Article Text

Abstract
Objective To investigate the impact of sustained low disease activity (LDA)/remission (REM) on physical function, quality of life (QoL) and structural outcomes in secukinumab-treated psoriatic arthritis (PsA) patients from the FUTURE 5 study.
Methods FUTURE 5 was a randomised, double-blind, placebo-controlled, parallel-group, phase 3 study in patients with active PsA. Patients were categorised according to LDA (Minimal Disease Activity, MDA/Disease Activity index for Psoriatic Arthritis, DAPSA LDA+REM) or REM (very LDA/DAPSA REM): not achieving LDA/REM, achieving it once or sustained LDA/REM ≥3 times up to week 104. Key outcomes were improvements in Health Assessment Questionnaire Disability Index and Short Form-36 Physical Component Summary Score, proportion of non-radiographic progressors and predictors of sustained LDA response.
Results Patients were randomised (N=996) into the following treatment groups: secukinumab 300 mg (N=222), secukinumab 150 mg loading (N=220)/non-loading (N=222) and placebo (N=332). Baseline characteristics were comparable between patients with sustained DAPSA and MDA responses. By week 104, 48%–81% and 19%–36% of the secukinumab-treated patients achieved sustained LDA and REM, respectively. Numerically greater improvements in physical function and QoL were observed with sustained LDA/REM versus LDA/REM achieved once or not at all, although patients reached the established minimal clinically important difference for all composite indices. A high proportion of secukinumab-treated patients were non-structural progressors at 2 years irrespective of achieving sustained LDA/REM. Younger age, lower body mass index at baseline, reduced tender joint count and PsA pain at week 16 were key predictors of sustained LDA in secukinumab-treated patients.
Conclusion Sustained LDA/REM was associated with improvements in physical function, QoL and inhibition of structural damage progression.
- Arthritis, Psoriatic
- Biological Therapy
- Patient Reported Outcome Measures
Data availability statement
Data are available on reasonable request. Data may be obtained from a third party and are not publicly available. The datasets generated and/or analysed during the current study are not publicly available. Novartis is committed to sharing with qualified external researchers access to patient-level data and supporting clinical documents from eligible studies. These requests are reviewed and approved on the basis of scientific merit. All data provided are anonymised to respect the privacy of patients who have participated in the trial, in line with applicable laws and regulations. The data may be requested from the corresponding author of the manuscript. The protocol can be made available on request by contacting the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is limited understanding of the proportion of patients who achieve long-term sustained low disease activity (LDA)/remission (REM) with secukinumab, the potential benefits and the predictors of response for these stringent outcomes.
WHAT THIS STUDY ADDS
A majority of secukinumab-treated patients achieved sustained LDA through 2 years irrespective of the outcome measure used, that is, Minimal Disease Activity (MDA) or Disease Activity index for Psoriatic Arthritis (DAPSA) LDA+REM.
Sustained LDA in secukinumab-treated patients was associated with better long-term functional improvement and long-term improvement of health-related quality of life.
There was a disconnect between inhibition of structural damage progression and disease activity.
Main predictors of sustained LDA response in secukinumab-treated patients were younger age, lower body mass index at baseline, lower disease activity and pain at week 16.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These data reinforce the validity of MDA and DAPSA LDA+REM as treatment goals in psoriatic arthritis since their achievement led to clinically meaningful benefits in health-related quality of life and physical function in psoriatic arthritis (PsA). Moreover, irrespective of achievement of sustained LDA or REM, there was inhibition of structural damage, highlighting the protective effect of secukinumab on radiographic progression in patients with PsA.
Introduction
Psoriatic arthritis (PsA) is a heterogeneous, chronic and progressive musculoskeletal inflammatory disease characterised by enthesitis, dactylitis, and skin, nail, peripheral and axial manifestations.1 It is often associated with impaired physical function and reduced health-related quality of life (HRQoL).2
The clinical heterogeneity of PsA is also translated by an important number of composite indices to measure disease activity. There is still an ongoing debate which of these disease activity indices should be used preferably and whether several unidimensional scores, each covering one PsA disease domain, or one multidimensional score encompassing multiple domains should be favoured for disease activity monitoring.
The latest Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) recommendations highlight that the goals of therapy for all patients with PsA are to achieve and maintain the lowest possible level of disease activity in all domains of disease corresponding to at least low disease activity (LDA) and ideally to remission (REM) to optimise functional status, improve quality of life (QoL) and well-being, and prevent structural damage.3
While the European Alliance of Associations for Rheumatology (EULAR) and GRAPPA recommendations support a treat-to-target (T2T) approach, they do not provide a clear recommendation for one disease activity score to guide therapeutic decisions in patients with PsA. However, the Disease Activity index for Psoriatic Arthritis (DAPSA) or Minimal Disease Activity (MDA) criteria seem to be the preferred options in clinical trials or clinical practice.4–7 DAPSA is a unidimensional, continuous measure that primarily focuses on articular involvement, whereas MDA is a categorical index that includes multiple disease domains and physical function.
