Article Text

Abstract
Background Psoriatic arthritis (PsA) and axial spondyloarthritis (axSpA) show certain overlaps: A subset of patients with PsA can develop axial involvement (axial PsA, axPsA), while a subset of patients with axSpA presents with psoriasis (axSpA+pso). Treatment strategy for axPsA is mostly based on axSpA evidence.
Objectives To compare demographic and disease-specific parameters of axPsA and axSpA+pso.
Methods RABBIT-SpA is a prospective longitudinal cohort study. AxPsA was defined based on (1) clinical judgement by rheumatologists; (2) imaging (sacroiliitis according to modified New York criteria in radiographs or signs of active inflammation in MRI or syndesmophytes/ankylosis in radiographs or signs of active inflammation in spine MRI). axSpA was stratified into axSpA+pso and axSpA without pso.
Results Psoriasis was documented in 181/1428 axSpA patients (13%). Of 1395 PsA patients, 359 (26%) showed axial involvement. 297 patients (21%) fulfilled the clinical definition and 196 (14%) the imaging definition of axial manifestation of PsA. AxSpA+pso differed from axPsA regardless whether clinical or imaging definition was used. axPsA patients were older, more often female and less often HLA-B27+. Peripheral manifestations were more often present in axPsA than in axSpA+pso, whereas uveitis and inflammatory bowel disease were more common in axSpA+pso. Burden of disease (patient global, pain, physician global) was similar among axPsA and axSpA+pso patients.
Conclusions AxPsA differs from axSpA+pso in its clinical manifestations, irrespective of whether axPsA is defined clinically or by imaging. These findings support the hypothesis that axSpA and PsA with axial involvement are distinct entities, so extrapolation of treatment data from randomised controlled trials in axSpA should be performed with caution.
- psoriatic arthritis
- spondylitis, ankylosing
- epidemiology
Data availability statement
Data are available on reasonable request. Applications to access the data should be made to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Axial manifestation in psoriatic arthritis (PsA) is common; however, there is no consensus in the definition of axial PsA (axPsA).
WHAT THIS STUDY ADDS
Our data indicate that patients with axPsA are different from ‘typical’ axial spondyloarthritis (axSpA), even if axSpA patients with psoriasis are used as a comparator. The observed differences between axPsA and axSpA in our cohort were similar regardless of whether a clinical or an imaging-based definition of axial involvement was used.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Extrapolation of the evidence derived from trials in axSpA patients to axial manifestations in PsA should be done with caution.
Introduction
Under the umbrella term spondyloarthritis (SpA), a group of chronic inflammatory diseases including axial spondyloarthritis (axSpA), psoriatic arthritis (PsA), reactive arthritis, inflammatory bowel disease (IBD) related SpA and undifferentiated SpA are subsumed.1 2 These diseases share common features like back pain, peripheral arthritis, enthesitis, dactylitis as well as extramusculoskeletal manifestations like acute anterior uveitis, IBD and skin psoriasis (pso). All forms of SpA are associated with the human leucocyte antigen (HLA)-B27, although to a variable degree. AxSpA and PsA are the most common diseases within the SpA spectrum and show a certain overlap in their clinical features. Therefore, differentiation between axSpA and PsA can sometimes be challenging but might have an impact on treatment choice.
While in axSpA inflammatory back pain (IBP) is the leading clinical symptom, in PsA oligoarthritis or polyarthritis and enthesitis are the most common musculoskeletal symptoms together with skin and nail involvement, but axial manifestation can also be present.
The classification criteria for axSpA (Assessment of Spondyloarthritis international Society (ASAS) classification criteria)3 and for PsA (Classification criteria for Psoriatic Arthritis (CASPAR) criteria)4 share symptoms like presence of arthritis, enthesitis, psoriasis or dactylitis. Therefore, patients can fulfil both classification criteria sets.5 Specific classification criteria for axial PsA (axPsA) have not yet been defined and this has been identified as an important unmet medical research question.6 The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) and ASAS have initiated a cross-sectional study (AXIS study, NCT04434885) with the main aim to develop classification criteria and a unified nomenclature for axial involvement in PsA in order to better define axPsA.7
Whether data and insights from axSpA with concomitant psoriasis can be extrapolated to axPsA is an ongoing debate. Differences between axSpA and axPsA in age, sex, HLA-B27 positivity and imaging results have been described.8 9 For example, in axPsA radiographic sacroiliitis was more frequently unilateral and less severe than in axSpA.5 8 10
Treatment strategies for the axial domain of PsA are mostly based on evidence generated for axSpA, as only little clinical trial data for axPsA exist.9 11 12 Before specific treatment recommendations for axial involvement in PsA can be set up, it is important, to define the axial manifestations more clearly. Therefore, the aim of this analysis was to compare axPsA with axSpA patients with concomitant psoriasis from the German disease register RABBIT-SpA,13 which includes patients with both axSpA and PsA.
