Article Text

Abstract
Objective The clinical spectrum of primary antibody deficiencies (PADs) and especially common variable immunodeficiency (CVID) includes various autoimmune disorders. We studied the prevalence and the features of articular rheumatic disease in a cohort of patient with PADs.
Methods In this retrospective cohort study, complete clinical data of 268 patients with PADs, mainly consisting of patients with CVID, visiting the immunology outpatient clinic of a German tertiary hospital between 2018 and 2021 were collected. Those included case history, physical examination, laboratory as well as radiological findings.
Results Inflammatory arthritis was diagnosed in 16.4% of studied patients and was significantly more common among patients with PAD-associated enteropathy (OR 13.39, p=0.0001), splenomegaly (OR 6.09, p=0.0001) or atopic diseases (OR 3.31, p=0.021). Given HLA-B27 status, the involvement of the axial skeleton and the presence of features, such as anterior uveitis, inflammatory bowel disease, psoriasis and/or dactylitis, 75% of studied patients fulfilled the Assessment of Spondyloarthritis International Society classification criteria.
Conclusion PAD-associated arthritis frequently shares features with spondyloarthritis (SpA) and enteropathic arthritis. The latter may suggest the interconnected pathomechanisms of inflammatory arthritis in SpA and PADs.
- Arthritis
- Spondylitis, Ankylosing
- Autoimmunity
- Immune System Diseases
Data availability statement
Data are available for formal research purposes only upon request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Primary antibody deficiencies (PADs), especially common variable immunodeficiency, are often associated with autoimmunity, including rheumatic disorders.
WHAT THIS STUDY ADDS
This is the first study characterising the clinical spectrum of inflammatory arthritis in PADs.
Arthritis in PADs is classified as a spondyloarthritis (SpA) or an enteropathic arthritis in 75% of studied patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Association of inflammatory arthritis in PADs with PAD-related enteropathies lends credence to the gut–joint axis hypothesis, proposed for the pathogenesis of SpA.
The diagnosis of an underlying PAD may be considered in patients with an enteropathic arthritis.
Introduction
Primary antibody deficiencies (PADs) comprise a heterogeneous group of disorders characterised by ineffective humoral immunity.1 Besides recurrent infections, especially due to encapsulated bacteria such as Streptococcus pneumoniae and Haemophilus influenzae, PADs manifest with variable immune dysregulation, including allergy, granulomatous disease, autoimmunity, autoinflammation and benign lymphoproliferation.2 The common variable immunodeficiency (CVID) has an estimated prevalence of 1:10 000–1:100 000 and is considered the most prevalent symptomatic PAD disorder.3 Autoimmunity in CVID is heterogeneous and commonly manifests as an autoimmune cytopenia or an autoimmune endocrinopathy.3 4 Further, CVID is associated with rheumatic articular and connective tissue diseases.4 Rheumatic disorders and especially inflammatory arthritis have also been reported in X-linked agammaglobulinaemia (XLA) and isolated IgG subclass deficiency.5–8
Previous studies have reported a varying prevalence of inflammatory arthritis in CVID, ranging from 1% to 11.5% in different patient cohorts.9–12 Rheumatoid arthritis (RA) and juvenile idiopathic arthritis (JIA) have been commonly reported in CVID.12–14 Polyarticular JIA and RA have been reported to represent relatively common autoimmune manifestations in XLA and isolated IgG subclass deficiency, respectively.5–8 However, inflammatory arthritis remains a poorly characterised manifestation of PADs. In the present study, we aimed to establish the prevalence of inflammatory arthritis in a German cohort of patients with PADs and characterise its clinical, laboratory and radiological features.
Patients and methods
Study cohort
This single-centre retrospective study included a total of 268 patients with PAD visiting the immunology outpatient clinics of the department of rheumatology and immunology of the Hannover Medical School.
Data were collected from 2018 to 2021. Diagnosis of primary immunodeficiency was based on the current European Society for Immunodeficiencies diagnostic criteria (available at http://esid.org/Working-Parties/Registry/Diagnosis-criteria).15 Clinical data were obtained from patients’ medical files. PAD-associated phenotypes were documented as described previously.16 In particular, those included bronchiectasis (CT-confirmed), autoimmune cytopenias, such as autoimmune haemolytic anaemia (AIHA), idiopathic thrombocytopenic purpura (ITP), organ-specific autoimmunity (including vitiligo, psoriasis, insulin-dependent diabetes mellitus, thyroidopathies, atrophic gastritis and arthritis), granulomatous disease, enteropathy and malignancies. Interstitial lung disease (ILD) was diagnosed based on typical CT scan findings, in the absence of evidence for aninfectious or alternative cause. Splenomegaly was defined as spleen enlargement of ≥11 cm on palpation or ultrasound, including previous splenectomy of an enlarged spleen. Lymphadenopathy was detected on palpation, ultrasound, CT or magnetic resonance scan. Granulomatous disease was definedas at least one biopsy-proven unexplained granuloma, excluding Crohn’s disease-associated granulomas.Enteropathy included all cases of biopsy-proven non-infectious inflammatory bowel disease (IBD) (ulcerative colitis and Crohn's disease), coeliac disease, lymphocytic infiltration of the interepithelial mucous, the lamina propria and/or the submucosa, as well as patients with chronic idiopathic diarrhoea. Malignancies included haematological and all other forms of cancer.
