Article Text

Abstract
Objectives We aim to evaluate the effect on different ways of classifying pain sensitisation on impact and quality of life (QoL) in knee osteoarthritis (KOA).
Methods We used baseline data from a cohort of consecutive patients with KOA listed for arthroplasty. We collected demographics and number of painful body sites. We measured pressure pain thresholds at the right forearm (PPTarm). Pain sensitisation was classified using: (1) widespread pain, (2) lowest 10th percentile of PPTarm and (3) PainDETECT questionnaire ≥13/38. Impact and QoL were assessed using Western Ontario and McMaster Universities Osteoarthritis Index and Short Form-36. Impact and QoL scores in patients with or without pain sensitisation were compared. We evaluated the association of pain sensitisation measures with QoL scores using multivariable regression.
Results 233 patients (80% female, mean age 66 years) included in the analysis; 7.3%, 11.6% and 4.7% were classified as having pain sensitisation by widespread pain, low PPTarm and PainDETECT criteria, respectively. There was minimal overlap of patients as classified as pain sensitisation phenotype by different measures. Patients with pain sensitisation had poorer QoL compared with those without. Low PPTarm identified patients with poorer general health, while widespread pain and PainDETECT identified poorer QoL in more psychological domains. There was weak correlation between number of painful body sites and PainDETECT (rho=0.23, p<0.01), but no significant correlation with PPTarm.
Conclusion Patients with KOA with pain sensitisation have poorer QoL compared with those without, regardless of classification method. Different criteria defined patients with different pattern of QoL impact.
- osteoarthritis, knee
- health services research
- outcome assessment, health care
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Pain sensitisation is one of the contributing factors to pain in knee osteoarthritis (KOA).
There are various methods that can be used to assess the concept of pain sensitisation, but no standardisation has yet been established.
What does this study add?
The current study showed the additional burden of pain sensitisation to pain, physical function and quality of life in patients with KOA listed for arthroplasty.
Different criteria to classify pain sensitisation defined patients with different pattern of quality of life (QoL) impact.
How might this impact on clinical practice or further developments?
This highlights the important impact that pain sensitisation has on pain, function and QoL for patients with KOA.
Further studies are required to develop standardised protocols for the assessment of pain sensitisation that can be applied in a clinical setting, and define clear cut-offs and criteria for the identification of pain sensitisation phenotypes that would affect disease burden and outcomes of interventions.
Introduction
Knee osteoarthritis (KOA) is the most common type of arthritis, estimated to affect 16% of the world’s population. The global incidence of incident KOA was 86.7 million individuals in 2020.1 KOA is also one of the major causes of disability worldwide.2 Pain is the key symptom of KOA and the main driver for functional disability and negative impact on different aspects of quality of life (QoL), including mobility, participation, mood and sleep.3 4 Pain in KOA is mechanical and was traditionally thought to be nociceptive. However, discordance between pain and the degree of structural joint damage have been recognised.5 A growing body of evidence is emerging to show the contribution of various pain mechanisms, some of which can involve alterations in nerve processing in both the peripheral and central nervous systems.6 A conceptual framework of complex interplay of physical, psychological, social and neurobiological factors has evolved to explain the chronic pain and disability in KOA.4
