Article Text

Abstract
Objective To explore the risk of pre-eclampsia in rheumatoid arthritis (RA), axial spondyloarthritis (AxSpA) and psoriatic arthritis (PsA), focusing on the impact of treatment and disease activity.
Methods We identified RA, AxSpA and PsA singleton pregnancies (2006–2018) by linking medical birth registers to Swedish (SRQ) and Danish (DANBIO) rheumatology registers. Control pregnancies from the medical birth registers were matched 1:10 on maternal age, parity and birth year.
We obtained information on antirheumatic treatment before and during pregnancy and disease activity during pregnancy. Risks of pre-eclampsia in RA, AxSpA and PsA pregnancies, compared with control pregnancies, were estimated overall and by antirheumatic treatment (conventional synthetic disease-modifying antirheumatic drug (DMARD)/biological DMARD/corticosteroids, as monotherapy or combination therapy) and disease load (Health Assessment Questionnaire≥1/C-reactive protein≥10/Disease Activity Score in 28 joints≥3.2) through logistic regression (adjusted ORs (aORs) with 95% CI).
Results We observed 69, 34, and 26 pre-eclampsia events among RA (n=1739), AxSpA (n=819) and PsA (n=489), resulting in a risk of pre-eclampsia of, respectively, aOR 1.27 (95% CI 0.96 to 1.67), 1.17 (0.76 to 1.78) and 1.85 (1.10 to 3.12), compared with controls.
For RA, maternal combination therapy before and during pregnancy was associated with increased risk (1.59; 1.07 to 2.37 and 1.53; 0.97 to 2.39, respectively). For PsA, maternal monotherapy before pregnancy was associated with pre-eclampsia (2.72; 1.4 to 5.13). In RA pregnancies with available information (43%), high disease load was associated with doubled risk of pre-eclampsia (aOR 1.96; 1.26 to 3.04).
Conclusion PsA pregnancies, but not AxSpA pregnancies, were at increased risk of pre-eclampsia. For RA, combination therapy (potentially a surrogate for high disease activity both before and during pregnancy) and high disease load during pregnancy might be a risk factor for pre-eclampsia.
- Arthritis, Psoriatic
- Arthritis, Rheumatoid
- Biological Therapy
- Patient Reported Outcome Measures
- Spondylitis, Ankylosing
Data availability statement
Data may be obtained from a third party and are not publicly available. The data cannot be shared publicly due to the requirements of the involved register holders and the general data protection regulation, in order to protect the privacy of individuals.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Arthritis, Psoriatic
- Arthritis, Rheumatoid
- Biological Therapy
- Patient Reported Outcome Measures
- Spondylitis, Ankylosing
WHAT IS ALREADY KNOWN ON THIS TOPIC\
Data indicate that women with rheumatoid arthritis (RA), psoriatic arthritis (PsA) and axial spondyloarthritis (AxSpA) are at increased risk of adverse pregnancy outcomes, such as preterm birth and caesarean section.
Studies on risk of pre-eclampsia in these conditions are inconclusive, and data on impact of treatment and disease activity are lacking.
WHAT THIS STUDY ADDS
Women with PsA (but not AxSpA) had increased risk of pre-eclampsia.
In RA, we observed an increased risk of pre-eclampsia in women with combination therapy (potentially a surrogate for high disease activity before and during pregnancy) and high RA disease load.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our findings underline the importance of monitoring disease activity in women with RA and PsA before and during pregnancy, especially those with high disease activity and/or antirheumatic treatment prepregnancy.
Introduction
Rheumatoid arthritis (RA), axial spondyloarthritis (AxSpA) and psoriatic arthritis (PsA) affect women in their reproductive years. Previous studies have indicated associations between these disorders and adverse pregnancy outcomes, for example, preterm birth, small for gestational age and caesarean sections.1–7 The potential impact of disease activity and use of medication during pregnancy are causes for concern.7–9
Pre-eclampsia is a severe adverse pregnancy outcome affecting approximately 3%–5% of all pregnancies worldwide.10 11 Previous studies have suggested an increased risk of pre-eclampsia in RA pregnancies compared with healthy controls,1 2 12 although not in AxSpA.5 13 14 Corresponding data for PsA pregnancies are inconsistent.3 4
The severity of pre-eclampsia is emphasised by the fact that pregnancy termination is the only effective cure.10 If left untreated, it has fatal consequences for both mother and child.10 11 Consequently, it may result in induced preterm delivery.
