Article Text

Abstract
Objective Studying vertebral bone loss in radiographic axial spondyloarthritis (r-axSpA) has been challenging due to ectopic bone formation. We cross-sectionally analysed low-dose CT (ldCT) trabecular bone density Hounsfield units (HU) measurements and calculated inter-reader reliability at the vertebral level in patients with r-axSpA.
Methods LdCT scans of 50 patients with r-axSpA from the sensitive imaging in ankylosing spondylitis study, a multicentre 2-year prospective cohort were included. Trabecular bone HU taken from a region of interest at the centre of each vertebra (C3-L5) were independently assessed by two trained readers. HU mean (SD), and range were provided at the vertebral level, for each reader and centre separately. Inter-reader reliability and agreement were assessed using intraclass correlation coefficients (ICC; single measurements, absolute agreement, two-way mixed effects models); smallest detectable difference and Bland-Altman plots.
Results Overall, 1100 vertebrae were assessed by each reader. HU values decreased from cranial to caudal vertebrae. For readers 1 and 2 respectively, the highest mean (SD) HU value was obtained at C3 (354(106) and 355(108)), and the lowest at L3 (153(65) and 150 (65)). Inter-reader reliability was excellent (ICC(2,1):0.89 to 1.00). SDD varied from 4 to 8. For most vertebrae, reader 1 scored somewhat higher than reader 2 (mean difference of scores ranging from −0.6 to 2.9 HU). Bland-Altman plots showed homoscedasticity.
Conclusion LdCT measurement of HU is a feasible method to assess vertebral bone density in r-axSpA with excellent inter-reader reliability from C3 to L5. These results warrant further validation and longitudinal assessment of reliability.
- ankylosing spondylitis
- bone density
- Outcome Assessment, Health Care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about this subject?
Studying vertebral bone loss in radiographic axial spondyloarthritis (r-axSpA) has been proved challenging due to imaging limitations.
Low-dose CT (ldCT) allows the whole spine assessment with acceptable levels of radiation exposure and avoiding ectopic bone formation; however, the use of ldCT for the assessment of vertebral bone loss in r-axSpA has never been studied.
What does this study add?
The ldCT measurement of Hounsfield units (HU) is a feasible method for assessing bone density at the vertebral level in patients with r-axSpA, lower values of HU representing a lower ldCT attenuation and, therefore, less-dense bones.
Inter-reader reliability and agreement of HU measurements on ldCT was good to excellent, at the vertebral level, from C3 to L5.
How might this impact on clinical practice or future developments?
LdCT vertebral HU (continuous score) may be used as a surrogate for bone density and aid the future research into bone loss throughout the whole spine.
Introduction
Radiographic axial spondyloarthritis (r-axSpA), traditionally known as ankylosing spondylitis, is a chronic inflammatory disease affecting the spine and sacroiliac joints.1 Bone disease in r-axSpA is a complex phenomenon in which bone formation and bone loss paradoxically coexist, both contributing to the morbidity of the disease.2
Studying bone disease in r-axSpA, and particularly bone loss, has been proved challenging due to imaging limitations.3 4 The most appropriate and valid method to assess bone mineral density (BMD) in patients with r-axSpA is still unclear.3 Dual-energy X-ray absorptiometry (DXA) is considered an accurate, repeatable and quantitative 2D method to assess BMD at the spine and hip, with a low dose up to less than 1 μSv.5 Notwithstanding, new bone formation and aberrant hyperostosis may artificially increase BMD of the spine.3 New imaging techniques for measuring BMD at the vertebral level have emerged in the past years.6 Quantitative CT, a 3D technique, has been shown to estimate trabecular vertebral BMD avoiding the ectopic osteoproliferative changes.6 7 However, QTC requires special settings for imaging acquisition, with high ionising radiation exposure.8 Therefore, studies included only a few vertebrae mainly at the lumbar spine.9 10 The use of ldCT to study bone loss in r-axSpA has not been evaluated in the literature.