Regular disease activity evaluation using these validated disease activity scores and subsequent adjustment of medical therapy to reach and maintain a defined therapeutic target like LDA or REM is summarised in T2T recommendations.3 Implementing a T2T approach in early PsA patients using MDA has shown several advantages compared with routine care. In the first T2T trial in PsA (TIght COntrol of Psoriatic Arthritis), though an impact of tight control on structural damage was not demonstrated, the study showed improvement in joint, skin and patient-reported outcomes (PROs) compared with standard of care.8
Secukinumab, a human monoclonal antibody that directly inhibits interleukin (IL)-17A, has demonstrated rapid and sustained improvement in signs, symptoms, physical function and improvement of HRQoL in patients with PsA over 5 years across the Phase 3 FUTURE programme.9–13 However, based on the different treatment recommendations in PsA which focus on more stringent treatment goals with LDA and REM than the efficacy data previously reported in the FUTURE trials, we present here retrospective analysis from the 2-year FUTURE 5 study which investigated the proportion of secukinumab-treated patients who could achieve and sustain LDA or REM, their benefits on patients and the predictors of response to LDA or REM.
Methods
Study design and patients
FUTURE 5 (NCT02404350) was a 2-year, randomised, double-blind, placebo-controlled, parallel-group, phase 3 study. Detailed study design is presented in online supplemental figure 1 and inclusion and exclusion criteria have been previously reported.13 14 Briefly, patients aged ≥18 years and those who met the ClASsification criteria for Psoriatic ARthritis (CASPAR) criteria with active PsA at screening and baseline and with symptoms of active PsA for at least 6 months were included in the study. Key exclusion criteria included history of or ongoing infection, prior use of a biologic other than a tumour necrosis factor inhibitor (TNFi) agent, use of ≥3 different TNFi agents and active inflammatory disease other than PsA.
Supplemental material
Eligible patients were randomly (2:2:2:3) allocated to one of the four following treatment groups: subcutaneous (s.c.) secukinumab 300 mg with loading dose (300 mg), s.c. secukinumab 150 mg with loading dose (150 mg LD), s.c. secukinumab 150 mg without loading dose (150 mg NL) or placebo administered at baseline, at weeks 1–3, and then every 4 weeks starting at week 4. Non-responders (patients with <20% improvement in tender joint count (TJC) or swollen joint count (SJC) from baseline) in the placebo group were switched to s.c. secukinumab 300 mg or 150 mg at week 16, and the responders were switched to s.c. secukinumab 300 mg or 150 mg at week 24. The study remained blinded to treatment allocation until week 52. After week 52, the secukinumab dose could be escalated from 150 mg to 300 mg according to the clinical judgement of the investigator following a protocol amendment.
During the open-label study period starting at week 52, patients continued to receive the same active dose of secukinumab as open-label treatment, administered until week 100. Patients were not allowed to switch to a lower dose once dose escalation had been done. Safety and efficacy procedures were conducted every 12–16 weeks during this open-label period.
The study was conducted in accordance with the Declaration of Helsinki15 and was approved by institutional review boards or independent ethics committees at each participating centre (online supplemental table 2). Written informed consent was obtained from all enrolled patients. Data were collected in accordance with the Good Clinical Practice guidelines by the study investigators and were analysed by the sponsor.
Outcome measures
Patients were grouped into three categories as follows: not achieving LDA/REM, achieving LDA/REM once only or sustained LDA/REM ≥3 times between weeks 24 and 104. Improvements in physical function (Health Assessment Questionnaire Disability Index (HAQ-DI)) for DAPSA only (also a component of MDA), and QoL (Short Form-36 Physical Component Summary score(SF-36 PCS)) for both DAPSA and MDA, were assessed from baseline through week 104. The proportion of non-radiographic progressors, defined as a change from baseline in the van der Heijde-modified total Sharp score (vdH-mTSS) ≤0.5, was determined up to week 104.16
Statistical analyses
Post hoc analyses involved patients enrolled into one of the four treatment groups—secukinumab 300 mg, secukinumab 150 mg LD, secukinumab 150 mg NL and placebo—from the FUTURE 5 study who had completed the 2-year study with no missing LDA/REM assessments at both weeks 24 and 104 to assure that the sustainability of status/responses was uniformly assessed for all patients during the same time period only.
Baseline demographics and clinical characteristics were summarised in patients who achieved sustained very LDA (VLDA) or MDA response and DAPSA REM or DAPSA LDA+REM status and in those who did not achieve these responses or states. Descriptive statistical analyses were performed on REM and LDA according to VLDA or MDA response and DAPSA REM or DAPSA LDA+REM status to group the patients into one of the three following categories: not achieving LDA/REM, achieving LDA/REM only once or sustained LDA/REM (which was defined as patients who achieved LDA/REM between weeks 24 and 52 and maintained the same response for at least two of the next six visits (visit every 8 weeks) up to week 104). Descriptive comparisons of achievement of one of these three categories by randomised treatment groups and in relation with changes from baseline to week 104 in the PsA-modified Sharp/van der Heijde score, in HAQ-DI score and in SF-36 PCS were reported as observed. In order to assure that the sustainability of responses was uniformly assessed for all patients in the same time window, only patients having non-missing evaluations at both week 24 and week 104 were included in this analysis. Intermittent missing assessments at scheduled time point were not considered.
Although patients could have the secukinumab dose escalated from 150 mg to 300 mg from week 52 according to the investigator’s judgement, they were analysed as per their original randomised group.