Methods
The German disease register RABBIT-SpA is a prospective longitudinal observational multicentre cohort study in Germany, which started in 2017. Patients diagnosed by the treating rheumatologist either with axSpA or PsA initiating a new treatment with a biological disease-modifying antirheumatic drug (bDMARD), targeted synthetic DMARD or a conventional systemic treatment (DMARD and/or nonsteroidal antiinflammatory drugs (NSAID)) can be included. After enrolment, data are collected after 3 and 6 months, and then every 6 months covering physician and patient reported parameters. Both entities are recruited in the same centres.
The electronic case report forms (eCRF) for axSpA and PsA share many items but differ in some disease specific variables. For example, the axSpA eCRF includes ASAS-classification criteria, Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functioning Index (BASFI) and spine mobility. The PsA eCRF includes CASPAR criteria, skin parameters like affected body surface area, and Dermatology Life Quality Index.
We used two different definitions of axPsA, the clinical definition and the imaging definition. The clinical definition was fulfilled if the treating rheumatologist documented axial manifestation in the eCRF. The imaging definition was fulfilled if there was a sacroiliitis according to modified New York criteria (mNYc) in radiographs or signs of active inflammation in MRI of sacroiliac joint (SIJ) or presence of syndesmophytes or ankylosis in radiographs of the spine or signs of active inflammation in MRI of the spine if performed in routine care and recorded by a rheumatologist.
AxSpA patients were stratified into axSpA+pso (with psoriasis in either patient history or present) and axSpA (without psoriasis).
Imaging changes were defined as: radiographic signs (sacroiliitis according to mNYc or presence of syndesmophytes or ankylosis) or typical signs in MRI (active inflammation of SIJ or of the spine). Asymmetrical sacroiliitis was defined as ≥2 grade difference in sacroiliitis in left or right SIJ.
All patients fulfilling inclusion criteria were included in this cross-sectional analysis. Baseline parameters of axSpA+pso patients and axPsA patients were compared by using Student’s t-test for continuous variables or Mann-Whitney U test for categorical variables. P values <0.05 were considered statistically significant. Database closure was 1 March 2022.
Results
Description of cohort
A total of 2823 patients were included in this analysis, 1428 in the axSpA cohort and 1395 in the PsA cohort (figure 1). Mean age was 44 years in axSpA and 52 years in PsA, 45% of the axSpA and 59% of the PsA patients were female. Psoriasis was documented in 181 of 1428 axSpA patients (13%). Of 1395 PsA patients, 359 patients (26%) showed axial involvement. A total of 297 patients (21%) fulfilled the clinical definition and 196 (14%) the imaging definition of an axial manifestation of their PsA (figure 1).

Flow chart of included patients. axSpA, axial spondyloarthritis; PsA, psoriatic arthritis.
Table 1 shows the distribution of the patients according to the different definitions used to define axial manifestation. Of the 297 PsA patients fulfilling the clinical definition of axial manifestation, 45% also fulfilled the imaging definition, 30% did not fulfil the imaging definition and in 25% imaging examinations were not undertaken. In the 1098 patients without clinical axial manifestation, 6% fulfilled the imaging definition, 27% had undergone an imaging examination but did not fulfil the imaging definition and in 67% imaging examinations were not undertaken.
Cross-table of intersection of clinical respectively imaging defined axPsA
On the other hand, clinical axial manifestation was negated in 32% of the 196 patients fulfilling the imaging definition (table 1). Of the 384 patients not fulfilling the imaging definition, 23% fulfilled the clinical definition. 90% of patients in which imaging examination has not been performed did not show any clinical sign of axial manifestation.
There were minor differences between axSpA patients with psoriasis (axSpA+pso) in comparison to those without psoriasis (table 2). Age was higher and disease duration was slightly longer in axSpA+pso and CRP was less often elevated. AxSpA+pso patients were more often obese (body mass index ≥30 kg/m2) (33% vs 24%).
