Article Text

Abstract
Objectives To evaluate the impact of discontinuation of adalimumab (ADA) for 1 year in Japanese patients with early rheumatoid arthritis (RA).
Methods This 52-week postmarketing study, HOPEFUL-2, enrolled patients who had completed HOPEFUL-1 for early RA, in which patients received either ADA + methotrexate (MTX) or MTX alone in a 26-week randomised phase, followed by ADA+MTX in a 26-week open-label phase.
Results A total of 220 patients (ADA discontinuation: 114 patients vs ADA continuation: 106 patients) were enrolled in this study. The proportion of patients with sustained low disease activity (LDA) in the ADA discontinuation group was significantly lower than that in the continuation group (80% (64/80 patients) vs 97% (71/73 patients); p=0.001); however, most patients sustained LDA in both groups. In patients with 28-joint disease activity score (DAS28)-C reactive protein ≤2.0 at week 52, the proportion of patients who achieved sustained LDA at week 104 was 93%, suggesting that DAS28 remission may be a predictor to indicate biological-free disease control in patients with early RA. The incidence of adverse events (AE) was significantly lower in the ADA discontinuation group than in the continuation group (34.2% (39/114 patients) vs 48.1% (51/106 patients); p=0.04), most notably for infection (14.9% vs 27.4%, p=0.031).
Conclusions Although ADA discontinuation was associated with an increase in disease activity, a large proportion of patients maintained LDA with MTX monotherapy after ADA discontinuation. Since ADA discontinuation was associated with a lower AE incidence, physicians should weigh the risks and benefits of ADA discontinuation.
Trial registration number NCT01163292.
- Rheumatoid Arthritis
- Anti-TNF
- Treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
In the treatment of rheumatoid arthritis (RA), an increasing concern has been raised about the possibility of successful tapering/withdrawal of biologic agents. However, sufficient information is not available to apply this therapeutic approach to patients with RA in a real-world medical setting.
What does this study add?
This post-marketing observational study demonstrated that a large proportion of early RA patients who had received either adalimumab (ADA)+methotrexate (MTX) or MTX alone for the first 26 weeks, followed by 26-week treatment with ADA+MTX, were able to maintain low disease activity with MTX monotherapy after 24-week ADA discontinuation. It was suggested that 28-joint disease activity score (DAS28)-C-reactive protein remission may be a predictor for successful ADA discontinuation.
How might this impact on clinical practice?
The findings imply that, although physicians should weigh its risks and benefits, they may consider ADA discontinuation in early RA patients who had received appropriate initial therapy.
Introduction
Rheumatoid arthritis (RA) is a progressive systemic inflammatory disease that, in the absence of appropriate treatment, results in joint destruction and functional disability.1 ,2 It is widely recognised that the combination of antitumour necrosis factor α (TNF-α) antibody with methotrexate (MTX) is associated with significantly better outcomes than MTX monotherapy.3–8 However, often there are significant barriers (economic reasons, patient preference, etc) that limit the introduction of biological therapies in the treatment of RA.
Recent studies have indicated that biological agents may be tapered or even discontinued in some patients in certain situations. For instance, intensive therapy early in the disease course and rapid attainment of stable low disease activity (LDA) or remission have been associated with maintenance of response on tapering/withdrawal;9 the biological agent can be restarted at a later date in the event of disease flare. Such an initial intensive therapy approach may be favoured economically and by patients, if it leads to outcomes similar to those experienced by patients who continue biological agents.
Despite several studies assessing biological tapering/withdrawal, some questions such as whether successful tapering/withdrawal can be achieved in patients with an initial inadequate response to MTX monotherapy remain to be addressed. Furthermore, to date few predictors of a sustained response following biological tapering/withdrawal have been identified.
Given these circumstances, we conducted this follow-up study to assess the effects of discontinuation of ADA on the effectiveness and safety following the phase III study, HOPEFUL-1, that evaluated the efficacy and safety of adalimumab (ADA) in combination with MTX in Japanese patients with early RA as compared with MTX monotherapy.10 The HOPEFUL-2 was designed to follow-up on the effectiveness and safety findings and to assess the ability to maintain a response after discontinuation of ADA in the period after the HOPEFUL-1, that is, our aims were to determine in a real-world medical setting whether patients receiving these ADA regimens can sustain their clinical responses and to identify factors contributing to sustained efficacy.
