seronegative. At 24 months, disease activity measures, radiographic progression and remission rates were similar between groups, despite more inflammatory activity in seronegative patients at baseline. Treatment response was slower in seronegative compared with seropositive patients. The groups received similar treatment.
Conclusion Our findings suggest that among patients with RA classified according to the 2010 ACR/EULAR criteria, seronegative patients respond well to modern treatment strategies. However, treatment response was somewhat slower in seronegative patients and radiographic progression was similar in seronegative and seropositive patients. Our results indicate that seronegative RA is not a mild form of the disease and requires intensive treat-to-target therapy similar to treatment of seropositive RA.
- anti-CCP
- early rheumatoid arthritis
- epidemiology
- rheumatoid arthritis
- rheumatoid factor
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Seronegative rheumatoid arthritis (RA) has been considered to represent a less severe disease subset than seropositive RA, with less radiographic damage.
Recent studies indicate that the implementation of the 2010 classification criteria for RA, which put strong emphasis on serological status, leads to higher inflammatory activity in seronegative compared with seropositive patients at time of diagnosis.
What does this study add?
Disease activity, remission rates and radiographic progression were similar in patients with seronegative and seropositive RA after 2 years of follow-up.
Treatment response was slower in seronegative than in seropositive patients, although all patients were treated according to the same algorithm.
How might this impact on clinical practice?
These results indicate that patients now classified as seronegative RA might have a more serious disease than the historic perception of this subgroup and require intensive therapy similar to treatment of seropositive RA.
Introduction
Rheumatoid arthritis (RA) is an autoimmune, potentially disabling joint disease.1 RA is currently classified as seropositive or seronegative based on the presence or absence of rheumatoid factor (RF) and anticitrullinated protein antibodies (ACPA), and serological status has become important in diagnosis, prognostication and treatment decisions. Seronegative RA has been considered to represent a less severe disease subset than seropositive RA, with less radiographic damage.2–6 It has been suggested that seronegative patients should be treated less aggressively than seropositive patients, which is also reflected in the 2016 update of the European League Against Rheumatism (EULAR) treatment recommendations.7 8
Implementation of the 2010 American College of Rheumatology (ACR)/EULAR classification criteria for RA redefined the patient population, including the classification of seronegative patients.9 In our recently published study of disease-modifying antirheumatic drug (DMARD)-naïve patients with early RA fulfilling the new classification criteria, we found that seronegative patients had markedly higher inflammatory activity at the time of diagnosis compared with seropositive patients.10 Based on follow-up data in this cohort, we aimed to examine the disease course of seronegative patients with early RA fulfilling the 2010 ACR/EULAR criteria compared with seropositive patients.
Methods
Patients and study design
Patients with RA fulfilling the 2010 ACR/EULAR classification criteria were included in the ARCTIC trial (ClinicalTrials.gov identifier NCT01205854).11 All patients had symptom duration less than 2 years and were DMARD naïve with indication for DMARD treatment. We stratified the patients as seropositive (RF+ (IgM or IgA), ACPA+ or both) or seronegative (both RF– and ACPA–). Patients were randomised 1:1 to a treat-to-target strategy with or without ultrasound examinations to guide treatment decisions and joint injections during follow-up. The same DMARD escalation algorithm was applied in both arms, and inflamed joints were treated with intra-articular glucocorticoids (triamcinolone hexacetonide). Patients were assessed at 13 visits within 24 months. Data from the two strategy arms were pooled and analysed together for the current study, as clinical and radiographic outcomes were similar in the two strategy arms after 2 years.11 The study was approved by the regional ethics committee, and all patients provided written informed consent.