Characteristics of included patients stratified into (1) axSpA with or without psoriasis, (2) PsA fulfilling or not fulfilling clinical definition of axial manifestation, (3) PsA fulfilling or not fulfilling imaging definition versus those with missing imaging data
Comparison of clinical versus imaging defined axPsA
Table 2 includes all patients of the cohort and shows baseline characteristics stratified into (1) axSpA with or without psoriasis and (2) PsA fulfilling or not fulfilling clinical definition of axial manifestation, and (3) PsA fulfilling or not fulfilling imaging definition and those in whom imaging was not performed. Thus, in table 2, PsA patients are listed twice, once in the respective clinical definition column and once in the respective imaging definition column. When comparing the baseline criteria of the 297 clinically positive with 196 imaging positive axPsA patients, there were no large differences between the groups (table 2).
The characteristics of PsA patients in whom imaging was not performed is very similar to the group of PsA patients lacking clinical criteria for axPsA. For example, in the group of patients in whom imaging was not performed, HLA-B27 was not available in 52% compared with 48% in the clinically negative group; in the clinically positive group and in patients with imaging results HLA-B27 was missing in 31% and 33%, respectively.
Comparison of axSpA+pso with axPsA
AxSpA+pso patients differed from axPsA regardless of the definition used (table 2). AxPsA patients were significantly more often female, older and less often HLA-B27 positive (table 2). Peripheral manifestations were significantly more often present in axPsA (84% in clinical definition group and 89% in imaging definition group) compared with 35% in axSpA+pso patients. Uveitis was significantly more commonly reported in axSpA+pso (table 2).
Disease activity measured by physician global disease activity as well as patient global disease activity, sleep disorder and pain measured by a Numeric Rating Scale were similar in axSpA+pso and axPsA.
We also compared the patient groups stratified according to their HLA-B27 status (online supplemental table 1). HLA-B27 positive patients were more often male, younger at symptom onset, had less often peripheral manifestations and more often uveitis.
Supplemental material
Results of imaging examinations
Imaging examinations of spine and SIJ were further analysed. At least one imaging examination was documented in 1411 (99%) of all axSpA, in 580 (42%) of all PsA patients. In the group of axSpA+pso, at least one imaging finding was available for 178 (98%) patients. At least one imaging finding was available in 75% of the clinical definition axPsA group and in 100% of the imaging definition group.
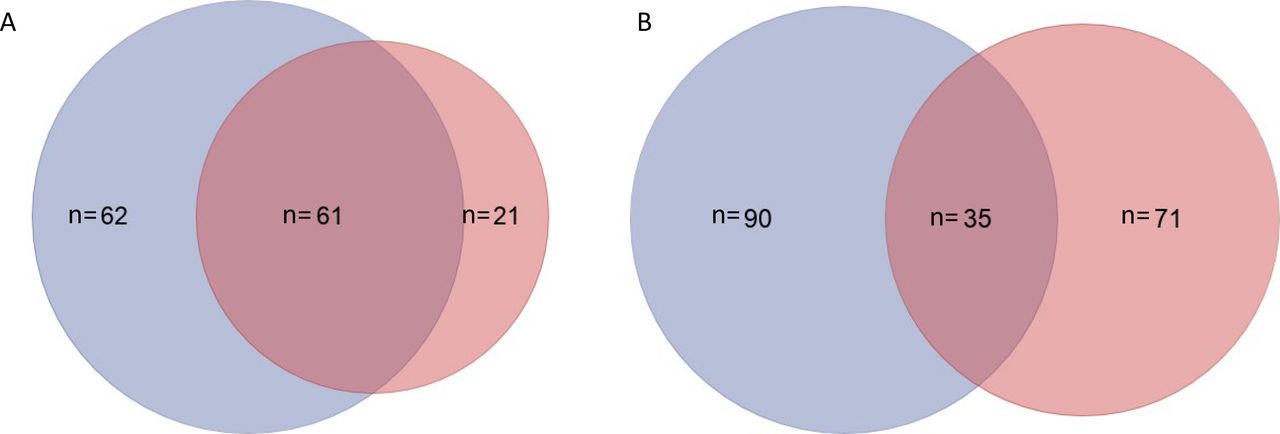
In the axSpA+pso patients, 62 patients showed imaging changes only in SIJ, 61 in both SIJ and spine, and 21 in spine only (figure 2A). In the axPsA patients, 90 showed changes only in SIJ, 35 in both and 71 in spine only (figure 2B).
