Article Text

Statistics from Altmetric.com
The benefit of rituximab (RTX) in interstitial lung disease (ILD) associated with connective tissue disorders (CTD) has been suggested.1–4 Moreover, preliminary data highlighted that B cell (BC) depletion measured 2 weeks after the first RTX infusion could be predictive of treatment response at 6 months in systemic sclerosis (SSc)-ILD.5 This raises the question of whether sustained BC depletion is associated with a longer-term response. Our aim was to determine whether BC depletion was associated with long-term response to RTX in CTD-ILD.
We conducted a retrospective monocentric study including all patients treated at least 1 year with RTX for CTD-ILD. The primary outcome was the absolute change from baseline of forced vital capacity (FVC) (L) at 12 months and at the last RTX infusion according to complete or incomplete BC depletion. The secondary outcomes were (1) the percentage of patients with any FVC benefit at 12 months and at the last RTX infusion; and (2) the change in carbon monoxide diffusion capacity (DLCO) at the same time points.
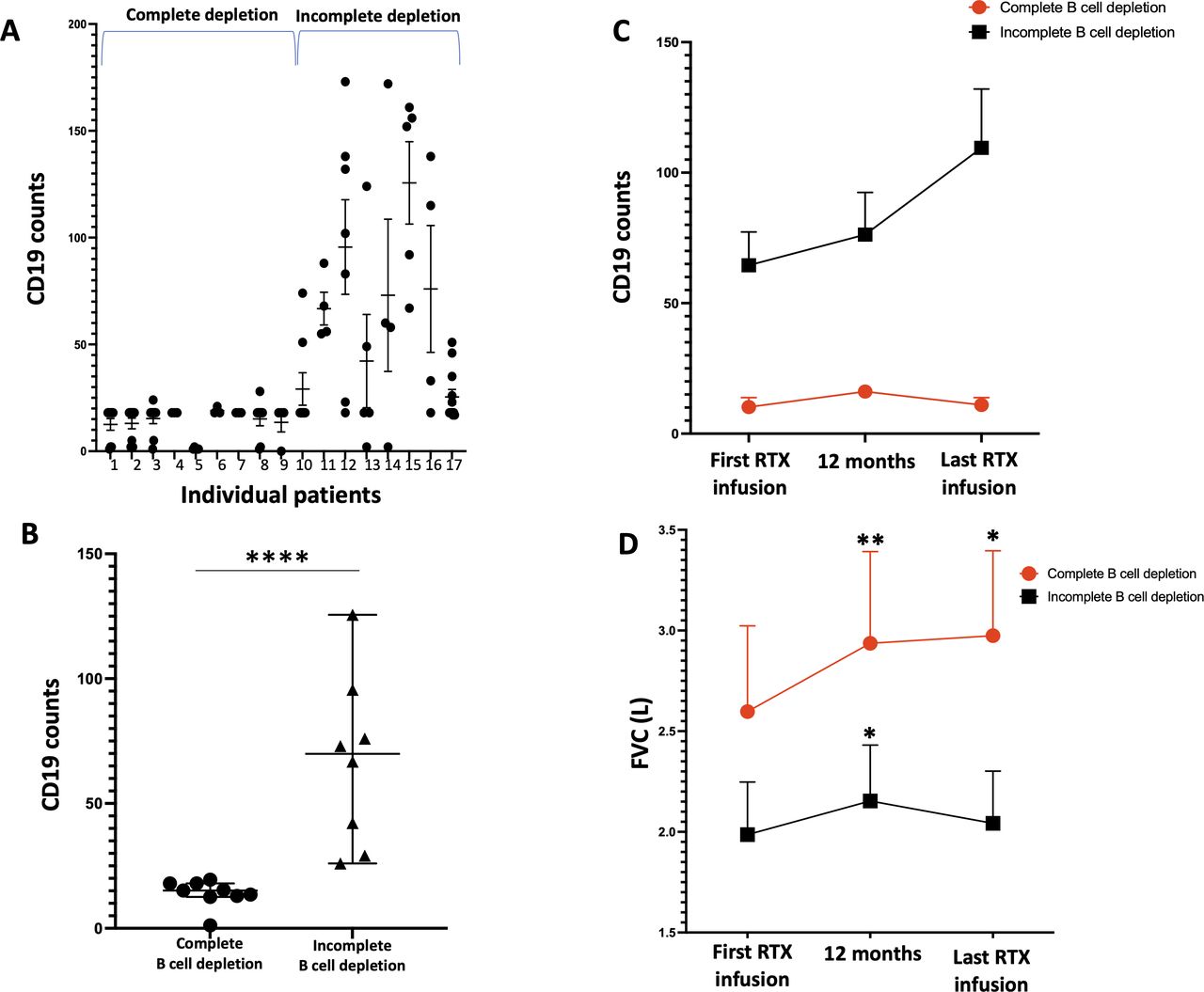
Overall, 17 patients (12 SSc, 5 with Mixed Connective Tissue Disease-MCTD) were included. The median age was 59 years (95% CI 48 to 63) and the median duration of CTD was 8 years (95% CI 5 to 11) (online supplemental table S1). The median duration of RTX exposure was 45 months (95% CI 19 to 90), the median number of infusions was eight per patient (95% CI 5 to 14) and the cumulative RTX dose was 7 g (95% CI 5 to 14). We identified nine patients with sustained complete BC depletion (median CD19 during the observation period: 15 per microlitre, 95% CI 14 to 18) and eight patients with incomplete BC depletion (median CD19 during the observation period: 70 per microlitre, 95% CI 18 to 126) (figure 1A,B and online supplemental table S2).