Methods
Study design
The 52-week postmarketing observational study, HOPEFUL-2, was conducted to follow-up the phase III study conducted between March 2010 and October 2012 in accordance with the Declaration of Helsinki and Good Postmarketing Study Practice in Japan after the reviews and approval by the Japanese Pharmaceuticals and Medical Devices Agency. This study is registered with ClinicalTrials.gov (NCT01163292).
The HOPEFUL-2 enrolled patients who had completed the 52-week HOPEFUL-1 study (figure 1). The design and main results of the HOPEFUL-1 study were previously reported in detail.10 Briefly, the study in patients with early RA consisted of a 26-week randomised double-blind placebo-controlled phase followed by a 26-week open-label phase. Eligible patients had early RA (age ≥20 years, <2 years RA duration) according to the 1987 revised American Rheumatism Association criteria,11 had poor prognostic factors for RA with high disease activity and had not previously been treated with MTX. In the randomised phase, patients received either subcutaneous injections of ADA 40 mg or placebo every other week, both in combination with oral MTX (ADA + MTX (intensive therapy) vs MTX alone (standard therapy)) for 26 weeks. Subsequently, during the open-label phase from week 26 to week 52, all patients received the ADA + MTX combination therapy.
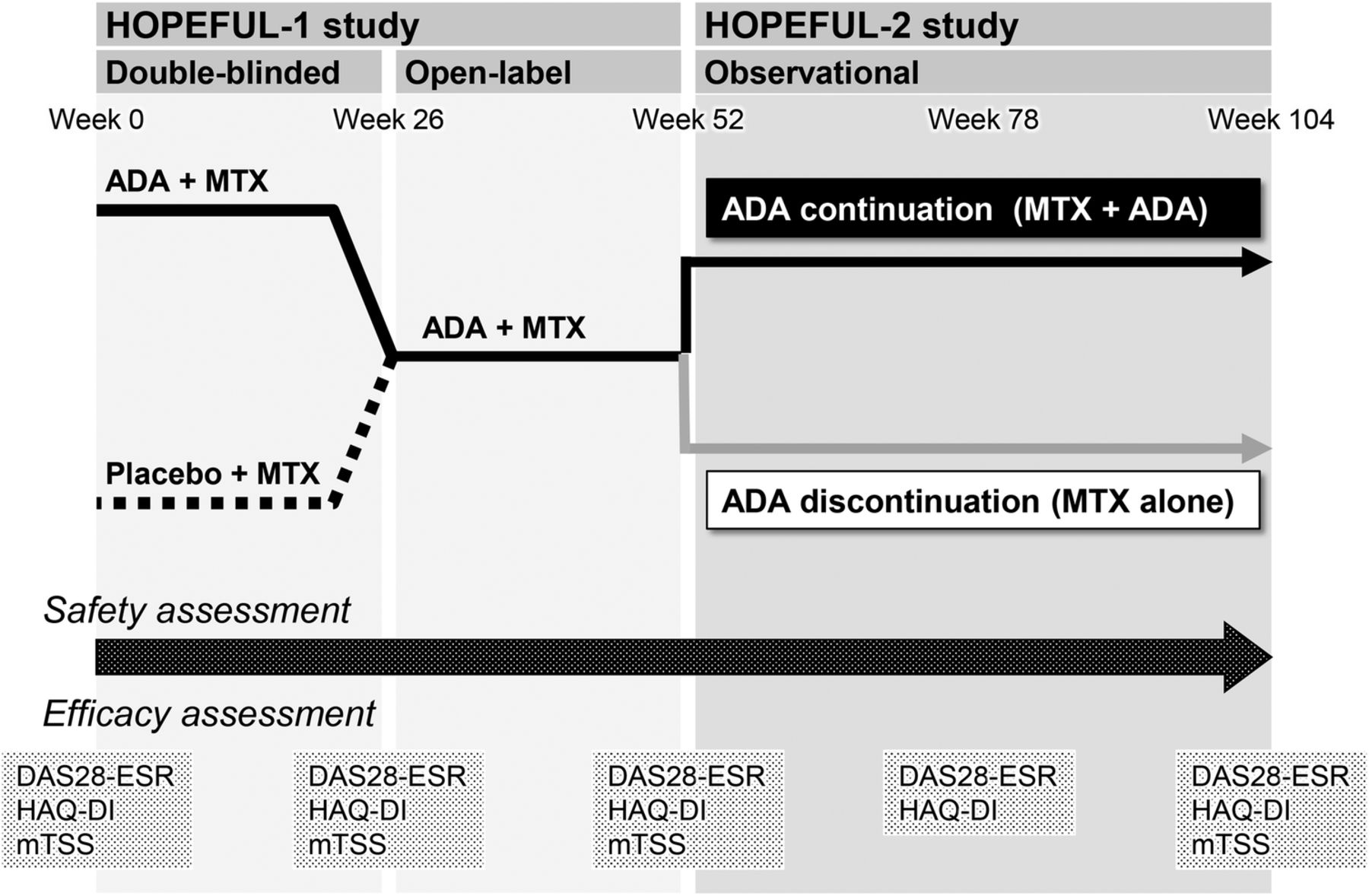
Study designs of HOPEFUL-1 and HOPEFUL-2. The HOPEFUL-1 study comprised a 26-week randomised phase (ADA + MTX (intensive therapy) vs MTX alone (standard therapy)) followed by a 26-week open-label phase (all patients received ADA + MTX). At completion of the HOPEFUL-1 study (at week 52), patients were asked to participate in HOPEFUL-2 and, if consent was provided, were followed for another 52 weeks (until week 104). ADA, adalimumab; MTX, methotrexate; DAS28, disease activity score 28; ESR, erythrocyte sedimentation rate; HAQ-DI, Health Assessment Questionnaire disability index; mTSS, modified total sharp score.
At the completion of the HOPEFUL-1 study (at week 52), patients were asked for their consent to participate in HOPEFUL-2 and for the use of the data obtained during the HOPEFUL-1 study. The decision as to whether to continue or discontinue ADA in the HOPEFUL-2 was made by informed consent from each patient. In the ADA continuation group, patients received subcutaneous injections of ADA 40 mg and MTX, while patients in the ADA discontinuation group received MTX alone (figure 1).