{kind=link}
{kind=link}
(A) Distribution of imaging changes in axSpA+pso patients. (B) Distribution of imaging changes in axPsA patients. Blue: changes in the SIJ defined as radiographic alteration based on modified NY criteria or signs of active inflammation in MRI; pink: changes in the spine represented by syndesmophytes or ankylosis in radiographs or signs of active inflammation in MRI of the spine. Blue: only SIJ; overlap: both; pink: only spine. axSpA, axial spondyloarthritis; NY, New York.
In patients with SIJ radiographs available, 68% of axSpA+pso and 48% of axPsA fulfilled mNYc. 7% of axSpA+pso and 7% of axPsA patients showed an asymmetrical sacroiliitis (≥2 grade difference).
In addition, we compared the patients with radiographic data stratified whether they fulfil or not fulfil mNYc (online supplemental table 2). Radiographic axSpA and radiographic axPsA were more often male, had longer symptom and disease duration, and were more often HLA-B27 positive compared with non-radiographic axSpA and axPsA. The differences between radiographic axPsA with radiographic axSpA were similar to the main comparison with axPsA patients being more often female, older, less often HLA-B27 positive and having more peripheral manifestations (online supplemental table 2).
Supplemental material
Discussion
There is an ongoing debate, whether evidence generated in axSpA can be extrapolated to axial manifestation in PsA. This question has gained importance, as it is currently unclear whether axPsA follows the pattern of therapeutic response of PsA or exhibits a response pattern that more resembles the one of axSpA. Our analysis of a large observational cohort compares axSpA patients with concomitant psoriasis with PsA patients with axial involvement defined in two different ways in order to increase knowledge of these clinical entities.
A clear definition of axPsA is still missing, therefore, the prospective cross-sectional AXIS study, a joint study of ASAS and GRAPPA, has been designed to gain insight into the clinical and radiographic features of axPsA.7 In the literature, the nomenclature was not used consistently, for example, Helliwell et al used the term psoriatic spondylitis,10 Giovannini et al axial psoriatic disease14 and Jadon et al psoriatic spondyloarthritis.5 In most of the recent publications, the term axPsA has been used.6–9 15 16 However, the definitions of axPsA used in different analyses are manifold and show inconsistency due to missing harmonisation. In the only prospective, randomised controlled trial in axPsA (MAXIMISE), PsA patients with the clinical diagnosis according to their treating rheumatologist and with an active spinal disease defined by a BASDAI ≥4 and spinal pain Visual Analogue Scale ≥40 were included.11 In the post-hoc analysis of the guselkumab trials (DISCOVER), axPsA was defined as axial involvement due to the discretion of the investigator and presence of sacroiliitis on radiographs or MRI.17 In the post-hoc analysis of the PsA trials with ustekinumab (PSUMMIT), axial manifestation was based on the treating physician’s assessment.18 Feld et al from the Toronto group defined axPsA as fulfilling mNY criteria in radiographs.8 In a recent analysis from the Toronto cohort, patients with isolated axial PsA were differentiated from patients with axial and peripheral PsA.16 In the analysis of the CorEvitas register (formerly CORRONA register), axial manifestation of PsA was defined either by clinical judgement of treating physician and/or radiographic evidence of sacroiliitis.19 These differences hinder comparison of the so far published data and highlight the need for a better definition of axial involvement. This dilemma has been discussed recently in the Annals of Rheumatic Diseases.20–22
In our register, axSpA and PsA patients are documented within one web-based documentation system following the same study protocol. The participating rheumatologists include both, axSpA and PsA patients. However, we have different eCRFs for axSpA and PsA patients, taking disease specific aspects into account, but also sharing many items. For example, we did not include both classification criteria sets in both eCRFs but included ASAS criteria in the axSpA eCRF and CASPAR criteria in the PsA eCRF. Degree of spine mobility and IBP is not requested in PsA and information on the severity of psoriasis is not included in the axSpA eCRF. These differences are a limitation to our comparison. However, to further characterise patients with axPsA, we have carefully chosen information that is documented in both disease cohorts. We have decided to use two different definitions of axPsA and to compare the patients according to these definitions with axSpA patients who also have a psoriasis. This enhances a selection of patients with the highest probability of similarities between axSpA and axPsA.
