Article Text

Abstract
Hepatitis C virus (HCV) is a global pathogen and is the cause of rare but complex rheumatic complications but more commonly exists as a challenging comorbidity for patients with existing rheumatic diseases. Until recently, the standard of care of HCV has been the use of interferon-based regimens, which not only have limited effectiveness in curing the underlying viral illness but are poorly tolerated and in patients with rheumatic diseases especially problematic given their association with a wide variety of autoimmune toxicities. Numerous and other more effective and better tolerated regimens are rapidly emerging incorporating direct acting antiviral agents that do not require the use of interferon, that is, interferon free. The potential of interferon free treatment of HCV makes screening for this comorbidity more important than ever. Rheumatologists need to be knowledgeable about these therapeutic advances and partner with hepatologists to craft the most efficacious and toxicity-free regimes possible.
- Infections
- Autoimmunity
- Treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Hepatitis C virus (HCV) is a global pathogen infecting nearly 200 million people and a major cause of morbidity and mortality. HCV now outpaces HIV infection, in the USA, as a cause of annual death.1 For rheumatologists, HCV infection is also a well-known cause of relatively rare rheumatic diseases, most notably cryoglobulinemic vasculitis, among others.2 ,3 Far more commonly, HCV is a complex comorbid condition in patients with rheumatic diseases that serves as a cause of significant concern and complexity to rheumatologists and hepatologists alike when they attempt to craft therapies to manage the underlying rheumatological disorder as well as the underlying HCV infection.4 A major reason for this conundrum has been the requirement of using α interferon, which has well known and severe side effects including the development of de novo, or the exacerbation of, underlying autoimmune disease. This problem is about to end as we witness one of the greatest advances in modern medicine, namely the prospects for curing HCV infection with short, well-tolerated oral regimes that are effective nearly 100% of the time; curing HCV infection will soon be totally devoid of the need to use interferon. This revolution is of particular relevance to rheumatologists and this commentary is designed to provide a brief background of this remarkable advance and guidance for approaching HCV in our practice.
The story of interferon therapy and, indeed, the common attitude towards interferon therapy for HCV, is one of resigned trepidation and deep concern. Introduced in the early 1980s as a mono therapy, it was found to be poorly tolerated and poorly effective with virological cure (sustained virological response or SVR) observed in about 6% of patients. Over time with different dosing regimens and pegylated formulations optimising its pharmacokinetics and then ultimately combining it with an oral immunomodulator ribavirin for up to 48 weeks or longer, SVR rates increased to about 50% in highly selected patients eligible for clinical trials.5 Unfortunately, the adverse effect profile was unchanged and actually exacerbated by ribavirin, which causes anaemia that at times can be severe. Tragically, the most common interferon side effects such as fever, fatigue, arthralgia, myalgia and depression have been of particular concern in rheumatology patients where differentiation of drug side effect from underlying disease was often impossible.6 ,7 The development of frank autoimmune diseases such as systemic lupus erythaematosus, rheumatoid arthritis, sarcoidosis, autoimmune thyroid disease and others has been reported in a small per cent with its use as well.6 ,8 As a result, many patients with coexisting HCV and inflammatory rheumatic diseases often had their rheumatological condition undertreated based on fears of exacerbating underlying liver disease. This practice has been encouraged by published treatment guidelines limiting aggressive use of most biological and non-biological disease-modifying antirheumatic drugs (DMARDs)9 or immunosuppressive therapies in patients with HCV infection. Similarly, while autoimmune disease is not an absolute contraindication for interferon therapy per se, liver specialists have often considered patients with rheumatic disease with HCV infection suboptimal treatment candidates based on concerns of exacerbating the underlying autoimmune disorder with interferon. Thus the patient with HCV infection with rheumatic disease has often been underserved by both specialty communities.
Even for patients with HCV-associated cryoglobulinemia, where interferon-based therapies have proven successful, the use of these agents has not been without difficulty.10 The presence of membranous glomerulonephritis was a negative predictive factor to a good response.11 The safety profile of this interferon-based combination was not good. On one hand, interferon has been reported to worsen peripheral neuropathy12 or skin ulcers,13 while it was frequently inducing fatigue and depression, limiting its use. On the other hand, ribavirin frequently induced a dose-dependent anaemia conducting to dose decrease than less frequent SVR.5
The beginning of the new era came relatively recently with the development of the first two ‘direct acting’ antiviral agents, that is, boceprevir and telaprevir.14 In combination with pegylated interferon and ribavirin, these first generation HCV protease inhibitors significantly improved outcomes in patients infected by HCV genotype 1 but worsened toxicity, thus limiting their use in general as well as in patients with rheumatic diseases.15 Today, however, we are squarely in a phase of tectonic change as multiple oral direct acting agents are either approved, imminently to be approved or in advanced stages of trials14 announcing the end of interferon therapy, ensuring that conditions will never be the same. The same principles, so successfully applied to the treatment of HIV infection, are now being applied with even greater success in the treatment of HCV infection including the use of multiple agents directed at multiple targets to maximise efficacy and limit resistance.