Data collection
The data collection included demographic data, erythrocyte sedimentation rate (mm/hour), C reactive protein (mg/L), Ritchie Articular Index, 44 swollen joint count (SJC), the patient’s and physician’s global assessment of disease activity on 0–100 mm visual analogue scales, patient-reported outcome measures and radiographs of hands and feet which were scored according to the van der Heijde-modified Sharp score by two independent readers blinded for patient identity and clinical information. The Disease Activity Score (DAS) was calculated.12
Ultrasound examinations were performed by trained rheumatologists according to a validated 0–3 semiquantitative scoring system for grey scale and power Doppler.13 Thirty-two joints were included, giving ranges from 0 to 96 for grey scale and power Doppler.
Sera were collected in a biobank, and RF and ACPA were analysed at the same laboratory by enzyme-linked immunosorbent assay ELISA and fluorescence enzyme immunoassay, respectively. A positive test was defined as any value ≥10 IU/mL for ACPA and ≥25 IU/mL for RF.
Statistical analyses
Continuous variables are presented as means (SD) or medians (25th–75th percentile) according to distribution. Dichotomous variables are presented as frequencies and percentages. At baseline and 24 month follow-up, measures of disease activity were compared across groups using independent samples t-test, Mann-Whitney U test or χ² test as appropriate. We also compared the change from baseline in these measures between groups. Measures of disease activity at baseline and 24-month follow-up were also compared between seronegative patients and subgroups of seropositive patients (single ACPA+, single RF+ and double-positive patients).
Radiographic progression, DAS, SJC44 and ultrasound scores over time were compared between seronegative and seropositive patients by linear mixed-effects models with random intercept for patient in order to account for within-patient dependencies. We used robust variance estimates for ultrasound scores and radiographic progression due to skewed distributions. Finally, we compared response and remission rates across serology status at 3, 6, 12 and 24 months using χ² tests. We also assessed treatment response in logistic regression models with EULAR good/moderate response at 3 and 6 months as dependent variables and serology status (seronegative/seropositive) baseline SJC44, baseline DAS, baseline Ritchie articular index, sex and age as independent variables. We performed the same analyses with ACR 50 response at 3 and 6 months as dependent variables.
Statistical tests were two-sided and p<0.05 were considered statistically significant. Three seronegative and 23 seropositive patients did not attend the 24 month visit, with missing values imputed as described elsewhere.11 Statistical analyses were performed using Stata 14.
Results
Patients
A total of 238 patients were initially included in the ARCTIC trial; of these, 230 attended follow-up visits and were thus included in the current study; 34 patients (15%) were seronegative. In the seronegative/seropositive groups, mean (SD) age was 55.4 (15.7)/50.8 (13.2) years (p=0.07), mean (SD) disease duration was 7.7 (6.8)/7.0 (5.1) months (p=0.46) and 56%/62% were women (p=0.48).
Disease severity
At baseline, measures of disease activity were higher in seronegative compared with seropositive patients.10 Seronegative patients had a significantly greater reduction in disease activity measures (DAS, number of swollen joints, physician global and ultrasonography scores) resulting in no differences between the groups at 24-month follow-up. There was a trend towards more radiographic damage in seronegative compared with seropositive patients, both at baseline and 24 months (table 1).
Measures of disease activity and severity at baseline and 24-month follow-up were also compared between seronegative patients and subgroups of seropositive patients (single ACPA+, single RF+ and double-positive patients). These analyses did not substantially change the results. At baseline, RF positive (ACPA negative) and seronegative (both ACPA and RF negative) patients had similar levels of inflammatory activity, however, the low number of patients in this subgroup makes interpretations difficult (online supplementary table 1).