Safety and effectiveness assessment
All adverse events (AEs) were recorded and coded according to the Medical Dictionary for Regulatory Activities V.14.0.
Disease activity, functional and radiographic effects were evaluated using the 28-joint disease activity score (DAS28), health assessment questionnaire-disability index (HAQ-DI) 12 and mTSS,13 respectively. In patients who achieved DAS28 C reactive protein (CRP) <3.2 sustainably at weeks 46 and 52 of the HOPEFUL 1 study as assessed by a post hoc analysis, therapeutic outcomes were compared between the ADA discontinuation and continuation groups. LDA was defined as DAS28-CRP <3.2 and indicating remission as DAS28-CRP <2.6. Radiographic non-progression was defined as a change in mTSS ≤0.5, and rapid radiographic progression (RRP) was defined as an annual progression rate of >5 units.
Statistical analysis
Demographic and baseline characteristics were analysed using Fisher's exact test for categorical variables and the Wilcoxon rank sum test for continuous variables. Univariate logistic regression was performed to identify predictors of sustained LDA. Multivariate regression was used to analyse factors with p <0.1 in the univariate analyses. Receiver operating characteristics (ROC) curve analysis was conducted to determine the DAS28-CRP cut-off value at week 52. Radiographic progression and functional outcomes over time were compared using the Wilcoxon signed rank test. The last observation carried forward method was used for imputing missing data of clinical or functional values after the initiation of ADA discontinuation. Linear extrapolation was used for missing radiographic outcomes. Analysis of safety included all patients who participated in this study and the percentages of AEs were compared between the ADA discontinuation and continuation groups using Fisher's exact test. All reported p values are two-sided and not adjusted for multiple testing. A difference with a p value of <0.05 was considered to be significant. The analyses were performed using StatView for Windows V.5.0 and SAS 9.3, SAS Institute Inc, Cary, North Carolina, USA.