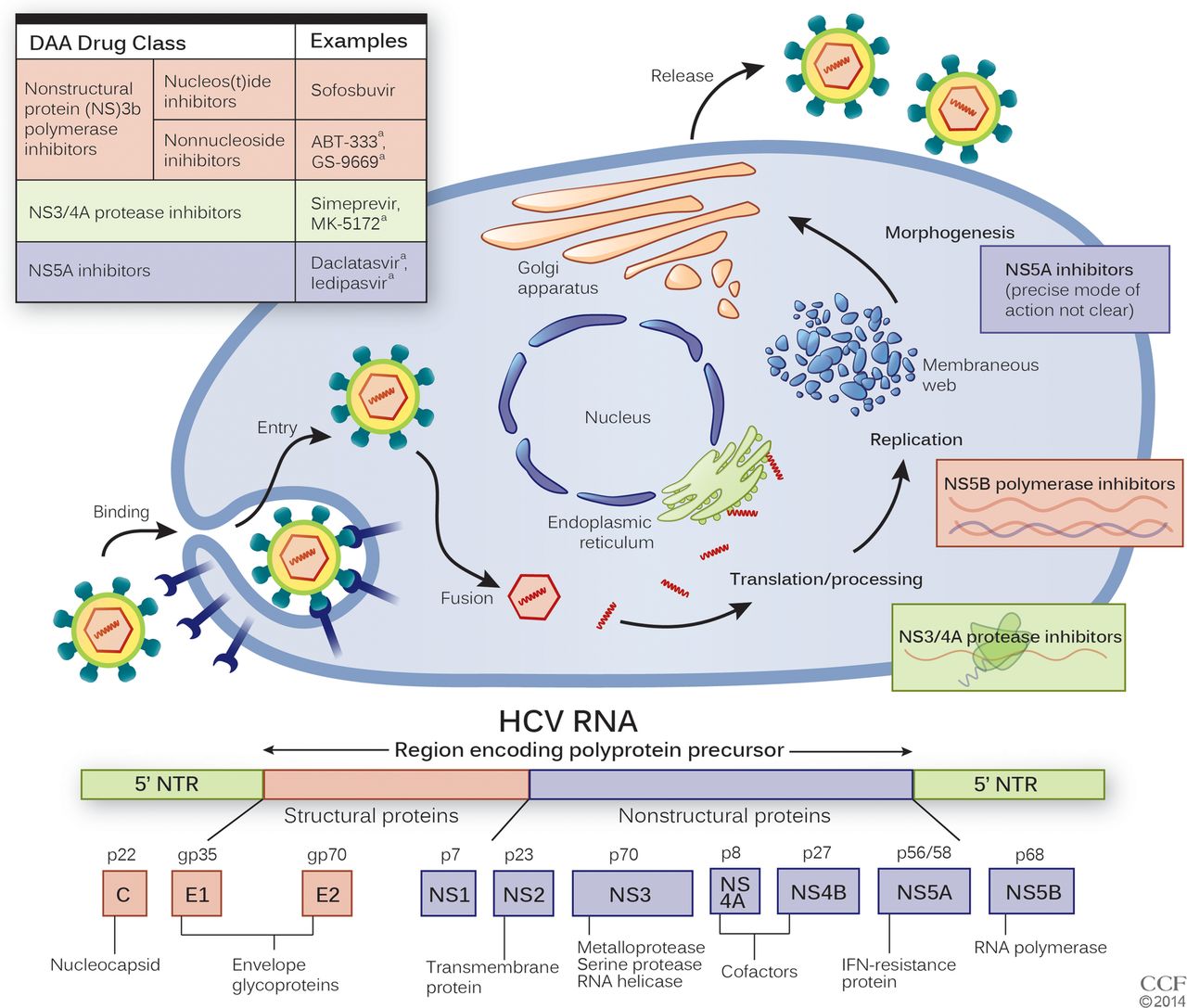
A basic understanding of these agents can be appreciated from figure 1, which describes only a few of the agents either approved or in advanced stages of trials demonstrating their selected sites of viral targeting.16 Since HCV, unlike HIV, is not a retrovirus, it has no proviral form and is not incorporated into the host genome. Thus when HCV is successfully treated (ie, SVR) it can be essentially cured. The new interferon free regimens, and ribavirin free regimen as well, have minimal toxicity and minimal side effects, and have reported cure rates of 93–100% in all HCV genotypes even in the presence of some traditional markers of poor treatment efficacy.17 In addition, they are all oral and used for a brief duration (some protocols as brief as 6 weeks18). While these treatments are highly expensive, these oral agents now offer a new hope for patients with rheumatic diseases who have been unable to take standard interferon-based therapies in the past.19 Professional societies are now challenged to publish guidelines in timely fashion given the rapidity of the pipeline development and approval pace. As of the writing of this commentary, one widely used set of guidelines for type 1 genotype endorses a combination of drugs that while the Food and Drug Administration (FDA)approved individually, are not in the favoured combination (http://www.hcvguidlines.org) demonstrating the extreme rapid nature of the changes in the field. In our opinion, such rapid and dramatic shifts in the therapy of a single disease are unprecedented.