Supplemental material
Measures of disease activity and severity at baseline and 24-month follow-up compared across serology status
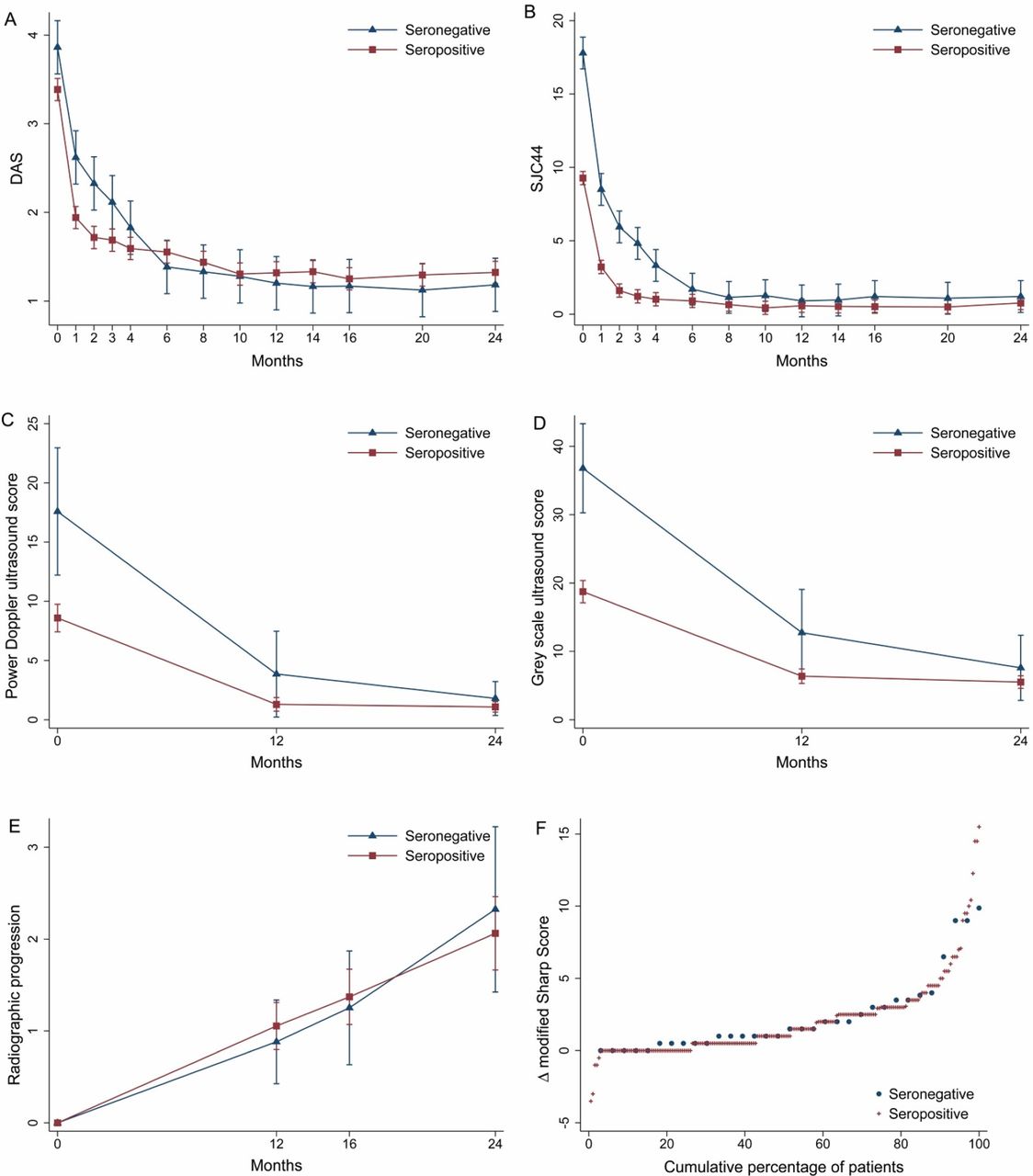
During the first 6 months following DMARD initiation, the number of swollen joints and DAS were higher in seronegative compared with seropositive patients. From month six, they were similar across groups (figure 1A,B). Ultrasound scores were not statistically significantly different between groups after 1 and 2 years (figure 1C,D). Radiographic progression was similar between the groups (figure 1E,F).

{kind=link}
(A–F) Disease activity measures and radiographic progression 0–24 months in seronegative and seropositive patients. (A–E) Margins plot over 24 months of DAS, SJC44, ultrasound power Doppler score, ultrasound grey scale Score and radiographic progression. Bars represent 95% CIs. (F) Cumulative probability plot of change between baseline and 24 months in Van der Heijde modified sharp score. DAS, Disease Activity Score; SJC, swollen joint count.