Multivariate logistic regression analyses were conducted to assess the effect of demographics, baseline disease characteristics, change from baseline to week 16 in specific clinical characteristics (TJC, PsA pain), and treatment on achievement of sustained DAPSA LDA+REM or sustained MDA.
Results
Baseline demographics, clinical characteristics and patient disposition
In the FUTURE 5 study, a total of 996 patients were randomised at baseline as follows: secukinumab 300 mg (N=222), secukinumab 150 mg LD (N=220), secukinumab 150 mg NL (N=222) and placebo (N=332). Demographics and baseline characteristics of the overall population were previously reported and balanced between treatment arms.13
Of the randomised patients, 213 (21.4%) patients discontinued before or at week 104, with the most common reasons being patient/guardian decision (7.8%) and adverse events (AEs; 6.2%). Discontinuation due to lack of efficacy was reported in 1.4%, 1.8% and 7.7% of patients in the secukinumab 300 mg, 150 mg LD and 150 mg NL groups, respectively. The disposition of patients up to week 104 has been reported previously13 and is also presented in online supplemental figure 2.
Baseline characteristics of patients who did or did not achieve sustained LDA according to DAPSA criteria or MDA response are presented in table 1. A higher proportion of patients who achieved sustained LDA according to DAPSA LDA+REM status were male, younger, had lower body mass index (BMI), a shorter duration of PsA and were TNFi-naïve. In addition, they had overall a less severe active disease characterised by a lower number of tender joints, lower frequency of enthesitis and dactylitis, lower disability and PsA pain, and lower systemic inflammation, at baseline than those who did not achieve this target/response. However, skin psoriasis was more frequent in the patients who achieved sustained DAPSA LDA+REM status versus those who did not. Similar findings were observed in patients who achieved sustained LDA according to MDA response, except that dactylitis was seen more commonly in patients with sustained response than those without (table 1). Similar trends were also observed in patients who achieved REM versus those who did not (data not shown).
Baseline demographics and clinical characteristics in patients who did or did not achieve sustained LDA according to DAPSA LDA or MDA response
Achievement of sustained LDA/REM by week 104
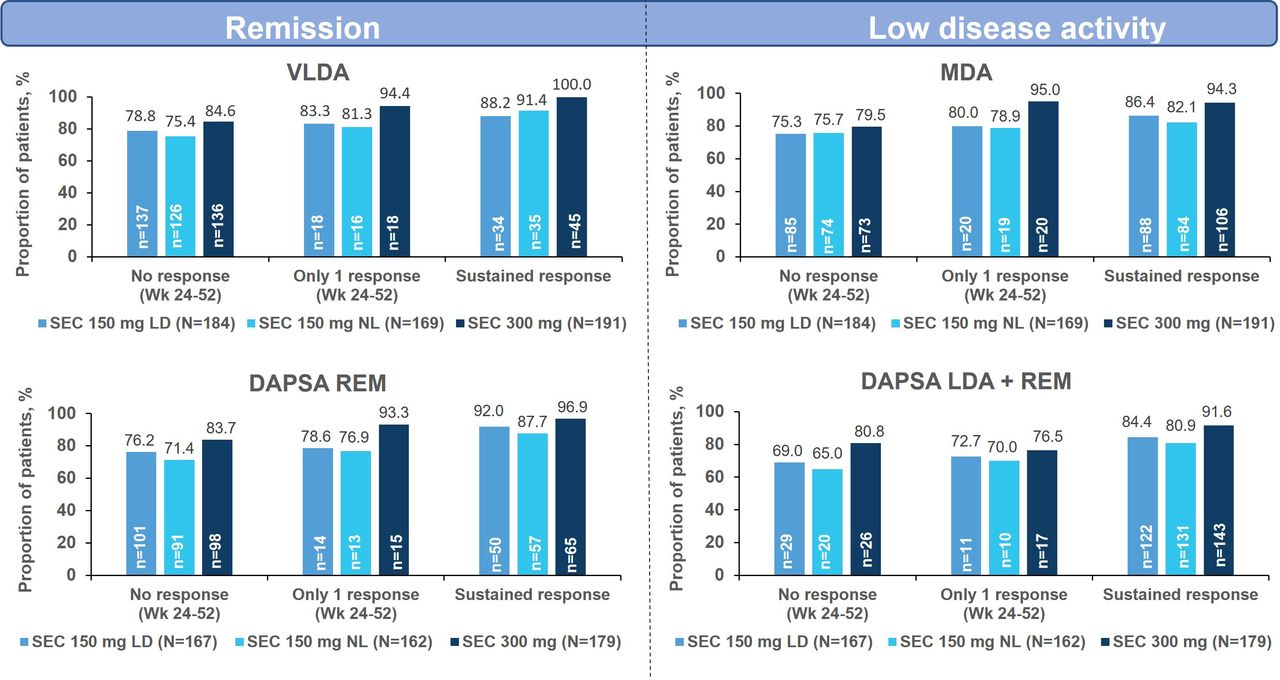
While a majority of patients treated with secukinumab could achieve either sustained MDA or sustained DAPSA LDA+REM, a relatively lower proportion of patients could achieve sustained REM according to VLDA (19%–24%) or DAPSA REM (30%–36%) as presented in figure 1. A lower proportion of secukinumab-treated patients achieved MDA/VLDA than DAPSA LDA+REM/DAPSA REM, which is consistent with previous reports, thus highlighting more stringency of MDA and VLDA versus DAPSA LDA+REM and DAPSA REM (figure 1).