Pain sensitisation has been shown to be one of the contributory factors to persistent pain in KOA.4 7 Pain sensitisation is as a complex pathophysiological phenomenon, or group of phenomena, with several underlying mechanisms at both spinal and brain levels. Continuous nociceptive inputs from KOA resulted from tissue injury or inflammation may lead to decrease in excitation threshold of the peripheral nociceptors (peripheral pain sensitisation). Neuroplastic changes in the dorsal horn transmission neuron receptors and central nervous system have been described that may associate with an increase in responsiveness to peripheral inputs (central pain sensitisation).4 8 Qualitative study among patients with knee or hip osteoarthritis has revealed that the pain experience started with a dull aching pain which became more constant over time, and punctuated increasingly with short episodes of a more intense and unpredictable pain that causes more profound psychological and social impacts.3 Studies have found that patients with KOA and concomitant pain sensitisation have lower QoL compared with those without.9–11 Knee arthroplasty is the treatment of choice for severe KOA. It is hypothesised that replacement of a diseased joint alleviates pain through removing the peripheral source of pain. Despite the success of knee arthroplasty for many patients, 10%–34% of patients experience chronic pain after surgery.12 The strongest preoperative risk factors for chronic pain after knee arthroplasty are preoperative pain severity, poor mental health, pain catastrophising and presence of patient comorbidities.13 A systematic review has also highlighted the importance of psychosocial influences and central pain modulation indices on arthroplasty outcomes.14
Currently, there are various methods that have been used to assess the concept of pain sensitisation, but no standardisation has yet been established.15 First is quantitative sensory testing (QST) methods that include pain pressure thresholds (PPTs),16 temporal summation17 and conditioned pain modulation.18 These modalities are often labour intensive and require careful standardisation to produce reliable results. Second, there are patient-reported outcomes (PROs) developed to evaluate neuropathic pain-like symptoms that can be completed by patients. The third is the traditional widespread pain concept—defined as pain above and below the waist, pain on the right and left sides of the body and axial skeleton.19 The absence of properly validated method with standardised cut-off points for the evaluation of the concept of pain sensitisation challenges the interpretation of results and makes the comparison of results across studies difficult.20 Having tools in clinical practice with which to identify those patients with pain sensitisation would help in selection of the best pain therapies. In this study, we aimed to explore the different methods of classifying pain sensitisation and the impact on pain, physical function and QoL for patients with KOA who were scheduled for knee arthroplasty.
Methods
We conducted a post hoc analysis using the baseline cross-sectional dataset of 249 adult patients with KOA listed for knee arthroplasty, recruited from the pre-operative centre of Singapore General Hospital from June to November 2015.
The study design and protocol of the original study have been published previously.21 In brief, patients listed for knee arthroplasty for clinician diagnosed KOA were recruited 1–2 weeks prior to arthroplasty at pre-operative assessment visit. We excluded revision arthroplasty or arthroplasty performed for other diagnoses, and cognitive impairment. Data were collected using self-administered questionnaire on sociodemographic variables including age, sex, ethnicity and educational attainment. Comorbidities were self-reported using the Functional Comorbidity Index,22 which asks about the presence or absence of 18 comorbidities to produce a score ranging from 0 to 18. Instead of administered by clinicians, the Functional Comorbidity Index was self-reported by patients in this study. The presence or absence of current pain in body sites were self-reported (detailed below). We summated the total number of painful body sites including the knee listed for arthroplasty. Body weight and height were measured at recruitment and used to calculate body mass index (BMI). Knee radiographs taken as part of routine care for the knee underdoing arthroplasty (index knee) were scored according to the Kellgren-Lawrence (KL) grading.23 Two researchers blinded to the clinical data of patients independently scored 30% of the radiographs for reliability. The intraclass correlation coefficient (ICC) of KL grading was 0.86 (95% CI 0.76 to 0.91).21 Index knee was defined as the knee listed for knee replacement (KR), and the dominant knee in case of bilateral KR. In case of bilateral arthroplasty, the dominant knee was designated as the index knee.
Pain sensitisation concept
We classified patients to be having pain sensitisation with the following three sets of criteria.