Supplemental material
{kind=link}
(A) Individual CD19 counts measured prior to each RTX infusion. (B) Comparison of CD19 counts between patients with or without complete B cell depletion. Each point represents the median CD19 value measured at each infusion per patient during the observation period (at least three measures per patient). Data are shown as median and 95% CI; ****p<0.0001 by Mann-Whitney test. (C) Course of CD19 during the observation period according to B cell depletion. (D) Course of FVC during the observation period according to B cell depletion; *p<0.05 and **p<0.01 versus baseline value by the Wilcoxon matched-pairs signed-rank test. FVC, forced vital capacity; RTX, rituximab.
In the whole population, the median FVC increased from 2.38 L (95% CI 1.38 to 3.10) to 2.64 L (95% CI 1.64 to 3.85) at 12 months (p<0.001) after the first infusion and decreased to 2.51 L (95% CI 1.6 to 3.22) at the last RTX infusion (p=0.008).
In the subset of patients with sustained complete BC depletion, the median FVC increased from 2.58 L (95% CI 1.13 to 4.08) to 3.08 L (95% CI 1.34 to 4.64) at 12 months (p=0.004), then to 3.22 L (95% CI 1.57 to 4.19) at the last RTX infusion (p=0.019) (figure 1D and online supplemental figure S1). Conversely, in the subset of patients with incomplete BC depletion, FVC initially increased from 2.04 L (95% CI 0.99 to 3.24) to 2.23 L (95% CI 0.83 to 3.35) at 12 months (p=0.039), before decreasing to 1.89 L (95% CI 1.00 to 3.24) at the last RTX infusion (p=0.37) (figure 1C and online supplemental figure S1). The percentage of patients with any FVC improvement was higher in the subset of patients who maintained complete BC depletion at 1 year (6 out of 9 (67%) vs 4 out of 8 (50%)) and at the last RTX infusion (8 out of 9 (89%) vs 4 out of 8 (50%)). Conversely, the median DLCO did not significantly differ according to BC depletion (online supplemental material).
Supplemental material
These results extend those obtained at short term in SSc-ILD5 and are consistent with the findings reported in rheumatoid arthritis, in which the persistence of BC in the circulation following RTX was associated with poor prognosis.6 Although prediction of progression is not fully understood in patients with SSc and MCTD, and particularly the predictive value of baseline FVC in further progression remains to be established, we acknowledge that the differences in baseline FVC may have influenced the outcomes in our sample of patients with CTD-ILD.7
Our study had a long-term follow-up and a standardised therapeutic regimen, but was limited by its small sample size and the DLCO measurement feasible only in 13 patients. This low number of patients, together with the fact that many factors related or beyond CTD-ILD may affect DLCO, may explain the absence of a significant modification of this parameter according to BC depletion. Due to the small sample size of our patient population and the heterogeneity in both patients with SSc and those with MCTD, the generalisation of the findings to patient populations of CTD may be limited.
Our results support the careful monitoring of circulating BC in daily practice with the objective of reaching and maintaining complete BC depletion in order to get the most from RTX in CTD-ILD.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
OAT, RG, JA and YA contributed equally.
Presented at Presented at ACR 2022, Abstract Number 1527: Maintained Complete B Cell Depletion Is Associated With Rituximab Efficacy in Connective Tissue Disorder Interstitial Lung Disease (https://acrabstracts.org/abstract/maintained-complete-b-cell-depletion-is-associated-with-rituximab-efficacy-in-connective-tissue-disorder-interstitial-lung-disease/).
Contributors OAT, RG, AC, AS and MT collected the data. OAT and JA performed the statistics. OAT, RG and JA wrote the manuscript. YA directed the work and reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.