{kind=link}
Simplified overview of the HCV life cycle and sites of direct acting antiviral therapies. HCV binds to one of several putative cell surface receptors and is internalised. Once inside the hepatocyte, the HCV genome is translated to produce a single large protein of around 3011 amino acids. The polyprotein is then proteolytically processed by proteases of viral and host origin to produce three structural and NS proteins. The NS proteins then recruit the viral genome into an RNA replication complex that is associated with rearranged cytoplasmic membranes. RNA replication takes places via the viral RNA-dependent RNA polymerase NS5B, which produces a negative strand RNA intermediate. The negative strand RNA then serves as a template for the production of new positive strand viral genomes. The NS5A protein is part of the cytoplasmic replication complex but has no enzymatic activity and although its function remains unclear it is critical to the viral lifecycle. New virus particles are thought to bud into the secretory pathway and are released at the cell surface. Inset: Proteins encoded by the HCV genome. The genome carries a long ORF encoding a polyprotein of 3010 amino acids. Translation of the ORF is directed via flankin NTR regions, which serve as robosomal entry sites. The HCV polyprotein is cleaved by viral-derived and host-derived proteases into structural and NS proteins. The putative functions of the cleavage products are shown. DAA, direct-acting antiviral; IFN, interferon; HCV, hepatitis C virus; NS, non-structural; ORF, open reading frame; NTR, non-translated.
Unanswered at the moment is: What will be the practical implications of these new therapies for patients with concurrent rheumatic diseases? In particular, there are virtually no data on the safety of these new agents in combination with antirheumatic drugs (ie, DMARDs or other immunosuppressives). While we have data on safety of tumour necrosis factor inhibitors in the presence of HCV, even when used concomitantly with standard interferon-based treatments,20 no such data yet exist for these new agents and thus caution is warranted. Similar to the interferon-based experience of the past two decades, careful investigations of efficacy and toxicity of the new and emerging antivirals in patients with rheumatic diseases, especially when used concomitantly with immunosuppressives, are sorely needed.
For now, what are rheumatologists to do? We have several suggestions but no doubt these will change soon pending further breakthroughs.
First, rheumatologists should increase their efforts to screen patients with HCV as most patients with the infection are undiagnosed. There are weak guidelines for HCV screening prior to methotrexate and leflunomide therapy but no comprehensive screening has been suggested. The Centers for Disease Control and Prevention advises testing all adults born between 1945 and 1965 as a possible strategy but others believe now is the time for universal screening.21 This advice appears even truer for rheumatologists, as many of their patients present with symptoms that may be or even mimic those in the long list of HCV extra hepatic manifestations.22 In addition, rheumatologists should take stock of patients already identified as having HCV who have not been effectively treated and for whom this problem may be considered inactive.
Patients with documented ongoing HCV infection, regardless of whether they have been previously treated and failed, should be referred to a hepatologist or liver specialist well familiar with the rapid advances and the availability of non-interferon-based and ribavirin-based therapies. If warranted, such patients should be treated or deferred for potentially even more effective regimen in the future.
For patients with HCV-induced rheumatic disease, especially HCV-associated cryoglobulinemia, while recent published recommendations have advocated a prominent role of pegylated interferon and ribavirin,10 there is no reason to doubt that future recommendations will advocate for ‘optimal’ HCV treatment (ie, interferon and ribavirin free) as experience with these regimes grows and data accrue.
Rheumatologists and hepatologists need to collaborate as organised societies to craft guidelines that are timely and to provide clear messaging on screening and treatment that is consistent with the rapid changes in the field.
The field of HCV therapy is evolving rapidly and emerging data suggest that all-oral treatments will be standard in the near future. For the vast majority of patients, these treatments will be curative and interferon-free. While this is good news for all patients infected with HCV, it is particularly good news for patients with rheumatic or connective tissue diseases either induced by or coincident with HCV infection. This new paradigm provides new impetus for HCV screening beyond risk-based strategies. Rheumatologists need to be aware of these advances and be positioned to work closely with specialists utilising such therapies and willing to work in partnership to treat this special population of patients.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.