Assessing local bone quality on CT scans with Hounsfield units (HU) quantification is being increasingly reported. HU allow for the assessment of tissue density on CT, based on a defined scale of zero for water and −1000 for air. The upper HU limits can reach more than 3000 for metals like steel or silver, while bone typically ranges from 300 up to 2000 HU for dense bones like cochlea.11 Modern imaging software programmes allow HU to be calculated from a region of interest on CT scans without any additional cost or radiation exposure. Several studies opportunistically assessed vertebral HU in trauma patients, general population or patients with CT scans performed for other reasons,11–16 including the lumbar spine in patients with r-axSpA.10 Correlations between HU and BMD (as measured by DXA) have been established, and normative data have been defined throughout the spine.11 14 However, the thorough assessment of HU from the cervical to the lumbar spine has never been made, mainly due to high radiation exposure issues.
Low-dose CT (ldCT), using acceptable levels of ionising radiation exposure (as low as 1.4 mSv for whole spine ldCT), has been hypothesised as the ideal imaging technique to study bone changes in r-axSpA.3 17 18 Major advances in the understanding of new bone formation in r-axSpA have been accomplished using ldCT scans of the whole spine. New bone formation in the spine of patients with r-axSpA can be reliably assessed using CT Syndesmophyte Score on ldCT with high sensitivity for syndesmophyte formation.19 20 Another advantage of using ldCT scans is that, as in conventional CT scans, vertebral HU can potentially be measured.14
In the present study, we aimed to cross-sectionally describe the ldCT measurements of HU, as a surrogate for bone density, and their inter-reader reliability at the vertebral level from C3 to L5 in patients with r-axSpA.
Material and methods
Study design and study population
This was a cross-sectional study using data from patients with r-axSpA included in the sensitive imaging in ankylosing spondylitis (SIAS) cohort. SIAS was a multicentre 2-year prospective cohort, including 60 patients with r-axSpA from two centres: Leiden, the Netherlands and, Herne, Germany. The main purpose of this cohort was to assess the role of new sensitive imaging techniques in r-axSpA. Patients were consecutively included according to the following criteria (recruitment period from 2010 to 2012): age ≥18 years; a diagnosis of r-axSpA, fulfilling the modified New York criteria21; 1–18 syndesmophytes (maximum of 75% of the possible sites) visible on lateral cervical and lumbar spine conventional radiographs and ≥1 inflammatory lesion on short tau inversion recovery MRI of the whole spine. Clinical and spine MRI data were obtained at baseline, 1 and 2 years, while ldCT scans of the whole spine were performed at baseline and after 2 years of follow-up. For the present study, a sample of 50 baseline ldCT scans was used, according to a sample size calculation focused on the reliability and considering an intra-class correlation coefficient (ICC) of ≥0.80 as acceptable.22 The sample size calculation details and respective formula are provided in online supplemental text S1.
Supplemental material
HU imaging assessments
LdCT imaging acquisition using automatic exposure control calibration was performed in both centres in accordance with a standardised protocol. In Leiden, the ldCT scanner used was a Aquilion 64 (Toshiba Medical Systems), while, in Herne, a Somatom Emotion 16 (Siemens) was used; the effective dose estimates for the whole spine were 3.8 (2.6) mSv and 4.7 (2.4) mSv per ldCT, respectively. The differences in ionising radiation exposure between 16-slice and 64-slice scanners, for a similar-sized patient (ie, CTDIvol), were approximately 10%, the 64-slice scanner involving less ionising radiation exposure. Differences between the radiation doses of the two scanners may be explained not only by the scanner settings and performance, but also by the area scanned (greater on the 16-slice scanner).