Results
Patients
A total of 220 patients agreed to participate in HOPEFUL-2. Of these, 114 opted to discontinue ADA (MTX monotherapy), while 106 chose to continue ADA in combination with MTX (ADA + MTX). The baseline characteristics (weeks 0 and 52 in HOPEFUL-1) were similar in the ADA continuation and discontinuation groups. A total of 157 patients (65 patients in the ADA + MTX group and 92 patients in the MTX monotherapy group) completed the 52-week extension period (figure 2).

Patient dispositions throughout HOPEFUL-1 and HOPEFUL-2. ADA, adalimumab.
Changes in DAS28-CRP and sustainability of LDA
Of the 220 patients enrolled, 188 (96 in the ADA discontinuation group; 92 in the ADA continuation group) had DAS28 measurement at week 52 (baseline of HOPEFUL-2) and were followed to allow further assessment (table 1); the mean DAS28-CRP was 2.1 and 2.2, respectively, and 82 patients (85%) and 77 patients (84%) were in LDA. At week 104, the mean DAS28-CRP was 2.5 and 2.0 in the ADA discontinuation and continuation groups, respectively, showing a greater increase in the former (p=0.006; table 2).
Patients’ baseline characteristics at weeks 0 and 52
Clinical, functional and structural outcomes of patients including those who failed to achieve stable LDA at week 52
The proportion of patients who achieved indicating clinical remission (DAS28-CRP <2.6) or LDA (DAS28-CRP <3.2) was significantly lower in the ADA discontinuation group than in the ADA continuation group (DAS28-CRP indicating remission/LDA: 60.4%/74.0% vs 76.1%/91.3%, p=0.028/0.002; table 2).
Effects of the initial therapy and factors associated with LDA
To fully rule out the effects of other drugs, all patients who received rescue treatment during HOPEFUL-1 were excluded. Table 3 shows the characteristics of patients who achieved LDA at weeks 46 and 52 of the HOPEFUL 1 study. Patients who received initial intensive therapy with ADA+MTX showed greater improvement in terms of inhibition of the structural damage measured by count of erosion, JSN and mTSS at week 52 as compared to those who received standard MTX therapy without ADA, reflecting the results of the HOPEFUL-1 study.10
Characteristics of patients with RA who agreed to or declined ADA discontinuation at the start of HOPEFUL-2
The proportion of patients who achieved LDA at week 104 was lower in the ADA discontinuation group than in the ADA continuation group (64/80 patients, 80% vs 71/73 patients, 97%, p=0.001; figure 3). A similar trend was observed regardless of whether patients received MTX monotherapy or ADA+MTX combination therapy during week 0–26 in the HOPEFUL-1 study (data not shown).

Time courses of disease activity scores assessed by the 28-joint disease activity score based on C reactive protein (DAS28-CRP) in patients who achieved the target low disease activity at weeks 46 and 52 (80 patients in the ADA discontinuation group and 73 patients in the ADA continuation group). ADA, adalimumab.
In the ADA discontinuation group, DAS28-CRP differed significantly between patients with sustained and failed LDA at week 104 (table 4). Multivariate regression analysis demonstrated that DAS28-CRP, but not other markers tested including CRP itself, was a significant factor that affects sustainability of LDA following 52-week discontinuation of ADA. Subsequent ROC analysis identified a cut-off value of DAS28-CRP 2.0, with a sensitivity of 81%, specificity of 75% and area under the curve of 0.818. The numbers of patients with DAS28-CRP <2.0 were 27/34 (79.4%) in the sustained LDA group with ADA+MTX therapy during week 0–26 in the HOPEFUL-1 study and 24/30 (80.0%) with MTX monotherapy during the same initial period of the HOPEFUL-1 study. On the other hand, 5/8 patients in the failed LDA group with ADA+MTX therapy during week 0–26 of the HOPEFUL-1 study and 7/8 with MTX monotherapy during the same initial period had DAS28-CRP >2.0 in the HOPEFUL-1 study.