Pressure pain thresholds
PPT was selected as it is one of the least variable QST measurements used to assess pain sensitisation.16 Meta-analysis revealed patients with KOA had lower PPT compared with healthy controls (mean difference −0.85; 95% CI −1.1 to –0.6). One designated staff (Shuqin Xiong), who was blinded to clinical data and questionnaire outcomes, was trained to measure PPT for all patients using a handheld digital algometer (Somedic, Sweden) to minimise measurement variability. A 1 cm2 probe was placed perpendicular to the skin, and pressure was applied at a constant rate of 10 kPa/s. The patients were instructed to say ‘stop’ at the very first sensation of pain, at which point the PPT reading was recorded. A total of three readings were recorded, with the average of the last two readings taken to increase reliability. PPT were measured at the medial joint line of the index knee (PPTknee) and the volar side of right forearm (PPTarm) to represent peripheral and central sensitisation, respectively. As the PPT taken at a distant site may represent more of central sensitisation,20 we used PPTarm for this study.20 Repeat PPT measurements were taken for 25 patients on the day of arthroplasty (median 9 days from the first PPT measurements, range 2–16 days) for test–retest reliability evaluation. The ICC (95% CI) of PPTarm was 0.80 (0.64 to 0.91). There are no current cut-offs developed for pain sensitisation, we used a distributional method and took the lowest 10th percentile of PPTarm to indicate the presence of pain sensitisation. This 10th percentile is chosen to represent the extreme end of the phenotype, and also to achieve a similar proportion of ‘sensitised’ patients as classified by the other two criteria sets.
PainDETECT
PainDETECT is a PRO developed to screen for neuropathic pain symptoms.24 Due to its association of pain quality with augmented central pain processing as shown in functional magnetic imaging,25 PainDETECT has been considered of its utility in the identification of pain sensitisation.26 27 It comprises 12 items that evaluates current pain severity, pain patterns, graphic representation of body sites and severity of somatosensory symptoms. A total score of −1 to 38 is assigned to represent the likelihood for neuropathic pain: (a) definitely neuropathic (>18), (b) possibly neuropathic13–18 and (c) unlikely to be neuropathic (<13). We defined pain sensitisation as a score of ≥13 on the PainDETECT. PainDETECT has been validated with good agreement and correction with the Self-Report Leeds Assessment of Neuropathic Symptoms and Signs questionnaires in KOA and supported by Rasch model analyses.25 Recently, a modified version of PainDETECT was validated for content validity in patients with KOA to identify neuropathic-like symptoms, and a cut-off of ≥12 predicts pain sensitisation as measured by QST.27 The modified version was not used in the current study as it was not available at the time of study planning.
Widespread pain
Patients self-reported the presence of current pain in nine body sites in addition to the planned arthroplasty knee in a yes or no response to the following sites: 1. neck; 2. left shoulder, elbow or hand, 3. right shoulder, elbow or hand; 4. lower back; 5. the other knee; 6. left hip; 7. right hip; 8. left ankle or foot and 9. right ankle or foot. Widespread pain was defined as the presence of pain in both the upper and lower trunk, involving both sides of the body, and axial skeleton pain.19 Patients with KOA with widespread pain were found to have lower PPT and poorer physical function than those with KOA alone or KOA with low back pain.11
Impact and quality of life measures
The severity of knee pain and functional limitations in the index knee was assessed using the Western Ontario and McMaster University Index (WOMAC).28 The WOMAC pain and function scores were standardised to 0–100, with a higher score indicating more severe symptoms.
QoL was evaluated using the self-administered Medical Outcome Survey Short-Form 36 (SF-36),29 which assesses eight domains of health, including physical functioning (PF), role limitations due to physical health (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE) and mental health (MH). Each domain is scored on a 0–100 range, with lower scores represent lower QoL. Physical component score (PCS) and the mental component score (MCS) were aggregated and standardised to the Singapore population norm.30
Statistical analysis
Sample size was estimated based on the original study.21 Demographic variables are presented using descriptive statistics, using means (SD) or medians (IQR) as appropriate. We compared the impact and QoL variables in patients classified as pain sensitisation versus none according to the three sets of classification criteria using Student’s t-test.