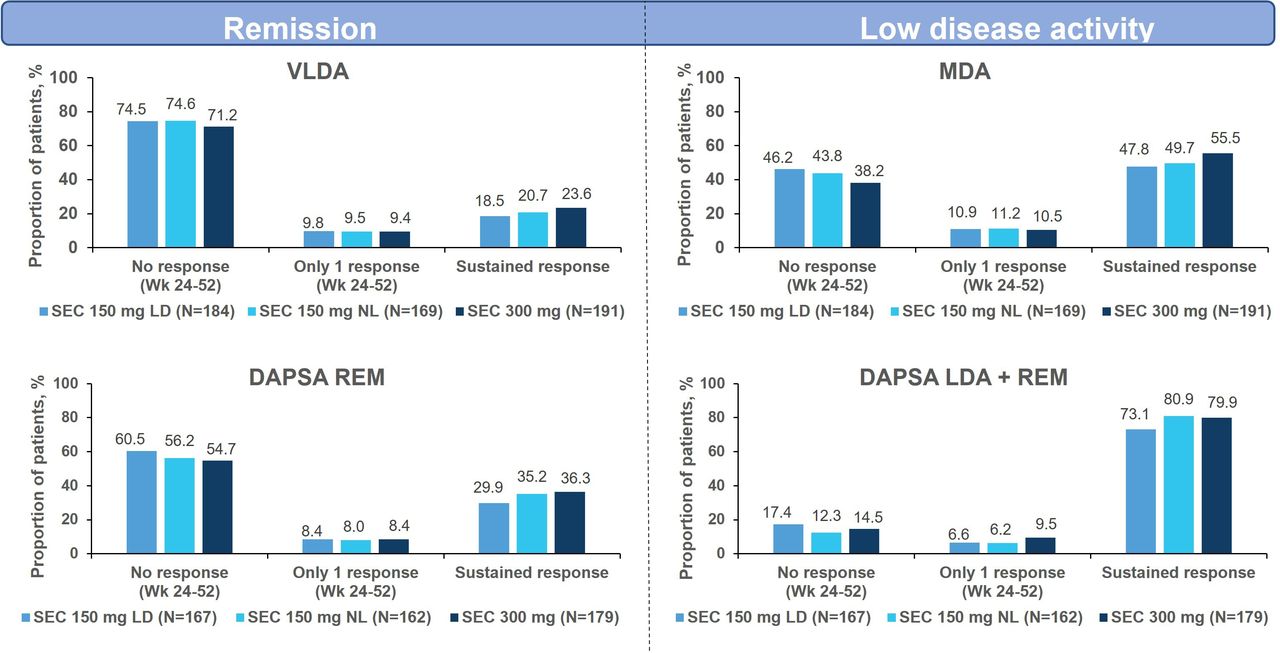
Proportion of patients achieving LDA/REM through week 104. Sustained LDA/REM was defined as achievement of the same response in at least two out of the next six visits (visits every 8 weeks). DAPSA, Disease Activity index in Psoriatic Arthritis; LD, loading dose; LDA, low disease activity; MDA, minimal disease activity; N number of patients with assessment at both weeks 24 and 104; NL, without loading dose; REM, remission; SEC, secukinumab; VLDA, very low disease activity; Wk, week.
Impact of sustained DAPSA LDA+REM/DAPSA REM on physical function through week 104
Patients with sustained DAPSA LDA+REM or DAPSA REM had a numerically greater improvement in physical function (HAQ-DI) when compared with patients who had not achieved this or only achieved this once, although changes in HAQ-DI reached minimal clinically important difference (MCID) for all. Moreover, patients with sustained DAPSA REM had a larger magnitude of improvement in function than patients with sustained DAPSA LDA+REM (figure 2).

Mean change from baseline to week 104 in HAQ-DI by LDA/REM and sustained LDA/REM status/response. Minimal clinically important difference (MCID)=−0.35. Baseline was defined as the last observation on the day of or before the first dose of the study drug. At each time point, only patients with a value at both baseline and that time point were included. Sustained LDA/REM was defined as achievement of the same response in at least two out of the next six visits (visits every 8 weeks). DAPSA, Disease Activity index in Psoriatic Arthritis; HAQ-DI, Health Assessment Questionnaire Disability Index; LD, loading dose; LDA, low disease activity; N, number of patients with assessment at both weeks 24 and 104; n, number of evaluable patients; NL, without loading dose; REM, remission; SEC, secukinumab; Wk, week.