Relationship between patient characteristics at week 52 and the LDA sustainability outcomes at week 104 in the ADA discontinuation group (n=80)
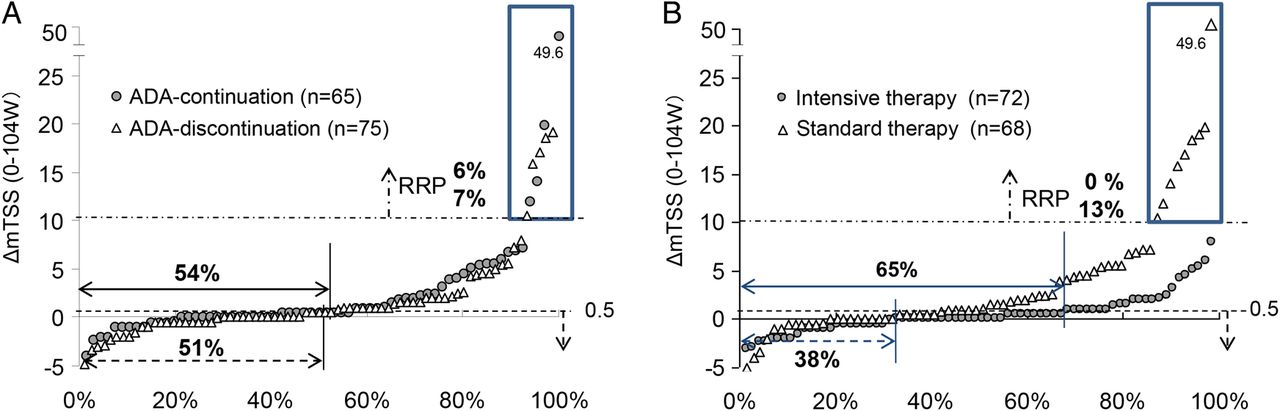
Changes in ΔmTSS
The within-patient differences in radiographic progression as assessed by mTSS were compared between the ADA discontinuation and continuation groups, and also according to the initial therapy. The proportions of patients showing radiographic non-progression increased similarly in these two groups (figure 4A). There were significant differences in radiographic progression at week 104 between patients who received initial intensive and standard therapy (figure 4B). All patients who had RRP at week 104 had received initial standard therapy. A similar trend was observed regardless of whether patients continued or discontinued ADA during weeks 52–104 of the HOPEFUL-2 study (data not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative probability plots of changes in mTSS (ΔmTSS) for 2 years (0–104 weeks) in patients in the ADA discontinuation group versus ADA continuation group (A); in patients in the initial intensive therapy group versus standard therapy group (B). ADA, adalimumab; mTSS, modified total sharp score; RRP, rapid radiographic progression.
Safety
Table 5 summarises the AEs in patients enrolled in HOPEFUL-2 (n=220). Overall, there were no cases with tuberculosis nor any deaths in either the ADA discontinuation group or the ADA continuation group. The percentage of patients who experienced AEs was significantly lower in the ADA discontinuation group than in the ADA continuation group (34.2% (39/114 patients) vs 48.1% (51/106 patients); p=0.04), and the difference was most noted for infection rates (14.9% vs 27.4%, p=0.031). Nevertheless, there was no significant difference in the incidence of serious AEs between the two groups, and most infections observed in the ADA continuation group did not lead to serious consequences such as hospitalisation.14
Summary of adverse events
Discussion
HOPEFUL-2, a postmarketing observational study conducted to assess the ability to maintain a response after discontinuation of ADA administered during the preceding HOPEFUL-1 study, investigated the continuous effectiveness on joints and safety of ADA in Japanese patients with early RA. ADA discontinuation was associated with a slight increase in disease activity as compared to patients who continued ADA therapy; however, there were no significant differences in functional or structural measurements between the two groups. The joint destruction progression appeared to be decreased radiographically during the 2-year period of the HOPEFUL-1 and HOPEFUL-2 studies.
Recent studies have shown that biological agents can be tapered or even withdrawn from the therapeutic regimens of patients who have achieved clinical remission.7 ,8 The impact of discontinuing treatment with biologics in HOPEFUL-2 cannot be adequately evaluated given the limited number of patients who were subsequently divided into two self-selected groups. Nonetheless, the proportions of patients who sustained LDA and clinical remission for 1 year after ADA discontinuation (80% and 65%, respectively) were similar to the findings (81% and 68%, respectively) obtained in the OPTIMA study. The fact that approximately half of the patients who had achieved LDA opted to discontinue ADA in the present study can be considered to reflect patient choices made in clinical practice. Therefore, we consider the findings of our study to be meaningful for understanding patient outcomes and choices in actual clinical settings.