Correlations between scores for measurement of pain sensitisation (PPTarm, PainDETECT and number of painful body sites) and impact (WOMAC pain, WOMAC function) and QoL (SF-36) were calculated. Generalised linear regression models were used to explore the associations of the different pain sensitisation measurements with impact/QoL outcomes with adjustment with age, sex, ethnicity (Chinese vs non-Chinese), education level (none vs primary vs secondary or above), BMI, radiographic KOA severity (KL0-3 vs KL4) and Functional Comorbidity Index score. These adjustment variables were chosen as they have previously been found to be associated with QoL in KOA.31 32 P values <0.05 were taken as statistically significant. All analyses were conducted using IBM SPSS statistic package, V.25.
Results
Out of the 249 recruited patients, 233 patients had complete data for all three pain sensitisation criteria and were included in the analysis. Baseline characteristics are summarised in table 1. The mean (SD) age of patients was 66.0 (8.3) years, 186 (79.8%) were female and 194 (83.3%) were Chinese. Mean (SD) WOMAC pain and function scores were 41.7 (18.0) and 35.0 (17.9), respectively. The three most common comorbidities were diabetes mellitus (n=53; 22.7%); visual impairment (n=47; 20.2%) and osteoporosis (n=26; 11.2%). One hundred and forty-three patients (61.4%) had painful body sites other than the index knee. Median (IQR) number of painful body sites, including the knee listed for arthroplasty was 2.0 (2.0).