Some of the established risk factors of pre-eclampsia are first pregnancy, very low or high maternal age and obesity.10 15 Furthermore, chronic inflammation might contribute to the pathogenesis.16 However, evidence on the impact of inflammatory disease activity and antirheumatic treatment on pre-eclampsia is lacking, even though high disease activity in RA and PsA has previously been associated to other adverse pregnancy outcomes, such as small for gestational age and preterm birth.3 17 18
Consequently, based on data from Swedish and Danish clinical and national registries, we aimed to evaluate the risk of pre-eclampsia in pregnancies of women with, respectively, RA, AxSpA and PsA, and to identify risk factors for pre-eclampsia in relation to: (1) antirheumatic treatment and (2) disease activity.
Methods
Data sources
We conducted a register-based matched cohort study in Sweden and Denmark. The included nationwide clinical and health registers were: the clinical rheumatology registers, that is, the Swedish Rheumatology Quality Register (SRQ) and the Danish DANBIO Registry,15–17 the Medical Birth Registers,18 19 the National Patient Registers,20 21 the Prescribed Drug Registers22–24 and the Total Population Registers (the Swedish Population and Death Register and the Danish Civil Registration System).25 26 The personal identification number assigned to all citizens in Sweden and Denmark allowed for linkage between the different registers. For details, see online supplemental table S1.
Supplemental material
Study population
In SRQ and DANBIO, we identified women with a rheumatologist-based diagnosis of RA, AxSpA or PsA (online supplemental table S2). From the Medical Birth Registers, we identified singleton pregnancies of these women by date of delivery: from 1 July 2007 to 31 December 2017 (in Sweden) and from 1 January 2006 to 31 December 2018 (in Denmark), to sample pregnancy cohorts for RA, AxSpA and PsA, respectively. Only pregnancies of women who were registered in SRQ or DANBIO at least 6 months prior to conception were eligible for inclusion. This criterion was applied to ensure access to relevant information on prepregnancy antirheumatic treatment and disease activity. Estimated date of conception was calculated as gestational age zero, based on the gestational age at birth registered in the Medical Birth Register (estimated from ultrasonography or, if ultrasonography was unavailable, by the recorded date of the first day of the last menstrual period).
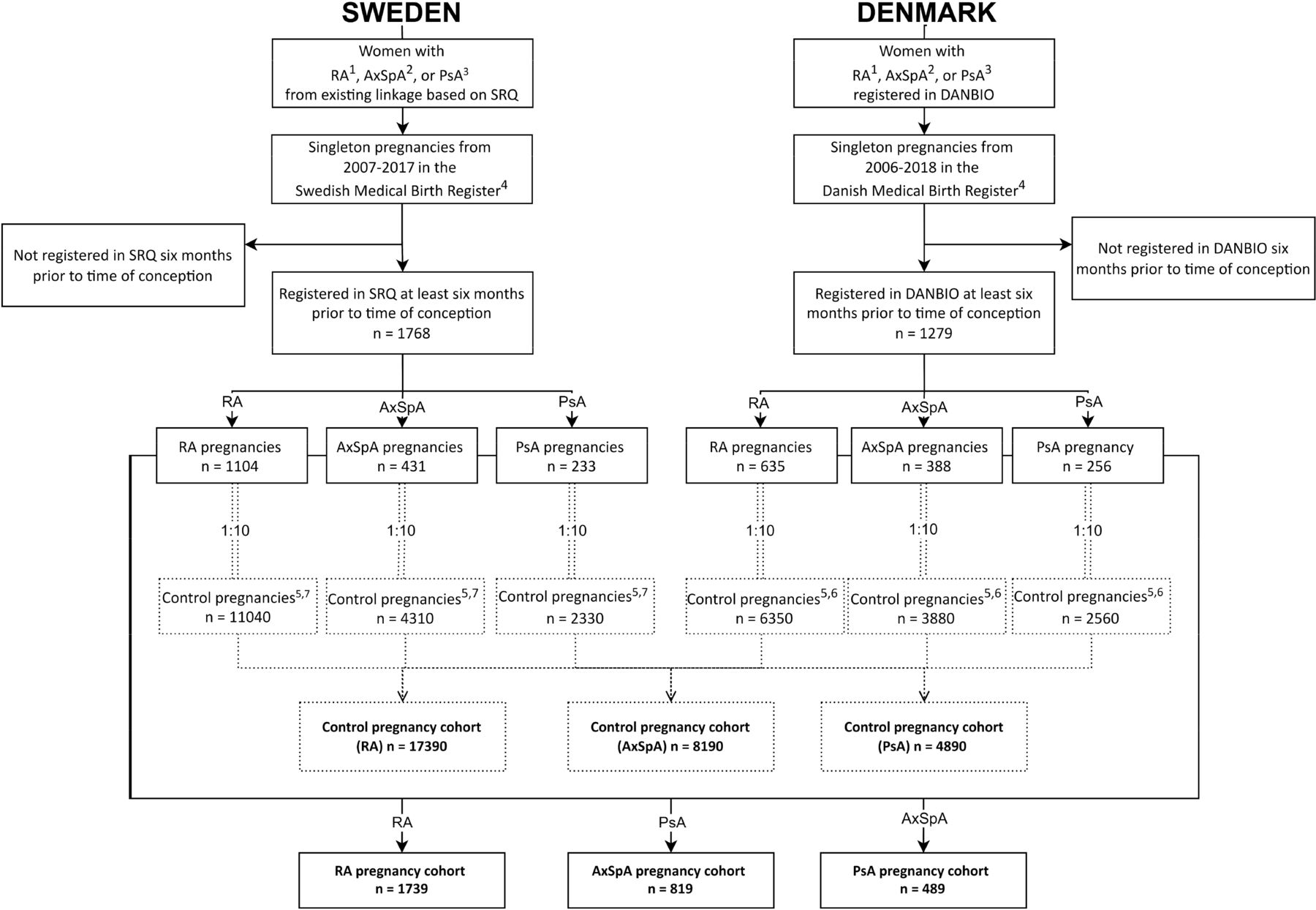