Response and remission rates
Three months after treatment start, response and remission rates were lower in seronegative patients, and 6% of seronegative patients (2/34) were in ACR/EULAR Boolean remission compared with 30% of seropositive patients (58/196) (p=0.004). From 6 months onwards, response and remission rates were similar between groups. After 6 months of follow-up, 32% of seronegative (11/34) and 35% of seropositive patients (69/196) were in ACR/EULAR Boolean remission (p=0.75) (table 2). Analyses adjusted for age, gender, baseline DAS, baseline SJC44 and baseline Ritchie articular index showed that seropositivity was associated with achieving treatment response at 3 months, both for ACR 50 response (OR 3.8 (1.5 to 9.8)) and EULAR good/moderate response (OR 3.9 (1.4 11.2)). Serology status did not predict treatment response at 6 months. Higher baseline DAS was associated with treatment response at 6 months, but not at 3 months (data not shown).
Treatment response at 3 and 6 months and remission rates at 3, 6, 12 and 24 months
Treatment
Treatment was similar across groups during the study, with similar rates of seronegative and seropositive patients receiving methotrexate monotherapy, triple therapy and biological treatment at 6 months and 24 months (data not shown). There was a trend towards a higher rate of biological treatment in seronegative patients at the 6 month visit, as 11.8% of the seronegative patients (4/34) received biological treatment, compared with 5.1% of the seropositive patients (10/196, p=0.13).
Discussion
In this follow-up study of patients with early RA classified according to the 2010 ACR/EULAR criteria, disease activity after 2 years of treat-to-target therapy was similar in seronegative and seropositive patients, despite markedly more inflammatory activity and a tendency towards more radiographic damage in seronegative patients at baseline. Treatment response was somewhat slower in seronegative patients and radiographic progression was similar in seronegative and seropositive patients. Our findings suggest that in patients RA classified according to the new criteria, seronegative RA is not a mild form of the disease and requires intensive treat-to-target therapy similar to treatment of seropositive RA.
Several studies of patients classified according to the 1987 criteria for RA indicate that seronegative patients have a less severe disease course with less radiographic damage than seropositive patients.2–6 14 Studies have also shown more inflammatory activity in seropositive patients, with fewer patients achieving remission,4 14 15 although evidence is somewhat conflicting.6 16 17 There is very limited information about the disease course of seronegative patients classified according to the 2010 criteria. One recently published study in patients with RA fulfilling the 2010 criteria showed that patient-reported outcomes including physical functioning and restrictions at work were similar in ACPA-positive and ACPA-negative patients after 4 years of follow-up.18 This is in line with our study where seronegative patients did not have a less severe disease course than seropositive patients, with similar rates of remission and similar radiographic progression over 2 years. In our study, there was a trend towards more radiographic damage in seronegative compared with seropositive patients, both at baseline and 24 months. The numerical differences may not have reached statistical significance due to the small number of patients in the seronegative group.
An aim for the ACR/EULAR 2010 RA classification criteria was to increase sensitivity for patients with early disease. However, the low number of seronegative patients included in the ARCTIC trial and, on average, high inflammatory activity in seronegative patients at baseline, indicate that the increased sensitivity may be confined to patients with seropositive disease.19
When patients were included in the ARCTIC trial, the ACR/EULAR 2010 classification criteria for RA were used. At this time, the erosion criteria had not yet been defined, and patients who did not otherwise fulfil the criteria may have been included if we had applied the later published erosion criteria.20 However, a recently published study has shown that the clinical and radiographic course in ACR/EULAR 2010 negative patients under treatment was not dependent on the presence of erosions at diagnosis.21
Studies have shown that patients who do not respond significantly to treatment within 3 months have a low chance of attaining remission within 6 months.22 23 According to the current EULAR recommendations for management of RA, treatment adjustment should be considered in patients with less than 50% improvement in disease activity 3 months after treatment start.8 In our study, the treatment response at 3 months was better in seropositive than seronegative patients, whereas the number of patients in remission at the end of the study was similar across groups. This observation may indicate that seronegative patients might respond well to treat-to-target strategies even if the initial treatment response is delayed compared with seropositive patients.