Demographical data of patients included (n=233)
Pain sensitisation concept
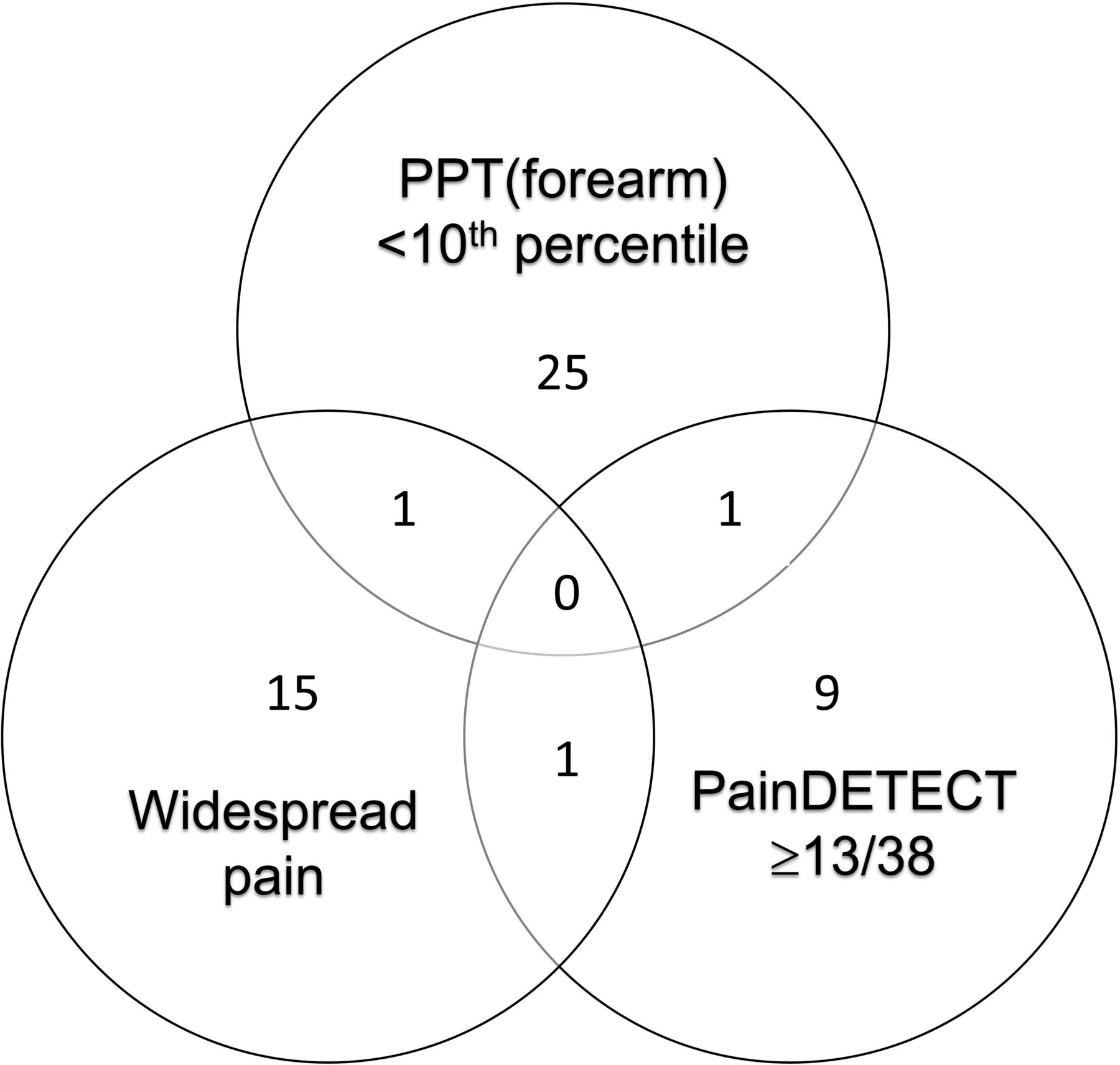
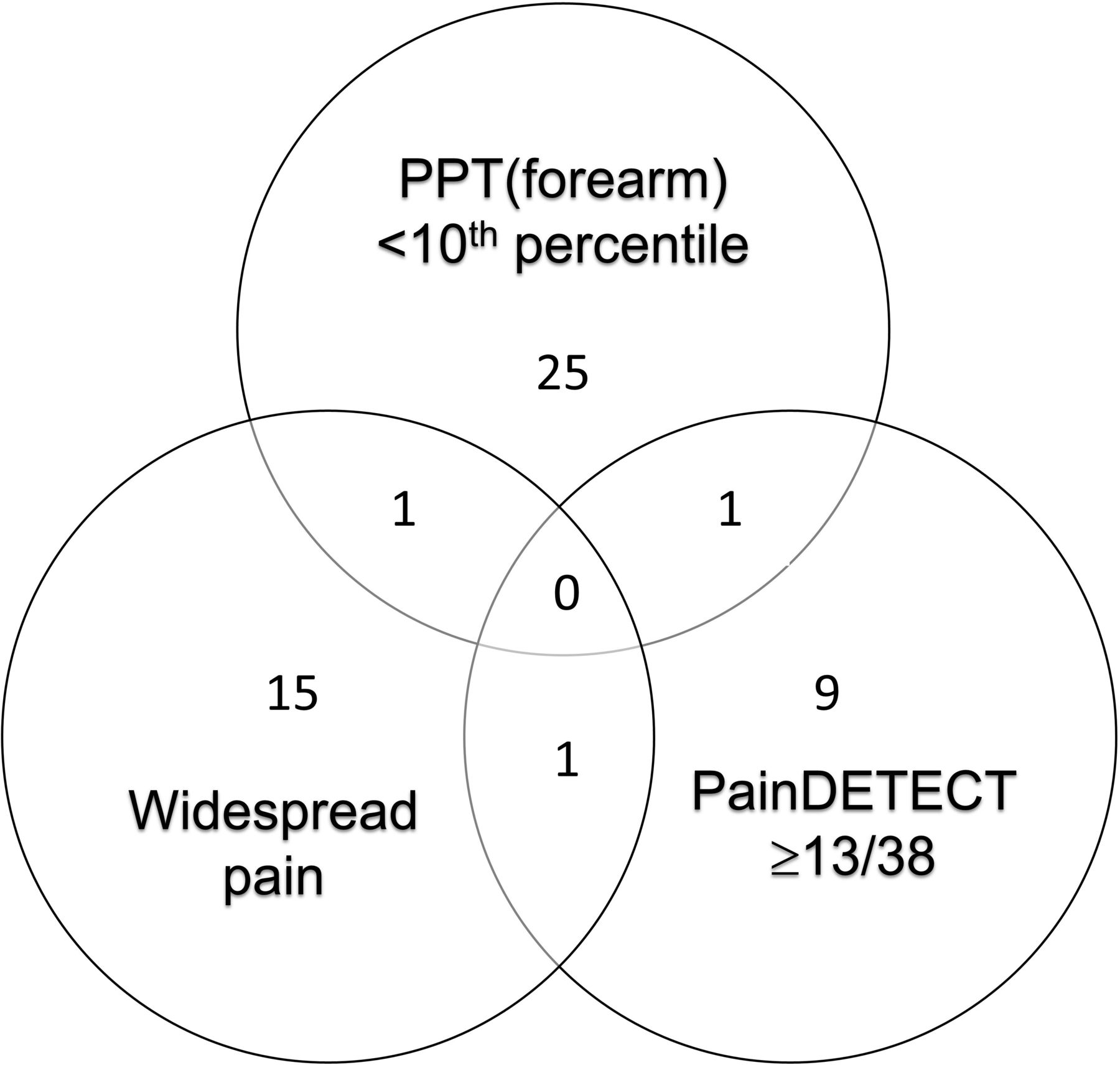
Concomitant pain sensitisation was identified in 17 patients (7.3%) using the widespread pain criteria, 27 patients (11.6%) based on PPTarm and 11 patients (4.7%) by PainDETECT (≥13/38) (table 3). Applying the three classification criteria sets identified different groups of pain sensitisation patients. There was no patient who fulfilled all three sets of pain sensitisation criteria. There were only 1, 1 and 1 patients that were classified as having pain sensitisation using PainDETECT and PPTarm; widespread pain and PainDETECT and widespread pain and PPTarm, respectively (figure 1).
{kind=link}
Venn diagram showing the number of patients with pain sensitisation as classified by three criteria sets. PPT, pressure pain threshold.
Regardless of the criteria used to define pain sensitisation, patients with concomitant pain sensitisation reported worse pain, function and QoL compared with patients without pain sensitisation (table 2). The impact of pain sensitisation on pain, function and QoL differed according to the criteria used to define pain sensitisation. Patients with concomitant pain sensitisation classified by low PPTarm had poorer WOMAC function and general health compared with patients without the phenotype. The impact of pain sensitisation in patients with concomitant pain sensitisation as classified by PainDETECT and widespread pain criteria was more diverse. Patients with widespread pain had higher WOMAC pain, worse RP, BP and MCS compared with patients without widespread pain. Patients with possible neuropathic pain (PainDETECT ≥13/38) had poorer WOMAC pain and function, worse PF, VT, MH and MCS compared with patients with KOA alone (table 2).
Comparison of pain, function and quality of life in patients with knee osteoarthritis with or without central sensitisation
Associations of pain sensitisation with pain, impact and QoL outcomes
There were weak correlations between the different measurements of pain sensitisation. The Spearman’s rho correlation between PainDETECT and number of painful body sites was 0.23 (p<0.001). However, there were no statistically significant correlations between PPTarm and PainDETECT (rho=−0.02, p=0.77); and PPTarm and number of painful body sites (rho=−0.09, p=0.16) (online supplemental table 1).
Supplemental material
In the univariable analysis, there were statistically significant associations with the different criteria used to define pain sensitisation and the outcome measures of pain, function and QoL, with the exception of PPTarm and WOMAC pain; and also number of painful body sites and PCS (online supplemental table 1). No statistically significant difference was observed between sex in the comparison of pain sensitisation identified by PPTarm, PainDETECT scores or widespread pain.