For each of the three pregnancy cohorts, we identified a control pregnancy cohort matched 1:10 on maternal age, parity and calendar year of delivery (figure 1). In Sweden, we identified control pregnancies from an existing linkage that comprised comparators to individuals with chronic inflammatory arthritis,17 27 and then we obtained information on their pregnancies from the Swedish Medical Birth Register. In Denmark, we identified control pregnancies from the general population in the Medical Birth Register (online supplemental table S3).
{kind=link}
Flow chart of RA, AxSpA, PSA and control pregnancy cohorts. 1ICD-10 RA M05, M06; 2ICD-10 AxSpA M45, M46.8, M46.9; 3ICD-10 PSA L40.5, M07.0, M07.1, M07.3; 4calendar year of delivery; 5matched on maternal age, parity and year of delivery registered in the national Medical Birth Register. Not included if any registration of chronic inflammatory arthritis (ICD-10 RA M05, M06.0, M06.2, M06.3, M06.8, M06.9, M12.3; PsA L40.5, M07.0, M07.1, M07.3; AxSpA M45, M46.0, M46.1, M46.8, M46.9; JIA M08, M09; PA M13.0) according to the National Patient Register; 6pregnancies from the Danish medical birth register; 7pregnancies from the Swedish Medical Birth Register of women registered in existing Swedish linkage. AxSpA, axial spondyloarthritis; DANBIO, the Danish Rheumatology Register; ICD-10, International Classification of Diseases, 10th revision; JIA, juvenile idiopathic arthritis; LMP, last menstrual period; PA, polyarthritis; PsA, psoriasis arthritis; RA, rheumatoid arthritis; SRQ, Swedish Rheumatology Quality Register.
Exposure
The primary exposure of interest was a diagnosis of RA, AxSpA or PsA. Second, we evaluated exposure to antirheumatic treatment and disease activity, before and during pregnancy.
Antirheumatic treatment
We obtained information on antirheumatic treatment prepregnancy (9 months prior to time of conception) and during pregnancy (time of conception until delivery) for the women with RA, PsA and AxSpA. Antirheumatic treatment was defined as: oral corticosteroids, conventional synthetic disease-modifying antirheumatic drugs (csDMARD) and biological (b)DMARD, including both tumour necrosis factor inhibitors (TNFis) and non-TNFi. Notably, this includes any treatment with each drug in the relevant period. Information on antirheumatic treatment was obtained from the Prescribed Drug Registers, SRQ/DANBIO and the Danish National Patient Register. If information conflicted between these sources, we used the information held by the Prescribed Drug Registers (online supplemental table S4).