Seronegative RA has been considered to represent a less severe disease subset than seropositive RA.2–6 This assumption could possibly lead to less intensive treatment of seronegative patients in usual care. Our results highlight that both patients with seronegative and seropositive RA should receive intensive treat-to-target DMARD therapy. The updated EULAR treatment recommendations are more or less the same as the treatment protocol in the ARCTIC trial, increasing the generalisability of our results.
A limitation of our study is the small number of seronegative patients included, which limits the statistical power. Strengths of our study include the extensive data collection with radiographic and ultrasonographic examinations of all patients. To our knowledge, this is the first study to examine the disease course of seronegative RA in an inception cohort of DMARD-naïve patients classified according to the 2010 ACR/EULAR criteria.
In conclusion, patients with seronegative RA classified according to the 2010 ACR/EULAR criteria respond well to modern treatment strategies, but seronegative RA is not a mild form of the disease and requires as intensive treat-to-target therapy as seropositive RA.
Acknowledgments
The authors wish to thank the patients for participating in this study and the ARCTIC investigators: Hallvard Fremstad, Tor Magne Madland, Åse Stavland Lexberg, Hilde Haukeland, Erik Rødevand, Christian Høili, Hilde Stray, Anne Lindter Noraas, Dag Magnar Soldal, Gunnstein Bakland.
References
Footnotes
Presented at Some of the findings in this article were presented as a poster presentation at the EULAR and ACR 2017 annual meetings.
Contributors All authors were involved in drafting the article or revising it critically for important intellectual content and approved the final manuscript to be submitted and agreed to be accountable for all aspects of the work. Conception and design of the study: EAH, SL, LBN, A-BA, EL, ICO, HBH, TU, DvdH, JS and TKK. Acquisition of data: EAH, A-BA, HBH, TU and the ARCTIC investigators. Analysis and interpretation of data: LBN, ICO, JS, EAH, SL, EL, A-BA, DvdH and TKK.
Funding The study has received grants from the Norwegian Research Council, the South-East Health Region in Norway, The Norwegian Rheumatism Association and unrestricted grant support from AbbVie, Pfizer, MSD, Roche and UCB.
Competing interests EAH has received research funding from Pfizer, UCB, Roche, MSD and AbbVie for the submitted work, honorariums as a speaker from Pfizer, UCB, Roche and AbbVie and honorariums for development of educational material from Pfizer and Eli Lilly and has sat on advisory boards for Pfizer, Eli Lilly, Celgene and Janssen-Cilag. A-BA has sat on advisory boards for UCB, AbbVie and Pfizer and received honorariums for development of educational material for UCB. HBH has received honorariums as a speaker from AbbVie, Bristol-Myers Squibb, Roche, UCB Pharma, Novartis and Pfizer. DvdH has received consultancy honorariums from AbbVie, Amgen, Astellas, AstraZeneca, Bristol-Myers Squibb, Celgene, Daiichi, Eli Lilly, Galapagos, Merck, Novartis, Pfizer, Roche, Sanofi Aventis, Janssen and UCB and is owner of Imaging Rheumatology. TKK has received consultancy honorariums from AbbVie, Bristol-Myers Squibb, Celltrion, Epirus, Hospira, Merck-Serono, MSD, Orion Pharma, Pfizer, Roche and UCB. TU has received honorariums as a speaker from AbbVie, Bristol-Myers Squibb, Lilly, Roche, Novartis, UCB Pharma and Pfizer. ICO has received consultancy honorarium from Pfizer.
Patient consent Not required.
Ethics approval The Norwegian Regional ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors commit to making the relevant anonymised patient level data available on reasonable request.