Our cohort was screened for the diagnosis of arthritis (figure 1). Data regarding arthritis were obtained from clinical documentation of observed arthritis during patients’ physical examination by a rheumatologist. Diagnosed arthritis was characterised according to the affected joints. The diagnosis of spondyloarthritis (SpA), RA, psoriatic arthritis (PsA) or JIA was accepted when diagnosis was made by a rheumatologist and when the respective classification criteria were fulfilled: the Assessment of SpondyloArthritis International Society classification criteria for SpA,17 the American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria for RA,18 the Classification Criteria for Psoriatic Arthritis for PsA19 and the International League of Associations for Rheumatology classification of JIA.20

Study design. ASAS, Assessment of Spondyloarthritis International Society; CASPAR, Classification Criteria for Psoriatic Arthritis; CVID, common variable immunodeficiency; JIA, juvenile idiopathic arthritis; PAD, primary antibody deficiency; RA, rheumatoid arthritis; SpA, spondyloarthropathy; SPAD, specific polysaccharide antibody deficiency.
Available serological findings, including rheumatoid factor (RF) test, cyclic citrullinated peptide (CCP) antibodies and antinuclear antibodies (ANAs), as well as HLA-B27 antigen test and C reactive protein levels at diagnosis of arthritis, were documented. For patients with arthritis with unknown HLA-B27 status and available DNA probe, we tested for HLA-B27 by PCR. Radiological findings included X-rays and MRI scans of affected joints. Based on the age of onset of arthritis, involved joints, imaging and serological findings, as well as the diagnosis of psoriasis, IBD or an alternative enteropathy, we evaluated classification of arthritis into a known articular rheumatic disorder. Oligoarthritis was defined as arthritis of ≤4 joints, whereas polyarthritis was defined as arthritis affecting ≥5 joints.
Statistical analysis
For statistical calculations, we used GraphPad Prism V.9 (GraphPad, La Jolla, USA). Descriptive statistics are reported as median and IQR in case of continuous variables and as counts and percentages for dichotomous variables. Categorical variables were compared by the Fisher’s exact test. Differences between patients with and without arthritis were evaluated with the Mann-Whitney test. To correct for multiple testing, p values were adjusted for Benjamini-Hochberg false discovery rate (FDR). P values were considered significant if they were lower than a threshold selected to control an FDR of 5%. To evaluate the independent role of variables whose association with arthritis was considered significant in the univariable analysis, we performed multivariable logistic regression analysis.
Results
Characteristics of patients with PAD, prevalence of arthritis and arthritis-associated phenotypes
Patients’ demographic data and characteristics are summarised in table 1. Most patients had a late-onset PAD diagnosed as CVID (216/268, 80.6%). Except for recurrent infections, the majority (202/268, 75.4%) had at least one additional PAD-associated manifestation, which more commonly was an autoimmune disorder (118/268, 44%). Among autoimmune disorders, autoimmune cytopenias were the most prevalent, diagnosed in 45/268 patients (16.8%). Those included ITP in 37/268 patients (13.8%), AIHA in 15/268 patients (5.6%) and autoimmune neutropenia in 2/268 patients (0.7%). With respect to arthritis, except for the case of a patient with XLA who suffered from a septic pneumococcal arthritis at first diagnosis of agammaglobulinaemia and a patient with a late-onset combined immunodeficiency with septic spondylodiscitis, all other cases were diagnosed with inflammatory arthritis. The prevalence of inflammatory arthritis was similar to the one of autoimmune cytopenias (44/268, ie, 16.4%). Female and male patients were equally likely to develop inflammatory arthritis (27/128 vs 17/93, p=0.7391; OR 1.15, 95% CI 0.59 to 2.24). Overall, in 14/44 cases (31.8%) with manifestation of arthritis preceded the diagnosis of PAD. Among PAD-associated manifestations, the diagnosis of arthritis was significantly more common among patients with splenomegaly, enteropathy or an atopic disease (table 2 and online supplemental table 1). All three, splenomegaly, enteropathy and the presence of an atopic disease, were independently associated with the diagnosis of arthritis (online supplemental table 2). We identified no association with psoriasis or infectious manifestations, including gastrointestinal infections. Among diagnosed enteropathies, Crohn’s disease was significantly more common among patients with arthritis (7/44 vs 1/224, p<0.0001; OR 42.2, 95% CI 7 to 477).