Impact of sustained LDA/REM on HRQoL through week 104
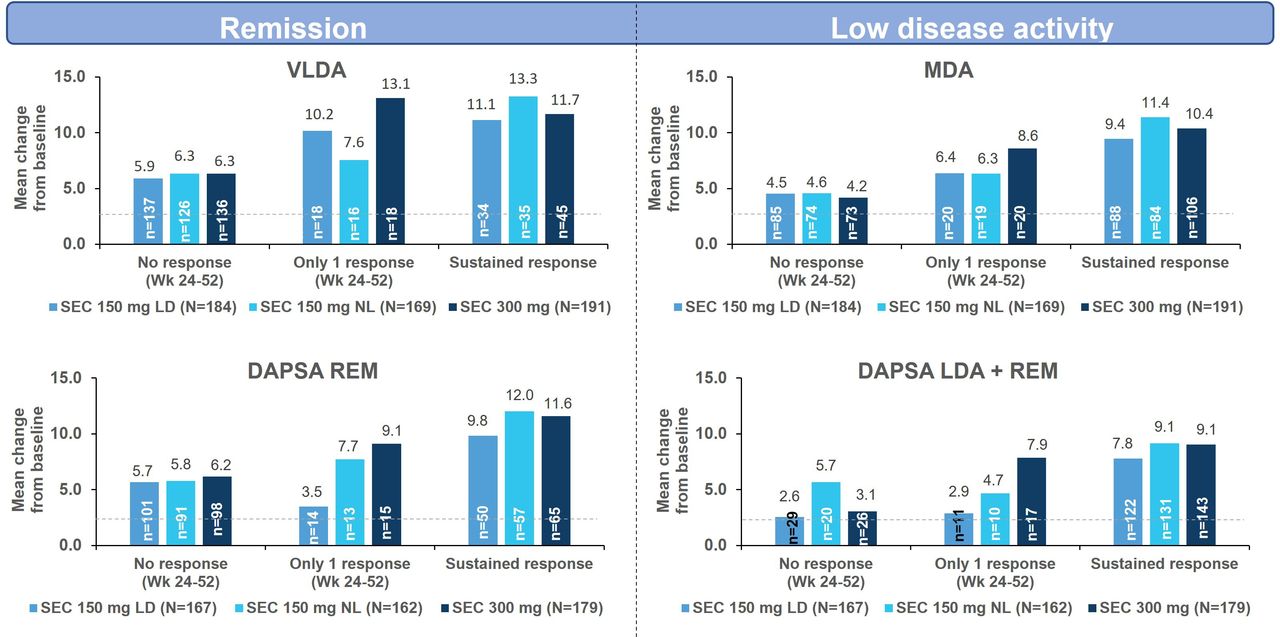
Consistent with changes observed in physical function, patients who had achieved sustained LDA or REM irrespective of the composite index selected experienced larger mean changes from baseline in HRQoL as assessed by SF36-PCS when compared with patients who had achieved this only once or who had not achieved it (figure 3). These changes also reached the MCID for SF36-PCS in all categories. Patients who reached sustained REM also had a higher numerical improvement in HRQoL than those who reached sustained LDA.

Mean change from baseline to week 104 in SF-36 PCS by LDA/REM and sustained LDA/REM status/response. Minimal clinically important difference (MCID)=2.5. Baseline was defined as the last observation on the day of or before the first dose of the study drug. At each time point, only patients with a value at both baseline and that time point were included. Sustained LDA/REM was defined as achievement of the same response in at least two out of the next six visits (visits every 8 weeks). DAPSA, Disease Activity index in Psoriatic Arthritis; LD, loading dose; LDA, low disease activity; MDA, minimal disease activity; N, number of patients with assessment at both weeks 24 and 104; n, number of evaluable patients; NL, without loading dose; REM, remission; SEC, secukinumab; SF-36 PCS, Short Form-36 Physical Component Summary Score; VLDA, very low disease activity; Wk, week.
Radiographic progression and sustained LDA/REM at week 104
The mean change in mTSS from baseline to week 52 and week 104 showed lower radiographic progression scores in secukinumab-treated patients across the different disease activity measurements (online supplemental table 1). Moreover, a high proportion of patients did not show any radiographic progression from baseline to week 104 irrespective of achievement of sustained LDA or REM category (figure 4).
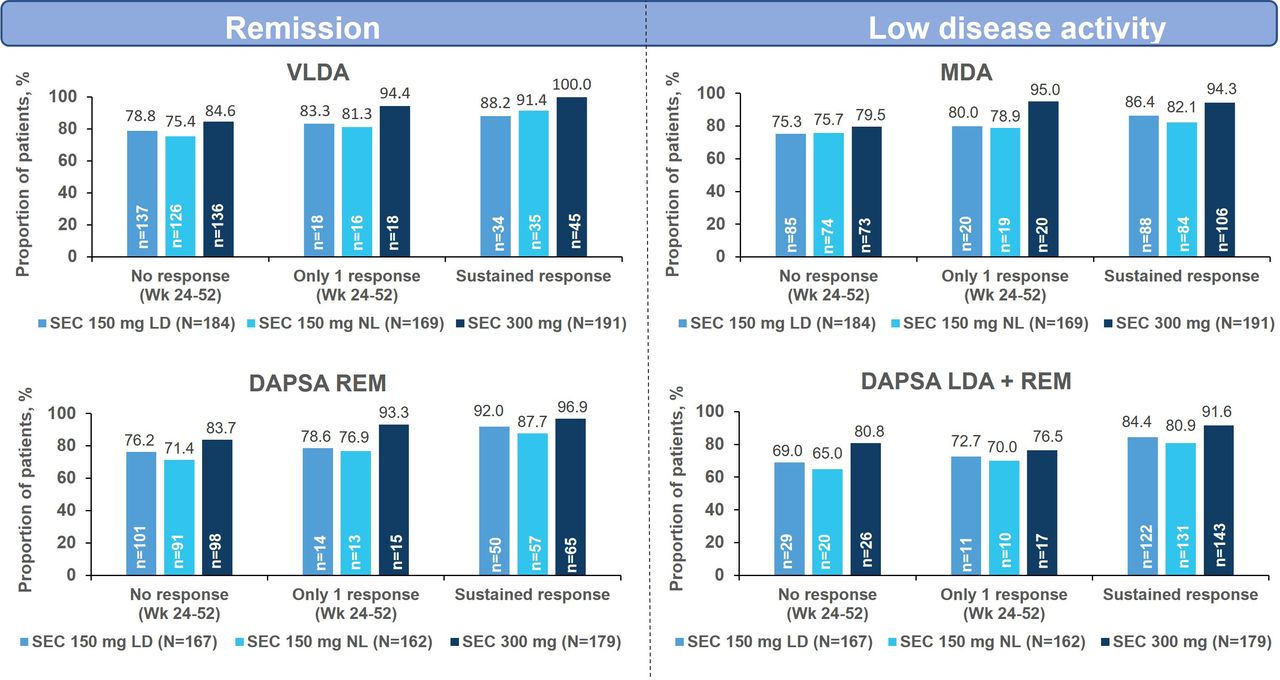
Percentage of vdH-mTSS non-progressors by LDA/REM and sustained LDA/REM status/response at week 104. Baseline was defined as the last observation on the day of or before the first dose of the study drug. At each time point, only patients with a value at both baseline and that time point were included. Sustained LDA/REM was defined as achievement of the same response in at least two out of the next six visits (visits every 8 weeks). vdH-mTSS