More patients fulfilled the clinical definition of axPsA than the imaging-based definition. Therefore, the clinical definition is more inclusive but excludes those patients with only evidence of radiographic changes, which have been described earlier.5 23 The imaging definition included fewer patients. In the cross-tabulation, it can be seen, that there are groups of patients who only fulfil one definition. Importantly, the comparison of the clinical characteristics of the two axPsA definitions in our patients did not show substantial differences. However, both definitions have important limitations. The clinical definition was based on the documentation of any axial involvement of PsA diagnosed by a rheumatologist. However, we cannot rule out that patients with unspecific back pain or degenerative disorders have erroneously been included. The imaging definition was based on local reading and was not proven by a specialised central reader, which might have led to inclusion of unspecific cases.
We decided to compare the clinically most similar subgroups by analysing axPsA patients and axSpA patients with concomitant psoriasis. Despite this selection of very similar disease manifestations, the differences previously noted in comparisons between axPsA and axSpA remained robust.6 8 9 16 Thus axPsA patients were older, more often female and less often HLA-B27 positive. Peripheral manifestation was present in the majority of axPsA, while common extra-articular manifestations as uveitis and IBD were more often reported in axSpA. Some of these differences might be due to the known differences in the classification criteria sets (ASAS and CASPAR) used in the two diseases. For example, the ASAS criterion of an onset of IBP before an age of 45 years might explain the difference in age with a younger mean age in axSpA+pso compared with axPsA.
In addition, we have analysed the groups of patients according to their HLA-B27 status. HLA-B27 positive axPsA patients show more similarities to axSpA patients. For example, they are more often male, have more often uveitis and less often peripheral manifestations compared with HLA-B27 negative axPsA patients. These results are in accordance with a recent analysis, which focused on the influence of HLA-B27 status on radiographic phenotype of axSpA and axPsA.24
In the analysis of the radiographic data of our patients, we confirmed the finding that in PsA more patients show an involvement of the spine without involvement of the SIJ.5 25 It has been described that in axPsA the SIJ changes are more frequently unilateral. We could not confirm this finding; however, our data need to be interpreted carefully since only a small number of patients were available for this question.
Patient characteristics of those in whom imaging was not performed are similar to patients without clinical signs of axial manifestation. This reflects common routine care where imaging examinations are only requested (and paid for), if there are signs or symptoms of axial manifestation.
Limitations of this study are mostly due to the fact that the per-protocol assessments slightly differed in PsA and axSpA patients, which may have not allowed the analysis of the entire breadth of differences between the two disease entities. Hence, additional differences between axPsA and axSpA+pso might exist, which have not been considered sufficiently in this analysis. This especially pertains to spinal function and structural changes in the spine, which have not or were only partly analysed in the PsA group of patients.
Despite this limitation, these data suggest that axial involvement in PsA is different to axSpA, even if axSpA patients with psoriasis are used as a comparator. Furthermore, these differences between axPsA and axSpA+pso stay similar regardless of whether a clinical or an imaging-based definition of axPsA is used. These data indicate that extrapolation of evidence from axial SpA to axial manifestations in PsA should be performed with caution.
Data availability statement
Data are available on reasonable request. Applications to access the data should be made to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committee of the Charité University Medicine, Berlin (#EA1/246/16). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors acknowledge the invaluable contributions of all participating consultant rheumatologists and their patients. In particular, we would like to thank those rheumatologists who enrolled the highest numbers of patients: Kaufmann J, Schwarze I, Bohl-Bühler M, Feuchtenberger M, Eisterhus C, Kellner H, Klopsch T, Zinke S, Spengler L, Karberg K, Krüger K, Wernitzsch H, Marycz T, Liebhaber A, Stille C, Krause A, Müller B, Fricke-Wagner H, Kühne C, Dahmen G, Tony H-P, Burmester G, Baumann C and Häckel B.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @AnneRegierer, @ProftDr
Contributors ACR had full responsibility for the finished work and the conduct of the study, had access to the data, and controlled the decision to publish. ACR and AW had full access to all of the data in the study and were involved in analysis and interpretation of the data. ACR and AW took responsibility for the integrity of the data and the accuracy of the data analysis. ACR, AW, FP, XB, FB, DP, GS and AS were involved in study initiation, conception and design. All authors were involved in drafting the article and revising it critically for important intellectual content, and approved the final version to be published.
Funding RABBIT-SpA is supported by a joint, unconditional grant from AbbVie, Amgen, Biogen, Celltrion, Hexal, Janssen-Cilag, Lilly, MSD, Novartis, Pfizer, UCB and Viatris.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.