In this study, the proportion of patients who sustained LDA in the ADA discontinuation group was significantly lower than that in the ADA continuation group (80% vs 97%, respectively; p=0.001). However, with the cut-off value for DAS28-CRP set at ≤2.0, the proportion of patients who achieved LDA (93%) in the ADA discontinuation group was similar to that of patients with LDA in the ADA continuation group, suggesting that DAS28 remission may be a predictor to indicate biological-free disease control in patients with early RA. Nevertheless, in the RRR study15 using infliximab and the HONOR study16 using ADA, both of which involved patients with established RA, the proportions of patients who maintained LDA without biologics for 1 year (71.4% and 79% of patients with DAS28-erythrocyte sedimentation rate (ESR) <2.225 and ≤1.98 defined in the respective studies as sustained LDA and remission) were lower than those in this study, taking the difference between DAS-CRP and DAS-ESR into consideration. This suggests that earlier intervention may increase the success rates of biological-free disease control without stringent criteria, such as the major remission required for patients with established RA.
No overall safety profile changes in ADA were recognised. Since ADA discontinuation was associated with a lower incidence of AEs, particularly infections, we must weigh the risks and benefits when determining optimal treatment after patients have achieved early remission or LDA.
In this study, the within-patient differences in radiographic progression assessed by mTSS were similar in the ADA discontinuation and continuation groups. On the other hand, the initial 6-month treatment (week 0–26) might have affected subsequent changes in mTSS (week 52–104), because all patients who had RRP at week 104 received MTX monotherapy from weeks 0 to 26 followed by the ADA + MTX combination therapy from weeks 26 to 52. In patients receiving the initial standard therapy, the proportion who achieved ΔmTSS ≤0.5 (week 52–104) was lower than that in patients receiving the initial intensive therapy (63% vs 83%; p=0.008). In addition, 4% of patients who had received the initial standard therapy had RRP during the later period (week 52–104), even among those with sustained LDA at week 52. The reasons for this were not clear, but the following explanations are suggested: recovery from severely osteoclast-dominant conditions in RA takes a long time,17 ,18 that is, restoration of a balanced osteoblast–osteoclast axis is a prolonged process; and therapy with TNF antagonists reduces matrix metalloproteinase (MMPs)19 and also modulates the osteoprotegerin/receptor activator of the nuclear factor (NF) κB ligand system resulting in bone formation being favoured.20–22 Further investigation may facilitate understanding the long-term benefits of joint preservation by intensive therapy with ADA + MTX in addition to earlier prevention of joint destruction.
Finally, the impact of MTX dose (the mean MTX dose in this study was 7.1 mg/week) on the results should be considered. The effects of 10 mg and 20 mg/week doses of MTX in the combination therapy with ADA are reportedly equivalent in patients with early RA. In the CONCERTO study,23 ,24 MTX 10 mg/week was used in combination with ADA, which is deemed equivalent to MTX 7 mg/week in this study based on the mean body weights of the study patients being 78.2 kg and 55.8 kg, respectively. However, these are the doses when used in combination with ADA, and a higher MTX dose would be necessary in monotherapy to prevent joint destruction in patients with early RA.
In conclusion, this 52-week follow-up study of the HOPEFUL-1 study involving Japanese patients with early RA showed sustained effectiveness in terms of joint damage prevention. Although ADA discontinuation was associated with a slight increase in disease activity, a large proportion of patients (80%) maintained LDA with a low dose (mean 7.1 mg/week) of MTX monotherapy after ADA discontinuation. This observation suggested that DAS28-CRP indicating remission may be a predictor to indicate biological-free disease control in patients with early RA. Since ADA discontinuation was associated with a lower incidence of AEs, particularly infections, physicians should weigh the risks and benefits of ADA discontinuation. Overall, the early intensive-later maintenance approach appears to be a viable treatment option for patients with early RA.
Limitations
In this real-world observational study, patients were not randomised to the adalimumab continuation and discontinuation groups, and there could be differences in terms of financial situation from patient to patient, suggesting potential biases derived from patients deciding whether or not to continue ADA, including the necessity of paying their own medical expenses. Thus, clinical predictors for discontinuation of biologics are required to provide patients with optimal therapeutic options.