was defined as change from baseline in mTSS≤0.5. DAPSA, Disease Activity index in Psoriatic Arthritis; LD, loading dose; LDA, low disease activity; MDA, minimal disease activity; N, number of patients with assessment at both weeks 24 and 104; n, number of evaluable patients; NL, without loading dose; REM, remission; SEC, secukinumab; vdH-mTSS, van der Heijde-modified Total Sharp score; VLDA, very low disease activity; Wk, week.
Multivariate analysis on predictors of response of sustained LDA
Multivariate logistic regression analysis showed that patients with low BMI at baseline, a reduction in TJC and decrease in pain at week 16 were more likely to achieve sustained DAPSA LDA+REM or sustained MDA. In addition, younger patients were also more likely to achieve sustained MDA response. In contrast, patients who were TNFi-naïve, had enthesitis and higher disability scores at baseline were less likely to achieve sustained LDA by either measure (figures 5 and 6).
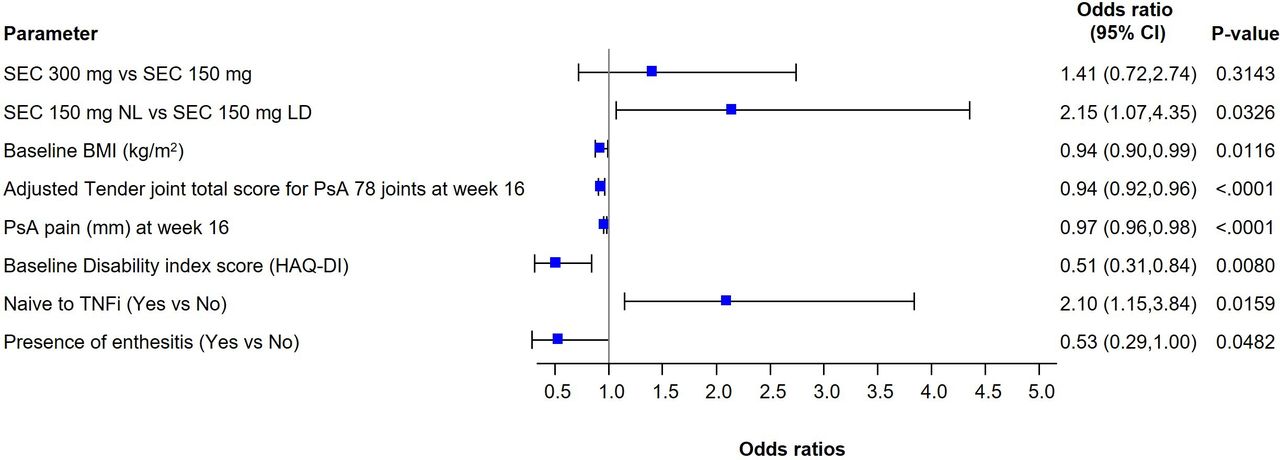
Forest plots of ORs for sustained DAPSA LDA+REM response at week 24 and week 104. Multivariate logistic regression model was fitted using sustained DAPSA LDA+REM response at least three times between week 24 and week 104 as outcome variable; covariates included treatment group, baseline BMI (kg/m2), adjusted TJC for PsA (78 joints) at week 16, PsA pain (mm) at week 16, baseline HAQ-DI, TNFi-naïve and presence of enthesitis. P values are all nominal. BMI, body mass index; DAPSA, Disease Activity index in Psoriatic Arthritis; HAQ-DI, Health Assessment Questionnaire-Disability Index; LD, loading dose; LDA, low disease activity; NL, without loading dose; OR, odds ratio; PsA, psoriatic arthritis; REM, remission; SEC, secukinumab; TJC, tender joint count; TNFi, tumour necrosis factor inhibitor.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots of ORs for sustained MDA response at week 24 and week 104. Multivariate logistic regression model was fitted using sustained MDA response at least three times between week 24 and week 104 as outcome variable; covariates included treatment group, age (years), baseline BMI (kg/m2), PsA pain (mm) at week 16 and adjusted TJC for PsA (78 joints) at week 16. P values are all nominal. BMI, body mass index; LD, loading dose; MDA, minimal disease activity; NL, without loading dose; OR, odds ratio; PsA, psoriatic arthritis; SEC, secukinumab; TJC, tender joint count.