In the multivariable analysis, PPTarm was only statistical significantly associated with PCS after adjustment for age, sex, ethnicity, education level, BMI, radiographic osteoarthritis severity using KL grading and comorbidities. PainDETECT and number of painful body sites were associated with more extensive impact and QoL scores. PainDETECT was statistical significantly associated with WOMAC pain, WOMAC function, PCS and MCS. Number of painful body sites was associated with WOMAC pain, WOMAC function and MCS (table 3).
Multivariable analysis of associations between measurements of pain sensitisation and QoL outcomes
Discussion
This study found associations between measures of pain sensitisation with pain, function and QoL in patients listed for knee arthroplasty due to KOA, with patients who had concomitant pain sensitisation and KOA reporting poorer QoL compared with those without, regardless of how pain sensitisation was classified. Interestingly, identification of pain sensitisation through the three classification methods yielded different groups of pain sensitisation patients. The widespread phenotype had more pain, poorer physical function and may predict poorer QoL.
Evidence from numerous studies have suggested that pain sensitisation is present in patients with KOA compared with healthy controls, which may be associated with KOA symptom severity.7 33 However, fewer studies have evaluated the association of QoL with the concept of pain sensitisation measured by different modalities in KOA. Our current study adds to the existing literature by affirming the association of pain sensitisation and QoL in KOA. Specifically, we demonstrated the added burden on pain, function and QoL by concomitant pain sensitisation in KOA. Using the same widespread pain concept, a previous study demonstrated that patients with KOA with widespread pain had lower scores in the Knee Injury and Osteoarthritis Outcome Score and performed more poorly in the stair climb test.11 In another smaller study in KOA, using the PainDETECT and DN4 questionnaires (both developed for measuring neuropathic pain), patients with concomitant pain sensitisation had poorer SF-36 domains scores.34 There is evidence that pain sensitisation may modify the perception of pain intensity in KOA, with patients who have limited chronic pain modulation response reporting greater limitations.35
There are a variety of instruments available for the assessment of the concept of pain sensitisation, yet none of these measures is directly measuring the underlying ‘construct’.15 Pain sensitisation remains a complex pathophysiological phenomenon with possible changes at both spinal and brain levels. The International Association for the Study of Pain defined sensitisation as an increased responsiveness of nociceptive neurons in the central nervous system to their normal or subthreshold afferent input.36 Recently, the term nociplastic pain is proposed as a mechanistic descriptor for chronic pain states not characterised by obvious activation of nociceptors or neuropathy, ‘but in whom clinical and psychophysical findings suggest altered nociceptive function’.37 Nonetheless, the mechanistic understanding of these constructs remains incomplete. Few studies have directly compared different criteria for defining pain sensitisation in patients with KOA. In our study, we compared three different methods and criteria in the assessment of pain sensitisation and found that the methods identified different patients. There were minimal overlaps in patients identified by these methods, and there were disparities in the effect of pain sensitisation on impact and QoL between the three groups. There was only mild correlation between PainDETECT and widespread pain, while there was no significant correlation with the above to PPTarm. It may indicate that these instruments are measuring slightly different construct. We have shown that among patients with KOA listed for arthroplasty, PainDETECT and number of painful body sites were associated with a wider spectrum of impact and QoL impairment, including vitality, psychological and mental aspects compared with those without the phenotype. Whereas PPTarm was associated with only physical function after adjustment of demographic variables. The lack of correlation between QST measures and widespread pain with scores from the Central Sensitisation Inventory (CSI) have been shown previously.10 Moore et al explored the relationship of various modalities and demonstrated only fair to moderate correlations between QST measures and clinical measures of pain sensitisation.38 Compared with PainDETECT and a painful body chart completed by patients, a manual tender point count administered by a physician had the strongest associations with QST measures and accounted for 11%–12% of the variance in PPTs