Disease activity
Disease activity measures are reported by the treating rheumatologist in SRQ/DANBIO, as a part of routine care. There are no specific guidelines in rheumatology clinics for monitoring pregnant women. From SRQ and DANBIO, we obtained information on functional status and disease activity during pregnancy: Health Assessment Questionnaire (HAQ) (<1: low, ≥1: high), C-reactive protein (CRP) (<10 mg/L: low, ≥10 mg/L: high), and for RA and PsA, we also obtained Disease Activity Score in 28 joints (DAS28-CRP) (<3.2: low, ≥3.2: moderate/high) (online supplemental table S2). We excluded registrations of CRP >50 mg/L (n=2) to avoid potential confounding by infectious conditions. DAS28-CRP was calculated without Global Health-Visual Analog Scale score, since the latter may be influenced by pregnancy.28 Because most patients visit their rheumatologist only once a year (in the case of stable disease), estimates of maternal disease activity and functional status were mainly based on one registration of disease activity in each time period (ie, before and during pregnancy). In case of multiple registrations, we chose the maximum value for each variable. Due to the high proportion of missing data (689/819, 85%) on AxSpA-specific disease activity measures (eg, Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)) during pregnancy in SRQ and DANBIO as well as the influence of pregnancy on measurements of axial pain, we abstained from using these data.29 We additionally defined a compound measure of disease load as ‘high’, if there was any registration of HAQ ≥1, CRP ≥10 mg/L and/or DAS28-CRP ≥3.2 during pregnancy. The variable was registered as missing if none of CRP, HAQ or DAS28-CRP was registered (online supplemental table S2).
Outcome
The outcome of interest was pre-eclampsia, which is clinically defined by new-onset hypertension and multiorgan failure. In addition to hypertension and proteinuria, symptoms may include headaches and cerebral or visual disturbances that can progress into convulsions, if the disorder develops into to eclampsia. In the present study, pre-eclampsia was defined as one or more diagnoses of pre-eclampsia or eclampsia, International Classification of Diseases, 10th revision (ICD-10) O14-O15, registered in the National Patient Registers at any time point during pregnancy (online supplemental table S2).30 31 Furthermore, pre-eclampsia was classified based on severity: moderate pre-eclampsia: ICD-10 O14.0 or O14.9, and severe pre-eclampsia: ICD-10 O14.1-O14.2 and O15.0–15.9.32 We also classified pre-eclampsia based on timing in relation to delivery; early pre-eclampsia as pre-eclampsia and delivery at <34 gestational weeks and late pre-eclampsia as pre-eclampsia and delivery ≥34 weeks.33–35 To account for the strong link between hypertension and pre-eclampsia, we excluded ICD-10 code O11, that is, pre-eclampsia superimposed in hypertension, from the outcome definition.
Covariates
From the Medical Birth Registers, we identified maternal age, parity, calendar year of delivery and self-reported information on smoking and body mass index (BMI) at the first antenatal visit. From the educational registers, we obtained information on mother’s highest educational level at the time of delivery (online supplemental table S2). We also included country of delivery as a covariate.
Statistical analysis
Overall risk in RA, AxSpA and PsA
All analyses were performed on a pooled dataset that included Swedish and Danish data. Analyses were based on complete cases, and no imputation on missing data was performed. Categorical data are presented as counts and percentages, and continuous variables as medians and IQRs. Using logistic regression models, we calculated crude and adjusted ORs (aORs) (‘risk’) with corresponding 95% CIs for pre-eclampsia in, respectively, RA, AxSpA and PsA pregnancies, compared with their respective controls.
We selected potential confounders a priori based on the existing literature10 11 33 36 and thus adjusted for BMI, smoking, education and country. We further adjusted for the matching variables (maternal age, parity and year of delivery) where the matching was broken. We applied a generalised estimating equation method (maternal identification as a cluster assuming an exchangeable correlation structure), because some women contributed with more than one pregnancy during the study period.37
In sensitivity analyses, we estimated country-specific risk of pre-eclampsia in RA, AxSpA and PsA pregnancies, compared with control pregnancies. We also tested differences in risk estimates between countries, by including an interaction term (exposure*country) in the primary analyses. Finally, we estimated risks of early and late, and moderate and severe pre-eclampsia, respectively.
Risk in relation to antirheumatic treatment and disease load
The analyses were stratified by maternal antirheumatic treatment in the 9 months prepregnancy, and during pregnancy and by disease activity during pregnancy.
In the analyses stratified on treatment exposure, we classified treatment as: (A) untreated (no registration of any antirheumatic drug), (B) monotherapy (csDMARD, bDMARD or oral corticosteroids) and (C) combination therapy (csDMARD, bDMARD or oral corticosteroids in any combination of at least two).