Discussion
The 2-year large phase 3, randomised, double-blind FUTURE 5 trial with active PsA treated with secukinumab provided an opportunity to explore the proportion of secukinumab-treated patients who could achieve a stringent treatment goal in line with EULAR and updated GRAPPA recommendations 2021 and characterised by either sustained DAPSA LDA+REM/MDA or sustained DAPSA REM/VLDA over 2 years which is more rigorous than the primary and key secondary efficacy objectives of most therapeutic studies in PsA used in the past.17–19
The composite index MDA is a comprehensive measure focusing on multiple domains on PsA and HAQ-DI and is a clinically meaningful endpoint to assess the impact of interventions on disease activity. It has been validated in both clinical trials and real-world evidence settings. The DAPSA is another very frequent and validated composite index used for the assessment of disease activity in patients with PsA in both clinical trials and clinical practice focusing on the joint domain, and is sensitive to change in clinical trial and observational studies.20 Secukinumab-treated patients had significantly higher MDA response rates compared with those receiving placebo in the short-term period (week 16), with sustained responses over 2 years that were comparable with those previously reported in FUTURE 2 trial.21 However, sustainability of the MDA response across different visits was never previously assessed in secukinumab trials.
The current analysis highlights that the majority of patients treated with secukinumab 150 mg or 300 mg were able to achieve sustained LDA irrespective of the composite index selected, whereas only 19%–36% of patients were able to achieve sustained REM by week 104. Various post hoc analysis from clinical trials of TNFi (golimumab, adalimumab) have reported data on sustained LDA using different definitions and different composite indices.22–24
The observed sustained MDA range over 2 years in this trial is consistent with existing literature that reported sustained MDA within the range of 9%–43%.24–27 However, a higher rate of sustained DAPSA LDA+REM (73%–81%) was observed in this study likely due to the less stringent composite index than MDA. This adds to the body of evidence that long-term sustained LDA is achievable with secukinumab in the majority of patients with established PsA.
Among the composite indices evaluated, MDA and VLDA appeared to represent more stringency compared with DAPSA LDA+REM and DAPSA REM, with a slightly higher level of residual disease activity observed with DAPSA, consistent with data from the FUTURE 2, FUTURE 5 and GO-REVEAL studies.4 22
This exploratory analysis also aimed to investigate the different benefits of sustained LDA or REM in patients with PsA treated with secukinumab on physical function, HRQoL and inhibition of structural damage progression. The descriptive analysis on the relationship between improvement of function and HRQoL, and sustained LDA or REM tend to show numerically greater benefits in sustaining REM than LDA. However, the differences between the two disease states were small and the level of improvement was far beyond MCID across these two categories. This suggests that sustained LDA may already be associated with substantial benefits in terms of function and HRQoL and the differences between the two categories may not be clinically meaningful. At present, there is not enough evidence from the patient’s perspective to suggest whether these small differences could be translated into additional clinical benefit in terms of HRQoL and physical function as compared with those achieving sustained LDA. Nevertheless, as only a small proportion of patients are able to maintain sustained REM, achieving sustained LDA could be an acceptable target for most patients with established PsA as observed in FUTURE 2 study and previous studies with TNFi and other therapies.4 20 24 28 29
In this study, no clear relationship between inhibition of structural damage and the different disease states in secukinumab-treated patients was observed as the mean change in mTSS from baseline to week 52 and week 104 remained low across the different disease activity categories. Furthermore, a vast majority of secukinumab-treated patients were non-structural damage progressors at week 104 irrespective of the level of disease activity. Thus, there is a potential ‘disconnect’ between disease activity and radiographic progression, highlighting that secukinumab may have a protective effect on structural damage progression in PsA that is independent of achievement of sustained LDA or REM. This was also observed in previous adalimumab30 31 and golimumab studies23 in PsA patients. In the ADEPT trial, changes in mTSS were significantly lower with adalimumab, even in patients having moderate or high disease activity or not achieving MDA. Moreover, disease activity correlated significantly with radiographic progression in patients receiving placebo, but not patients receiving adalimumab, thus suggesting a ‘disconnect’ in patients treated with adalimumab.30 Similarly in the GO-VIBRANT trial, golimumab-treated patients exhibited less radiographic progression regardless of composite index or disease activity state achieved.23 Patients with rheumatoid arthritis have also reported this ‘disconnect’ phenomena with other TNFi therapies, abatacept and IL-6i.32–35
In this study, patients who achieved sustained LDA were younger, more frequently male, had a shorter time since diagnosis and presented with milder disease than those who did not achieve this target. This observation is in line with other studies reporting similar baseline characteristics.26 36 We also explored the potential role of several demographic, clinical and systemic parameters as predictive factors of sustained clinical LDA. Predictors of response of sustained MDA and DAPSA LDA+REM were mostly similar and included younger patients with less active disease, which is partly consistent with those observed in clinical trial settings.24 Further, the present analysis also found that the odds of achieving sustained DAPSA LDA+REM or MDA was lower in patients with higher BMI at baseline, which is consistent with the limited efficacy of other biologics described in the literature in case of high BMI.25 37 In contrast, patients who were TNFi-naïve, had enthesitis and higher disability at baseline were less likely to sustain DAPSA LDA+REM. Similar findings were observed in the GO-REVEAL study which demonstrated a lower likelihood of achieving MDA (≥3 time points) in patients with a one-unit higher baseline HAQ-DI score.22