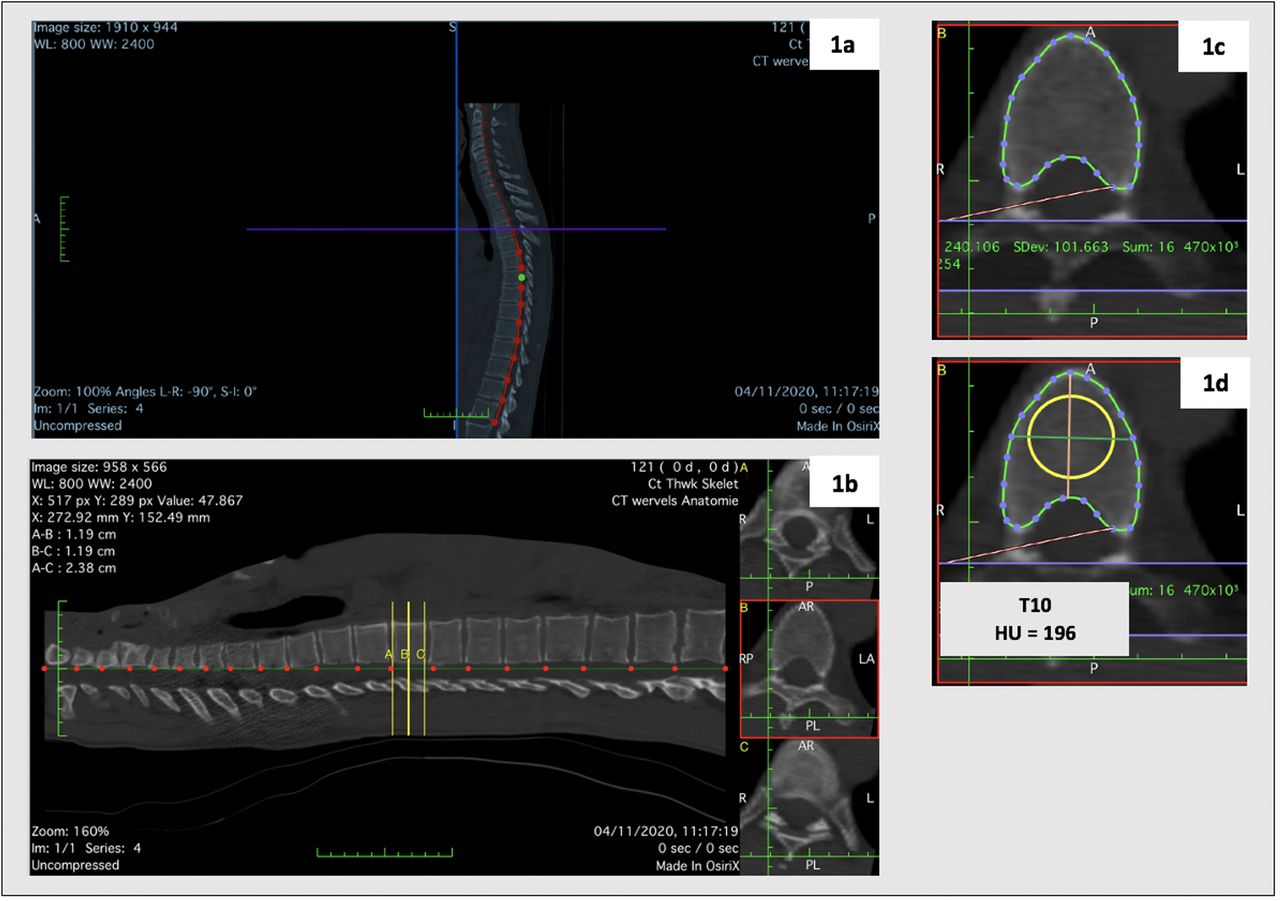
Vertebral ldCT HU (continuous score for the whole vertebra) were independently assessed at the vertebral level from C3 to L5 by two trained readers (a radiologist and a rheumatologist) using OsiriX software (v6.5.1). A recent methodology validated in trauma patients was adapted in an iterative process for the whole spine.14 Briefly, using a three-dimensional curved-multiplanar reconstruction (3D Curved-MPR), each vertebral level was identified on a sagittal plane. Vertebral HU measurements were taken from a reconstructed cross-sectional slice positioned at the centre of the vertebra. The mean HU value obtained at each vertebra corresponded to the average image density within a selected region of interest avoiding the peripheral bone. A detailed description is provided in figure 1.