measured from six body sites. In another study in KOA, PPTarm was weakly correlated with CSI (rho=−0.24, p<0.05), but not statistically significantly correlated with modified PainDETECT.39 Identifying patients with the phenotype of pain sensitisation or nociplastic pain remains challenging and limits progress in the identification and evaluation of targeted treatment modalities for patients with KOA with the phenotype. PROs, or QST may be helpful in assisting clinicians to identify a nociplastic pain phenotype, yet further studies are required to develop standardised protocols for the assessment of pain sensitisation that can be applied in a clinical setting, and define clear cut-offs and criteria for the identification of pain sensitisation phenotypes that would affect disease burden and outcomes of interventions. In the meantime, clinical assessment remains critical to identify possible pain sensitisation or nociplastic phenotype. This would entail a comprehensive history taking and physical examination, paying attention to the characteristic of pain, particularly those with neuropathic qualities such as pain at rest, shooting in nature and intense severity on tactile triggers. It is equally important to explore associated fatigue, cognitive problems, sleep problems, multiple environmental sensitivities and psychological symptoms.37
Strengths of the study include its relatively large sample size for a QST study and use of validated PRO measures. One trained and designated staff personnel assessed PPTs and demonstrated good test–retest reliability.21 However, the study has limitations. First, this was a post hoc analysis of baseline cross-sectional data from a cohort of patients undergoing arthroplasty, and therefore inferences about causality cannot be drawn. We did not evaluate the impact of concomitant pain sensitisation on patient outcomes after arthroplasty. Second, there may be other variables that may affect pain sensitisation and QoL that we have not adjusted for in the models, such as concomitant osteoarthritis of other joints, the control of comorbidities and the use of pain killers on the day of assessment and other psychosocial variables. Third, despite preliminary effort, none of the instruments has been comprehensively validated for the identification of pain sensitisation in patients with KOA. None of the instruments is direct measurement of the underlying construct. We are cognizant of the possibility that patients classified as having widespread pain may represent polyarticular osteoarthritis and not necessarily be related to sensitisation. On the other hand, PainDETECT is a measurement of neuropathic pain. A smaller study has tried to validate it in KOA against multiple QST modalities, yet the sensitivity and specificity of the proposed cut-off was not adequately robust.27 The cut-offs for the different classifications for concomitant pain sensitisation in the current study were arbitrary, which may have influenced the findings. Finally, the absolute number of patients who met any one of the criteria for ‘pain sensitisation’ was quite small, which may have impacted our findings. A low prevalence of neuropathic-like phenotype has been reported in other Asian cohorts.40 41 Perhaps, a certain proportion of patients with KOA who have pain sensitisation may have been excluded from offering arthroplasty during clinical assessments. The results may not be generalisable to patients with earlier stage and milder KOA.
In conclusion, we have shown that the degree of pain sensitisation in KOA is closely associated with pain, function and QoL. Patients with KOA who have concomitant pain sensitisation have poorer pain, function and QoL compared with those without regardless of how pain sensitisation was classified. This highlights the important impact that concomitant pain sensitisation can have on pain, function and QoL among patients with KOA.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was approved by Singhealth Central Institution Review Board (CIRB Ref 2014/2010E) and all patients provided informed, written consent prior to participation.
Acknowledgments
The study team is grateful to Ms Shuqin Xiong (SX) who was trained and committed to measurement of PPT in all participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors YYL designed research; YYL, S-JY and SBW conducted research; YYL and NM-YA analysed data; YYL and NM-YA drafted the paper. All authors critically reviewed and approved the final manuscript. YYL accepts full responsibility and acts as the guarantor to the work.
Funding This study was supported by the Khoo Pilot award of the Duke-NUS Medical School, Singapore (DUKE-NUS-KP/2014/0016). YYL was supported by the National Medical Research Council, Singapore (NMRC/CSA-Inv/0022/2017).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.