In the analyses stratified on disease activity and functionality score, we stratified on: (A) HAQ (high, low and missing), (B) CRP (high, low and missing), (C) DAS28-CRP (high, low and missing) and (D) the compound score ‘disease load’ (high, low and missing).
In the primary analyses, we compared RA, AxSpA and PsA pregnancies to their respective controls. Additionally, we performed internal comparisons in which the disease groups without any antirheumatic treatment or with low disease activity constituted the references, respectively.
In a sensitivity analysis, we restricted registration on disease activity during pregnancy to 180 days from time of conception (first and second trimester), because pre-eclampsia can occur as early as from gestational week 20.
Data were analysed in SAS V.9.4 and R Studio V.1.3.1093.
Patient involvement
Patient representatives participated in the development of research questions and study design.
Results
We identified 1739 RA, 819 AxSpA and 489 PsA pregnancies and 17390, 8190 and 4890 control pregnancies, respectively. For RA and AxSpA pregnancies, there were no major differences in maternal characteristics, compared with their control pregnancies (table 1). By contrast, pregnant women with PsA were more likely to be obese, less educated and smokers, compared with controls. For country-specific characteristics, see online supplemental tables S5–S6.
Maternal characteristics in RA, AxSpA, PSA and control pregnancies, n (%)
In PsA, we found in total 26 (5.3%) events of pre-eclampsia, resulting in an 85% increased risk of pre-eclampsia compared with control pregnancies (aOR 1.85; 95% CI 1.10 to 3.12). Compared with their controls, the risk was slightly increased in RA (69 events, 3.9%), although statistically insignificant (1.27; 0.96 to 1.67). In AxSpA (34 events, 4.2%), the corresponding aOR was 1.17 (95% CI 0.76 to 1.78) (table 2).
Risk of pre-eclampsia in RA, AxSpA and PSA pregnancies versus control pregnancies
Within all three conditions (RA, AxSpA and PsA), the risk estimates for moderate and severe pre-eclampsia were largely similar (online supplemental table S7). Very few women developed early pre-eclampsia, and we were not able to present or detect a potential difference in rates, compared with the controls, due to low power (data not shown).
Notably, the risk estimate for pre-eclampsia in PsA was somewhat higher in Denmark than in Sweden, but there were no statistically significant differences in risk estimates between the countries for the interaction term exposure*country (p=0.29, 0.58 and 0.52 for RA, AxSpA and PsA, respectively). For country-specific risk estimates, see online supplemental tables S8–S9.
Risk in relation to antirheumatic treatment prepregnancy
We observed an aOR of 1.59 (95% CI 1.07 to 2.37) in RA pregnancies receiving combination therapy prepregnancy compared with control pregnancies, whereas we found no increased risks among those untreated or with monotherapy prepregnancy, compared with control pregnancies (table 3).
Risk of pre-eclampsia in RA, AxSpA and PSA pregnancies in relation to antirheumatic treatment strategy prepregnancy versus control pregnancies
In AxSpA pregnancies, we found no increased risks of pre-eclampsia when stratifying on treatment, compared with control pregnancies (table 3).
In PsA pregnancies, we observed an increased risk of pre-eclampsia when receiving prepregnancy monotherapy compared with control pregnancies (aOR 2.72; 95% CI 1.44 to 5.13), whereas no significantly increased risks were found in PsA pregnancies exposed to combination therapy or untreated (table 3).
In the AxSpA and the PsA pregnancies, the numbers of events were too low to conduct internal comparisons (untreated pregnancies as references), while in RA, a comparison of prepregnancy use of combination therapy to untreated pregnancies demonstrated a signal similar to the results of the analyses including the control pregnancies as references (aOR 1.33; 95% CI 0.68 to 2.61). When comparing prepregnancy monotherapy to untreated, we found no statistically significant increased risk (aOR 0.86; 95% CI 0.42 to 1.76).
Risk in relation to anti-rheumatic treatment during pregnancy
We found no statistically significant increased risks when stratifying on treatment during pregnancy in any of the disease groups compared with their control pregnancies (table 4). However, among RA women exposed to combination therapy during pregnancy, we observed a tendency towards an increased risk compared with control pregnancies (aOR 1.53; 95% CI 0.97 to 2.39). When comparing RA pregnancies with monotherapy or combination therapy during pregnancy to RA pregnancies untreated during pregnancy in internal comparison, the pattern was similar, but the confidence intervals were wide (aOR 1.31; 95% CI 0.69 to 2.49 and aOR 1.52; 95% CI 0.79 to 2.91, respectively) (data not shown in tables).