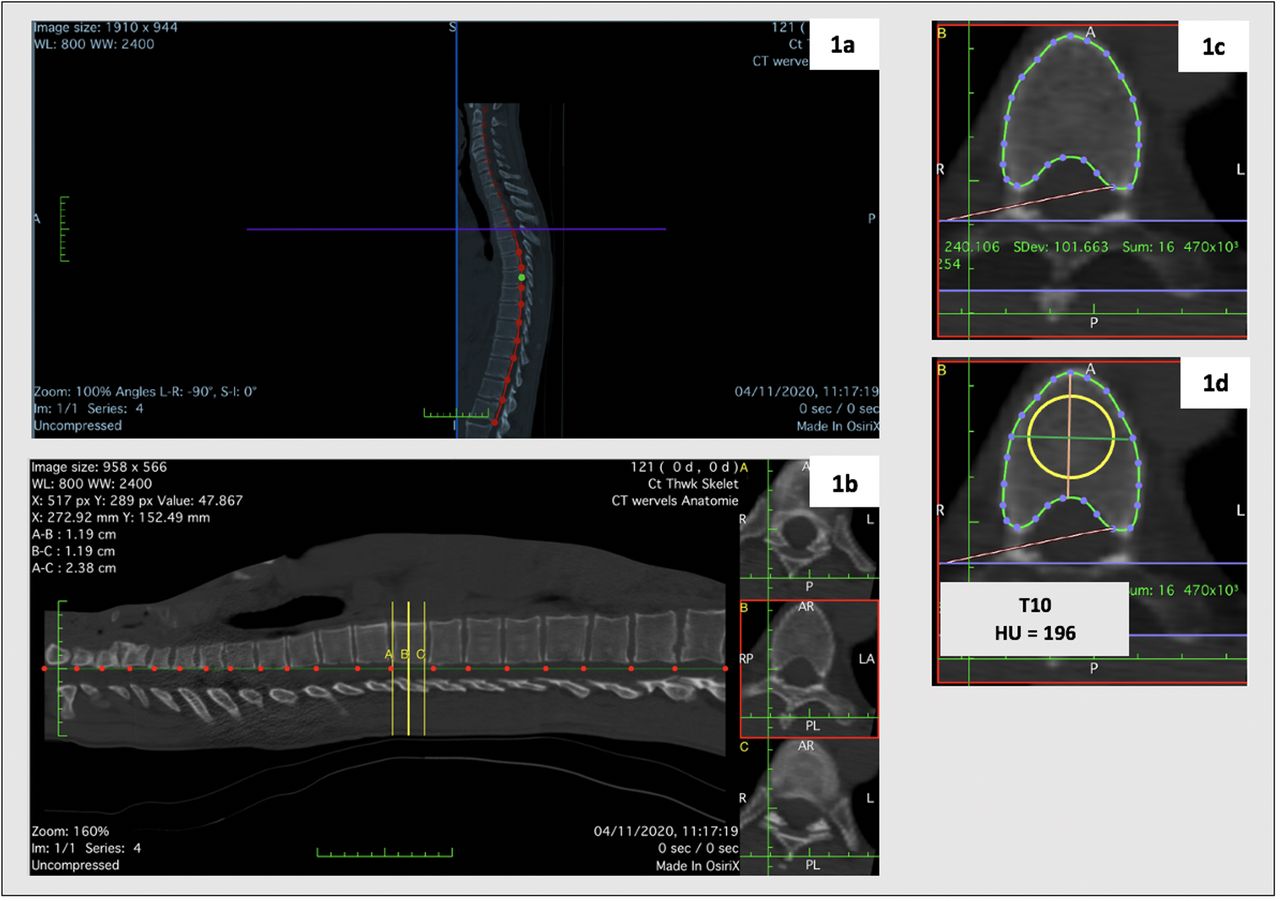
Methodology of Hounsfield Units (HU) measurement. (A) Using a three-dimensional curved-multiplanar reconstruction (3D Curved-MPR) the curve of the spine adjacent to the spinal canal was selected. (B) On the obtained sagittal image, the individual vertebral levels were identified. The software automatically displays three lines of reference (yellow lines A, B and C). At each vertebral level, two lines of reference were manually positioned at the superior (yellow line A) and inferior (yellow line C) limits of the vertebra. Equidistant to A and C, the yellow line B was automatically placed by the software at the centre of the vertebral body. (C) Vertebral HU measurements were taken from a single reconstructed cross-sectional slice positioned at the centre of the vertebra (at the level of the yellow line B). (D) A centred region of interest (ROI) was manually selected, having a diameter equal to 75% of the average of anteroposterior and transverse diameters. The density of the vertebra was displayed by the software as the average image intensity within the sample region, reported in HU.