The potential limitations of the current analysis include its post hoc nature, as the study was not primarily designed as a T2T study and the retrospective analysis of targets. In addition, there was a lack of a long-term comparator given that the placebo-controlled period of the core FUTURE 5 study was only up to week 24 due to ethical considerations. Considering the achievement of stringent outcomes like LDA/REM, the study did not evaluate the relationship between these stringent outcomes from study start. As such, the inhibition of structural damage progression if related to more stringent outcomes may only occur later when there is no placebo. Moreover, in the FUTURE 5 study, secukinumab uptitration from 150 mg to 300 mg was done in patients from week 52, which may limit the interpretation of incremental benefit between 150 mg and 300 mg doses at week 104. Furthermore, MDA is a composite response achieved by meeting 5 of 7 possible criteria, and we do not discern if any of the seven criteria are more important in achieving MDA than others. Consequently, MDA also includes HAQ as one of the components and one cannot evaluate the impact of physical function using HAQ as a separate assessment in patients achieving MDA. Finally, the study duration was limited to only 2 years. Further long-term studies could provide more data on maintaining REM and its impact on QoL and structural outcomes in patients with PsA.
In conclusion, these analyses provide further insights into the long-term achievement of LDA or REM in patients treated with secukinumab which is associated with better long-term function and PRO benefits. The study also highlights the protective effect of secukinumab on inhibition of structural progression irrespective of the level of disease activity. Patients who sustain these stringent outcomes tend to be younger, with low BMI and milder disease which emphasises the need for early intervention in terms of diagnosis and management of the disease.
Data availability statement
Data are available on reasonable request. Data may be obtained from a third party and are not publicly available. The datasets generated and/or analysed during the current study are not publicly available. Novartis is committed to sharing with qualified external researchers access to patient-level data and supporting clinical documents from eligible studies. These requests are reviewed and approved on the basis of scientific merit. All data provided are anonymised to respect the privacy of patients who have participated in the trial, in line with applicable laws and regulations. The data may be requested from the corresponding author of the manuscript. The protocol can be made available on request by contacting the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki. The study was approved by institutional review boards or independent ethics committees at each participating centre and are included in the manuscript. Written informed consent was obtained from all enrolled patients. Data were collected in accordance with the Good Clinical Practice guidelines by the study investigators and were analysed by the sponsor. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the patients who participated in this study and the study investigators for their contributions. The authors also thank Shreya Dam (Novartis Healthcare, Hyderabad, India) for providing medical writing support and Andrew Franklin (Novartis Pharma AG, Basel, Switzerland) for providing medical and editorial guidance in accordance with Good Publication Practice guidelines.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @drlauracoates
Contributors All authors were involved in the study design and/or collection, analysis and interpretation of the data, provided critical revision of the manuscript and approved the final version to be submitted for publication. LCC was responsible for overall content as the guarantor.
Funding This study was funded by Novartis Pharma AG, Basel, Switzerland.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests LCC is an associate editor for RMD Open and has received grants/research support from AbbVie, Amgen, Celgene, Eli Lilly, Janssen, Novartis, Pfizer and UCB; worked as a paid consultant for AbbVie, Amgen, Bristol Myers Squibb, Celgene, Eli Lilly, Gilead, Galapagos, Janssen, Moonlake, Novartis, Pfizer and UCB; and has been paid as a speaker for AbbVie, Amgen, Biogen, Celgene, Eli Lilly, Galapagos, Gilead, GSK, Janssen, Medac, Novartis, Pfizer and UCB. LCC is supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre (BRC). PJM has received research grants from AbbVie, Amgen, BMS, Celgene, Lilly, Galapagos, Gilead, Janssen, Novartis, Pfizer, Sun Pharma and UCB; consulting fees from AbbVie, Aclaris, Amgen, Boehringer Ingelheim, BMS, Celgene, Lilly, Galapagos, Genentech, Gilead, GlaxoSmithKline, Inmagene, Janssen, Novartis, Pfizer, Sun Pharma, and UCB; speakers’ bureau for AbbVie, Amgen, BMS, Celgene, Lilly, Janssen, Novartis, Pfizer, and UCB. DG has received grant/research support from: Amgen, AbbVie, Celgene, Eli Lilly, Janssen, Novartis, Pfizer and UCB. Consultant for: Amgen, AbbVie, BMS, Celgene, Eli Lilly, Gilead, Galapagos, Janssen, Novartis, Pfizer and UCB. SN has received consulting and speaker fees from Pfizer, Novartis, Janssen, Boehringer Ingelheim, Biogen, Glaxo Smith Kline. WB is an employee of Novartis with Novartis stock. CG is an employee of Novartis; Shareholder of Novartis and BMS.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.