Risk of pre-eclampsia in RA, AxSpA and PSA pregnancies in relation to antirheumatic treatment during pregnancy versus control pregnancies.
Antirheumatic treatment during pregnancy was not associated with any significantly increased risk in AxSpA pregnancies, compared with controls. For PsA, the risk estimates from the analysis stratified by treatment during pregnancy were in line with the overall risk of pre-eclampsia in PsA, but they did not reach statistical significance (table 4).
Risk in relation to functional status and disease activity during pregnancy
We had information on one or more measures of either HAQ, CRP or DAS28-CRP during pregnancy in 43% (n=756) of all RA pregnancies. The risk of pre-eclampsia was approximately doubled in RA pregnancies with high DAS28-CRP, compared with controls (aOR 1.95; 95% CI 1.10 to 3.49), and the results were similar for HAQ and CRP (table 5). When assessing functional status and disease activity variables as disease load, the signal was even stronger (aOR 1.96; 95% CI 1.26 to 3.04). The internal comparison (untreated group constituting the reference) further indicated an increased risk in RA pregnancies with high versus low disease load, but the estimates did not reach statistical significance (table 5). RA pregnancies lacking information on all three variables had no increased risk compared with controls.
Risk of pre-eclampsia in RA, AxSpA and PSA pregnancies in relation to functional status and disease activity any time during pregnancy versus control pregnancies.
In AxSpA and PsA the level of missing data was high on disease load was high, and although we found no association between pre-eclampsia and high disease load, the number of events was few (table 5).
Overall, the estimates did not substantially change when we restricted the analyses to only include disease activity measurements in the first and second trimester (online supplemental table S10).
Discussion
In this large observational cohort study, including more than 1700 pregnancies, we included nationwide register data from Swedish and Danish clinical and health registers and observed several important findings of clinical relevance regarding the risk of pre-eclampsia in women with, respectively, RA, AxSpA and PsA.
We found an approximately doubled risk of pre-eclampsia in PsA pregnancies, compared with control pregnancies. The risk was primarily driven by women receiving monotherapy before pregnancy. By contrast, we identified no overall increased risk of pre-eclampsia in RA and AxSpA pregnancies. However, our results indicated that women with RA receiving combination therapy before or during pregnancy carried a moderately increased risk. Among RA pregnancies with high disease activity during pregnancy, we observed a doubled risk of pre-eclampsia.
Previous studies on the risk of pre-eclampsia in RA pregnancies are few and with inconsistent findings.1 2 38–40 In the present study, we found signals of an increased risk of pre-eclampsia, although not statistically significant. This is in line with some,38 39 but not all, previous studies.1 2 12 A recent publication, based on a cohort of more than 6000 RA pregnancies in the USA, reported an increased risk of pre-eclampsia compared with unexposed pregnancies (aOR 1.71; 95% CI 1.54 to 1.87).1 The study did not include information on parity, which might, at least in part, explain the increased risk estimates given that nulliparity is related to pre-eclampsia,10 and women with RA have fewer children than age-matched controls.9 In the present study, we matched and adjusted for parity.
We further identified an approximately doubled risk in RA pregnancies with one registration of high disease activity during pregnancy compared with controls (without respect to treatment), though, it is difficult to properly disentangle the effects of disease activity from other potential risk factors. However, we are the first to demonstrate such an association for pre-eclampsia, although previous studies have indicated associations between high RA disease activity and adverse pregnancy outcomes, such as preterm birth and small for gestational age.7 41 42 It is known that the pathogenesis of pre-eclampsia is related to some degree of immune dysregulation and that a high inflammatory load can lower the threshold for overt pre-eclampsia.11 Therefore, it could be hypothesised that RA-related inflammatory activity might be a risk factor also for pre-eclampsia, but pathophysiology remains to be explored in detail.
However, the impact of disease activity and antirheumatic treatment on the risk on pre-eclampsia is difficult to disentangle. For RA pregnancies, we found an association between receiving combination therapy before pregnancy and a modestly increased risk of pre-eclampsia in RA pregnancies. The signal was similar, but weaker, when we assessed treatment during pregnancy.