Statistical analysis
Baseline data were analysed at the vertebral level. The entire spine was analysed (C3-L5; 22 vertebrae per patient), which allowed using a maximum of 1100 vertebrae in 50 patients. Mean (SD) and range for HU were provided at the vertebral level, for each of the readers and for each centre separately (Leiden vs Herne). The number and type of incident density abnormalities or artefacts were also described.
Reliability and agreement of HU measurements at the vertebral level
Inter-reader reliability and agreement were assessed at the vertebral level. ICCs single measurements, absolute agreement were used, applying two-way mixed effect models.23 The reader was defined as fixed (only applicable to the readers of the present study and not aiming at generalising the results to other studies), and the patients/vertebral levels were defined as random. Agreement was assessed using Bland-Altman plots and the smallest detectable difference (SDD=1.96 × SDdifference /(√k)). SDdifference is the SD of the differences in status scores between two readers and k is the number of readers (n=2).24
Intra-reader reliability was assessed in a 20% random sample (n=10 patients; n=220 vertebrae). Reader one reassessed the ldCT scans in a different session at least 1 week after the first assessment. Two-way mixed effects models, absolute agreement, were used to compute ICCs. Agreement was assessed using Bland-Altman plots and SDD. The SDD formula was the same as above, though the SDdifference is the SD of the differences in status scores between the two assessments performed by the same reader, and the K stands for the number of assessments (k=2).
Statistical analyses were performed using STATA software V.14.0.
Results
Whole spine ldCT scans from 50 patients with r-axSpA (mean (SD) age of 49 (10) years; 43 (86%) male and 42 (84%) HLA-B27 positive) were included – 26 of them from Leiden, and 24 from Herne. Detailed information regarding demographic and clinical characteristics of the included patients is provided in online supplemental table S1.
Of the 1100 vertebrae, 1053 (96%) could be assessed for HU measurements. Severe ankylosis precluded the assessment of a maximum of 47 vertebrae (most of them (n=30) at the cervical spine). In total, 220 cervical, 588 thoracic and 245 lumbar vertebrae were assessed by each reader.
The HU values decreased from cranial to caudal vertebrae. The gradient of decreasing values from the cervical to the lumbar vertebrae is shown in table 1. For both readers, the highest mean (SD) value for HU was obtained at C3 (354 (106) and 355 (108) for readers 1 and 2, respectively), and the lowest at L3 (153 (65) and 150 (65) for reader 1 and 2, respectively). Remarkably, when analysing the results separately for the two centres included in this study (Leiden vs Herne), the same gradient and similar HU values were observed throughout the spine—online supplemental table S2.
Descriptive statistics of Hounsfield units (HU) values according to the measurements of readers 1 and 2, inter-reader reliability and agreement for each vertebral level
Only 7% of the vertebrae (n=72) were reported by at least one of the readers as having density abnormalities or artefacts that affect the HU measurement. The most frequent artefact was the presence of sclerotic changes affecting the vertebral body (n=31, 43%). Photon starvation artefact was reported as the second most common limitation to the HU measurement (n=18, 25%), typical at the shoulder level. No osteosynthesis material or other visible foreign material were detected in the assessed vertebrae. A detailed description of the total artefacts at the vertebral level is provided in online supplemental table S3.
Reliability and agreement of HU measurements at the vertebral level
Inter-reader reliability was shown to be excellent, with ICCs ranging from 0.90 to 1.00 in the cervical spine; 0.97 to 1.00 in the thoracic spine; and 0.89 to 0.94 in the lumbar spine (table 1). SDD varied, throughout the whole spine, from 4 to 8. A small degree of systematic error was observed between the two readers, that is, for most vertebrae, reader 1 scored somewhat higher than reader 2 (mean difference of scores ranging from −0.6 HU to 2.9 HU). Bland-Altman plots showed homoscedasticity throughout the whole spine. Representative examples from vertebrae of each segment of the spine (C3, T1 and L1) are presented in figure 2. The Bland-Altman plots for all the other vertebral levels are provided in online supplemental figures S1-S19.