Acknowledgments
The authors thank all patients, investigators and support staff who participated in the study, as well as Benjamin Wolfe, PhD, of AbbVie Inc, for editorial assistance. The authors acknowledge the contribution of Mr Naoto Hirota to the data analyses (Stella Co, Ltd); this assistance was funded by Abbvie.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors KK and KH were involved in the data collection and data analyses. YT was the principal investigator in this study. All authors participated in the study design, interpretation of study results, and in the drafting, critical revision and approval of the final version of the manuscript.
Funding AbbVie GK and Eisai Co, Ltd sponsored the study, contributed to its design, participated in the collection, analysis and interpretation of the data, and in the writing, review and approval of the final manuscript.
Competing interests YT has received consulting fees, speaking feesand/or honoraria from Abbvie, Daiichi-Sankyo, Chugai, Takeda, Mitsubishi-Tanabe, Bristol-Myers, Astellas, Eisai, Janssen, Pfizer, Asahi-Kasei, Eli Lilly, GlaxoSmithKline, UCB, Teijin, MSD and Santen, as well as research grants from Mitsubishi-Tanabe, Takeda, Chugai, Astellas, Eisai, Taisho-Toyama, Kyowa-Kirin, Abbvie and Bristol-Myers. HY has received research grants from AbbVie GK, Bristol-Myers Squibb, Chugai Pharmaceutical Co, Eisai Co, Ltd, Janssen Pharmaceutical K.K., Mitsubishi Tanabe Pharma Corporation, Otsuka Pharmaceutical, Pfizer Japan Inc, Takeda Pharmaceutical Company and UCB Japan Co, Ltd, and speakers honoraria/consulting fees from AbbVie GK, Bristol-Myers Squibb, Chugai Pharmaceutical Co, Eisai Co, Ltd, Janssen Pharmaceutical K.K., Mitsubishi Tanabe Pharma Corporation, Otsuka Pharmaceutical, Pfizer Japan Inc, Takeda Pharmaceutical Company and UCB Japan Co, Ltd. NI has received research grants from Abbott Japan Co, Ltd, Astellas Pharma, Bristol-Myers Squibb, Chugai Pharmaceutical Co, Eisai Co, Ltd, Janssen Pharmaceuticals, Inc, Mitsubishi Tanabe Pharma Corporation, Pfizer Japan Inc and Takeda Pharmaceutical Company. NM has received research grants from AbbVie GK, Astellas Pharma, Banyu Pharmaceutical Co, Ltd, Chugai Pharmaceutical Co, Daiichi Sankyo, Eisai Co, Ltd, Janssen Pharmaceuticals, Inc, Mitsubishi Tanabe Pharma Corporation, Takeda Pharmaceutical Company and Teijin Pharma Limited. KK and KH are shareholders and employees of AbbVie GK. TT has received grants from AbbVie GK, Astellas Pharma, Bristol-Myers K.K., Chugai Pharmaceutical Co, Daiichi Sankyo, Eisai Co, Ltd, Janssen Pharmaceutical K.K., Mitsubishi Tanabe Pharma Corporation, Nippon Shinyaku Co, Ltd, Pfizer Japan Inc, Sanofi K.K., Santen Pharmaceutical Co, Ltd, Takeda Pharmaceutical Company and Teijin Pharma Limited, speaking fees from AbbVie GK, Bristol-Myers Squibb K.K., Chugai Pharmaceutical Co, Eisai Co, Ltd, Janssen Pharmaceutical K.K., Mitsubishi Tanabe Pharma Corporation, Pfizer Japan Inc and Takeda Pharmaceutical Company, and consultant fees from AstraZeneca K.K., Eli Lilly Japan K.K., Novartis Pharma K.K., Mitsubishi Tanabe Pharma Corporation and Asahi Kasei Medical Co, Ltd.
Patient consent Obtained.
Ethics approval HOPEFUL-2, a prospective observational study, was conducted between March 2010 and October 2012 in accordance with the ethical of the Declaration of Helsinki and Good Postmarketing Study Practice in Japan after the reviews and approval by the Pharmaceuticals and Medical Devices Agency (PMDA). This 52-week study was designed to assess the benefits and risk of ADA discontinuation versus continuation (clinicaltrials.gov identifier, NCT01163292).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.