For PsA, the risk of pre-eclampsia was also increased in untreated women, with respect to antirheumatic drugs during pregnancy. Assuming that treatment is a proxy for disease activity, this may seem contradictory. However, it could be that some untreated women stopped treatment due to pregnancy wishes, leading to disease flares and thereby adverse outcomes.43 In the present study, unfortunately, we did not have the granularity to assess exactly how treatment strategies (ie, continuing or stopping therapy) affected the risk of pre-eclampsia.
To separate these effects, more detailed information on disease activity and treatment, prospectively and repeatedly collected during pregnancy, would have been ideal. Nevertheless, our findings suggest that combination therapy prepregnancy is a surrogate of severe disease rather than a risk factor of its own.5 7 This supports the perception that pregnant women with RA should not fear treatment, but rather the disease flares arising from insufficient treatment. This is further strengthened by a recent paper from our group showing that the risk of preterm birth and SGA remained increased in RA pregnancies with high disease activity, even after adjusting for type of treatment during pregnancy.7
For PsA, we found an overall increased risk of pre-eclampsia. Although previous results have been conflicting, our findings are in line with two published observational studies.4 44 These publications presented an increased risk of pre-eclampsia—both in a study based on prospectively collected interview data and in a register study, including 117 and 946 pregnancies exposed to PsA, respectively. On the contrary, a Swedish study, including 541 pregnancies exposed to PsA, found no increased risk of pre-eclampsia.3 A recently published meta-analysis presented a pooled OR of 1.40 (95% CI 0.78 to 2.51), based on the three aforementioned studies, which is slightly lower than the risk estimate in our cohort.45 However, the patients included in our study may suffer from more severe disease compared with the patients included in previous cohort studies from Sweden and Denmark3 4 since those included patients only from the National Patient Register. In the present study, women with PsA were identified in the clinical rheumatology registers (SRQ and DANBIO) based on diagnoses given by trained rheumatologists, which increased the validity of the diagnosis. At the same time, in SRQ and DANBIO, there may be a selection towards patients with more severe PsA treated with bDMARDs or with more severe comorbidity.15–17 Notably, the risk estimate for PsA women untreated during pregnancy was increased to the same extent as monotherapy and combination therapy, however, insignificantly. Consequently, though data were scarce, our results did not indicate that treatment itself was associated with the risk of pre-eclampsia in PsA pregnancies.
The analyses evaluating impact of disease activity were, however, limited by low power. Our finding of a significantly increased risk of pre-eclampsia in PsA, but not in the two other conditions, is interesting. However, even though RA, AxSpA and PsA share some similarities, they also differ with respect to comorbidity conditions. For example, there is a well-established association between psoriasis/PsA and the metabolic syndrome including hypertension, obesity and dyslipidaemia,46 which are also associated to pre-eclampsia. In our study, we observed that women with PsA were more often smokers and had higher BMI in early pregnancy, as compared with their controls. However, even though we adjusted for smoking and BMI, women with PsA may carry underlying predisposing factors for pre-eclampsia, apart from factors associated with the underlying disease itself and/or chronic inflammation.
Taken together, our results may reflect an association between severe PsA (using prepregnancy treatment as a proxy) and pre-eclampsia. Additionally, it is of clinical importance that the absolute risk in patients with PsA might be increased due to a higher extent of obesity and smoking among these patients.
For AxSpA, we did not identify any increased risk of pre-eclampsia, which is in line with previous studies.5 13 14 44 Similarly, there were no associations in relation to antirheumatic treatment or disease activity in AxSpA. Although the stratified analyses exploring impact of disease activity and treatment were hampered by low power, the only previous study comprised two pre-eclamptic events, compared with 34 pre-eclamptic events in our AxSpA group.47 Based on existing evidence and our results, compared with controls, women with AxSpA do not appear to be at substantially increased risk of pre-eclampsia.
The strengths of our study include the large size of our pregnancy cohorts, enriched with prospectively and independently collected data from the comprehensive Scandinavian clinical health and population registers. This allowed us to include a large number of pregnancies, to eliminate the risk of recall bias and to adjust for important covariates, such as smoking, BMI and educational level. In contrast to previous studies, we defined RA, AxSpA and PsA solely from the clinical rheumatology registers to ensure a high degree of diagnostic validity. We were also able to include information on disease activity, which has never been done before.17 Furthermore, we combined multiple data sources to obtain the most accurate treatment information available. In RA, we had information on HAQ, CRP or DAS28-CRP in 756 (43%) pregnancies at any time during pregnancy, which makes it the largest cohort in the field.