{kind=link}
{kind=link}
Bland-Altman plots for representative examples from vertebrae of each segment of the spine: C3, T1, and L1. The scatter of differences is homoscedastic. HU, Hounsfield Units.
Intra-reader reliability was also excellent. Descriptive statistics for the HU repeated measurements, ICCs and SDD are provided for each vertebra in online supplemental table S4. ICCs varied from 0.92 to 1.00, while SDD ranged from 2 to 6 throughout the spine. Bland-Altman plots showed homoscedastic scatter throughout the spine, with mean differences of the two assessments close to zero HU – representative examples are given in online supplemental figure S20.
Discussion
In this study, we cross-sectionally tested a methodology for assessing bone density of the whole spine in patients with r-axSpA, using vertebral HU measured on ldCT scans. HU measurements were proven to be feasible with excellent inter-reader reliability at the vertebral level, from C3 to L5.
LdCT HU values were higher in the cervical vertebrae and decreased throughout the spine, with the lowest values obtained for the lumbar vertebrae. Lower HU values represent a lower ldCT attenuation. Thus, less-dense bones will likely have lower HU values. The gradient of HU is also in line with previous results in different populations (trauma patients or general population),14 15 25 and with findings in histomorphometry analysis of intervertebral variation in trabecular microarchitecture throughout the normal spine.26 The analysis of excised vertebral bodies of the complete spine (C3 to L5) in 26 autopsy cases revealed a significant intervertebral variation of trabecular microarchitecture.26 The density of the trabecular structure of cervical vertebrae was shown to be much higher than that of thoracic and lumbar vertebrae.26 Remarkably, the structural differences between lumbar spine at one end and cervical spine on the other end of the spine were shown to increase with age, bone mass decreasing faster caudally than cranially within spinal vertebrae.26 The rationale behind these differences, although poorly studied, might be due to the high dynamic forces of which cervical vertebrae are exposed to because of their mobility and small size.26
Notwithstanding, in the present study, the vertebral HU values for patients with r-axSpA were on average, and for all spinal segments, lower than what was previously presented in stratified data for similar age and gender general populations.14 15 25 These results may indicate that, in r-axSpA, bone loss is likely locally present throughout the whole spine and not predominantly in the lumbar spine, the latter more consistent with biological systemic bone loss. Although data in other fields suggested that low-dose and standard CT scans yield equivalent HU measurements,27 caution is needed when comparing HU measured by different CT techniques.
Negative HU values were observed in seven vertebrae, corresponding to two patients in which medullar fat infiltration was present. These vertebrae likely do not have a major influence on the lower mean HU values. On the contrary, sclerotic lesions, were rather more frequent throughout the spine and could have slightly falsely increased the HU. In the current analysis, we decided not to exclude vertebrae with artefacts, as those are relevant for the reliability analysis.
A recent meta-analysis tested the diagnostic accuracy of HU on CT scans relative to DXA for the diagnosis of osteoporosis in spine surgery populations.28 In patients with mean age around 60 years or more, a threshold of 135 HU (or below) to diagnose lumbar osteoporosis was proposed. Notwithstanding, a large heterogeneity between studies was observed warranting caution in the interpretation of these results. In the present study, and differently from previous studies,11–15 25 we aimed at assessing bone loss as a local phenomenon, at the vertebral level, and not as systemic bone loss. Thus, the validation of this technique against a gold standard for the diagnosis of osteoporosis, namely DXA, was not within our aims. Indeed, in SIAS cohort, in which syndesmophytes are largely prevalent at baseline,19 using DXA as a gold standard for osteoporosis (bone loss) definitions imposes caution.3 4 Bone loss would expectedly be underreported in DXA measurements and the correlation between DXA BMD and ldCT HU would, by concept, be inaccurate. Combining QTC with ldCT may be a potential way for future validation of these results.3 8
In our study, while inter-reader ICC values were excellent (ICC:0.89 to 1.00), these values may be spuriously high due to the large spread of the HU values. Therefore, besides ICCs, Bland-Altman plots, and SDD, are important to take into consideration. Bland-Altman plots were homoscedastic, with mean differences of the two readers’ scores close to zero HU. Moreover, SDD values, which ranged between 4 and 8, were relatively small in comparison to the full range of HU values. Intra-reader reliability and agreement (although assessed in a small sample) were excellent. Taken together, these results encourage the future use of ldCT HU measurements to aid the research of bone loss as a local pathological phenomenon in patients with r-axSpA.
This study has several strengths. First, the use of a technique which allows the comprehensive assessment of the whole spine using low ionising radiation exposure (the effective dose estimates were around 4 to 5 mSV per ldCT in SIAS,19 but are currently estimated to be as low as 1.4 to 1.7 mSV per ldCT using technical optimisation in the 64-slice scanners), without noticeable imaging quality loss. The use of automatic exposure control as a calibration method to produce identical imaging quality, may have resulted in more accurate HU values of the targeted tissue than the traditionally used phantom calibration.11 29 Also, the measurement of HU within the trabecular bone, avoided artificially increased values due to peripheral ectopic bone formation. This technique was shown to have excellent agreement and inter-reader reliability as assessed by a comprehensive statistical methodology, being feasible and easy to be applied by others than radiologists within a limited number of hours of training. The multiplanar nature of ldCT assessments allow increasing accuracy and repeatability of HU measurements in a specific region of interest even in patients with severe kyphosis when compared with anteroposterior DXA measurements. Despite the use of different CT scanners (16- and 64-slice CT), the HU values in the reconstructed images for each vertebral level were within similar ranges for both centres. The latter adds to the generalisability of our findings and may imply less concerns regarding previously reported issues in matching automatic exposure control parameters among scanners from different CT manufacturers.29 However, short- and long-term precisions are important, particularly, in a method which uses reconstructed images in different equipment. The use of patients with r-axSpA recruited in different countries (the Netherlands and Germany) adds to the external validity of the present results.
The present study is not without limitations. Our methodology for HU assessment included only one slice at a given vertebra, which does not fully account for the heterogeneity of the trabecular bone.11 Notwithstanding, iterations of our methodology were performed according to that described by Schreiber et al,11 and the average HU of several slices from the same vertebra were not significantly different from the HU obtained for one slice only.14 Thus, and given the comprehensive assessment of 22 vertebrae per patient, we opted for the less time-consuming methodology. LdCT artefacts can affect HU measurements. Notwithstanding, photon starvation and beam-hardening artefacts, that correspond to the presence of streaks and dark bands generated by the shoulder girdles, leading to falsely lowered HU measurements, could likely be prevented, or later corrected in the reconstruction process.30 Some of the limitations affecting HU measurement are incidental findings such as haemangiomas or bone islands.
In summary, the newly adapted and reliable assessment of ldCT vertebral HU can, as a surrogate of bone density, aid the study of bone disease throughout the whole spine in r-axSpA without the well-known limitations of DXA,3 4 and with a lower radiation exposure relatively to CT scans.19 These results warrant further validation and longitudinal assessment of reliability.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval for the study was obtained from the institutional review board at each centre (Leiden Medisch Ethische Toetsings Commissie (METC) number: P10.021; Herne Ethikkommission der Ruhr Universität Bochum number: 4366-12). Participants gave informed consent to participate in the study before taking part. Coded data of the included patients were used.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors XB, JB, FAvG and MR performed the data collection in SIAS cohort. MLM, DvdH, SR and FAvG developed the study design. MLM and NPdS iteratively tested the methodology and independently performed all the Hounsfield Units measurements. MLM and SR prepared the dataset. MLM and SR performed the statistical analyses and synthesised the data. MLM has drafted the first version of the manuscript, and all authors have critically reviewed and agreed with the final version of the manuscript. SR is responsible for the overall content as guarantor.
Funding SIAS study was funded by the Dutch Rheumatism Association. MLM is supported by the Fundação para a Ciência e Tecnologia (FCT) grant SFRH/BD/143744/2019.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.