The study also has challenges to address. Despite the fact that we had data on all pregnancies from the two countries in the study period, the number of events was low. This reduced our statistical power, especially in women with AxSpA and PsA. We lacked information on disease activity in a considerable proportion of the pregnancies, and additionally, few women had more than one visit at a rheumatologist registered in SRQ/DANBIO during the pregnancy. We acknowledge that relying in many cases only on one registered value of disease scores is not optimal, but it is based on the best available data we had and corresponds well to clinical routine care (1 yearly visit in stable disease).
Given the proportion of missing information on disease activity, especially in PsA and AxSpA, we chose to construct the composite score: disease load. The purpose was to identify women with any clinical signs of disease activity and, reassuringly, for RA, we observed overall consistent findings for disease load compared with the individual parameters included (HAQ, CRP, and DAS28-CRP). Therefore, we find it relevant to present the ORs for the compound disease load variable since it offered the best available measurement to evaluate disease activity in AxSpA and PsA.
Also, our information on treatment was not complete. We solely had information on filled prescriptions and not whether the women were actually compliant to the medication. Hence, incomplete registration of treatment initiation and withdrawal cannot be excluded.
To properly disentangle the potential effects of disease activity and treatment on the risks of adverse pregnancy outcomes would require even more detailed information on treatment and disease activity. The relatively large proportion of patients without visits during pregnancy in the quality registers suggests that the clinical practice of patient follow-up during pregnancy, in some perspectives, is suboptimal. Hence, to obtain more granular information, a prospective study with a close follow-up of women included before or in early pregnancy would be optimal.48
With respect to AxSpA, both patients with ankylosing spondylitis and unspecific spondyloarthritis were included without stratifying on subtypes, and we lacked more valid measures of disease activity, such as BASDAI.47 Despite extensive confounder adjustment, we could not eliminate potential residual confounding due to the observational study design. In our analyses, we did not have the opportunity to adjust for previous pre-eclampsia, which is an important risk factor for pre-eclampsia. Likewise, we lacked information on prescriptions of acetylsalicylic acid (ASA), which would have been of interest, given the use of prophylactic use of ASA to prevent pre-eclampsia in women with predisposing risk factors. Finally, the differences in the pathophysiology of early and late pre-eclampsia are subjects of ongoing discussion.33 In this study, we were not able to present stratified risk analyses on this due to low number of early pre-eclamptic events. Notably, RA, AxSpA and PsA were all evenly associated to both severe and moderate pre-eclampsia.
In conclusion, women with PsA, but not AxSpA, had an increased risk of pre-eclampsia compared with control pregnancies, even when adjusting for well-known risk factors of pre-eclampsia. For women with RA, our results indicated that severe disease (ie, combination therapy before and during pregnancy and high disease activity during pregnancy) might be a risk factor for pre-eclampsia. From a clinical perspective, our findings add to the field of knowledge, by informing clinicians of the underlying risk of pre-eclampsia in these patient populations and by emphasising the importance of monitoring women with, in particular, RA and PsA regarding this risk.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data cannot be shared publicly due to the requirements of the involved register holders and the general data protection regulation, in order to protect the privacy of individuals.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Ethics Review Board in Stockholm (2015/1844-31/2). Approval by the Danish Ethics Committee was not required because the study had a register-based design (H-18003871). The project was approved by the Danish regional Data Protection Agency (RH-2018–68). All data were hosted at Statistics Denmark’s servers.
Acknowledgments
We would like to acknowledge the patient representatives of the NordForsk collaboration for their valuable contribution to this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
AEPS and FG are joint first authors.
MLH and KH are joint senior authors.
Contributors Study concept and design: all authors: Analysis of data: AEPS and FG. Interpretation of data: all authors. Drafting the manuscript: AEPS, BG, AR, MLH and KH. Critical revision of the manuscript for important intellectual content: all authors. Approval of final version: all authors. Guarantor of overall content: AEPS.
Funding This work was supported by NordForsk, FOREUM and the Danish Rheumatism Association (Grant number R151-A4623 and R161-A5262).
Competing interests AES: none; KH: none; BG: research grants: AbbVie, Pfizer and BMS; AR: none; MLH: consultancy fees: Biogen, Celltrion, Janssen Biological B.V, MSD, Pfizer, Samsung Biopis; research grants: AbbVie, Biogen, BMS, Eli Lilly Danmark A/S, Lundbeck Fonden, Pfizer, Roche, Medac, Sandoz, Novartis; speakers bureau: Biogen, Celltrion, Janssen Biological B.V, MSD, Pfizer and Samsung Biopis; FG: none.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.