Supplemental material
Characteristics of studied patients with PADs
Association of infectious and non-infectious manifestations of PADs with inflammatory arthritis.
Clinical subgroups of inflammatory arthritis in pads and CVID
A total of 21/44 (47.7%) cases had oligoarthritis and 23/44 (52.3%) were diagnosed with polyarthritis. The pattern of articular involvement, as well as all relevant extra-articular manifestations for all 44 patients with arthritis, is presented in table 3. Based on the pattern of affected joints, on HLA-B27 positivity and extra-articular disease, such as psoriasis and IBD, arthritis could be classified as a SpA in 31/44 patients (75%) (figure 2A). Those included eight patients with axial spondyloarthritis (axSpA) who displayed sacroiliitis, confirmed through radiographic and/or MRI. In particular, 3/8 patients displayed radiological findings consistent with the diagnosis of radiographic axSpA or ankylosing spondylitis (AS), whereas the rest (ie, 5/8) were diagnosed with a non-radiographic axSpA. A total of 4/44 patients (9.1%), all with a concomitant plaque psoriasis, and 1, who in addition to plaque psoriasis displayed nail psoriasis, fulfilled the classification criteria for PsA. Further, 4/44 patients (9.1%) with early-onset of arthritis, prior to the age of 16 years, could be diagnosed with JIA. Reactive arthritis was diagnosed in 3/44 patients (6.8%) and followed in all three of them an acute gastrointestinal infection.
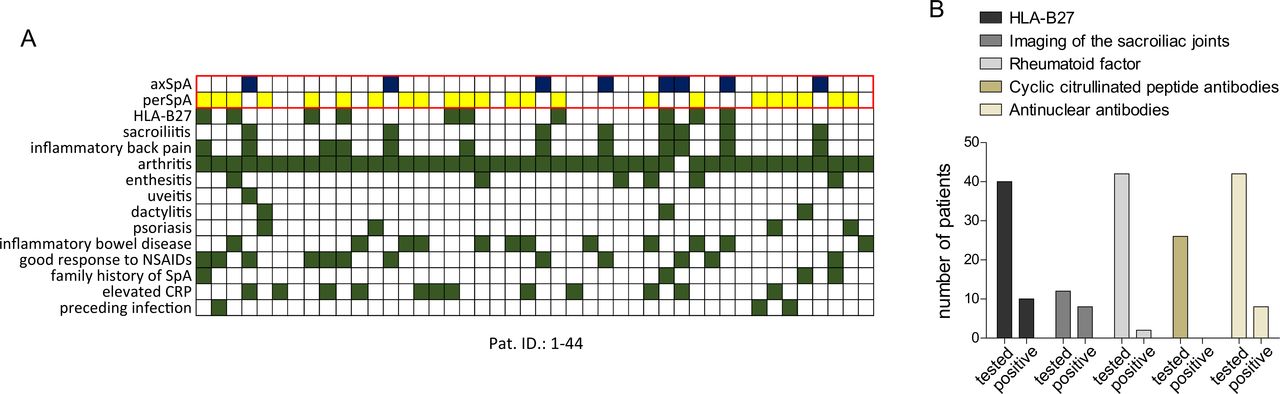
(A) Summary of ASAS classification criteria, evaluated in 44 patients with arthritis and PAD. Green boxes indicate a fulfilled ASAS criterion, whereas blue and yellow boxes indicate fulfilled criteria for the diagnosis of an axSpA and a perSpA, respectively. Each map column matches a studied patient with arthritis (1–44; see table 3). (B) Arthritis workup, available imaging and laboratory investigations. ASAS, Assessment of Spondyloarthritis International Society; axSpA, axial spondyloarthritis; CRP, C reactive protein; PAD, primary antibody deficiency; perSpA, peripheral spondyloarthritis.
Clinical description of arthritis
As discussed previously, 33/44 patients with arthritis (75%) had an enteropathy. The subgroup of patients with enteropathy included 12/33 with IBD (6/11 with Crohn’s disease and 6/11 with undifferentiated colitis). A total of 7/33 patients had a biopsy-proven nodular lymphoid hyperplasia (NLH). In addition, two patients were diagnosed with seronegative coeliac disease and the remaining 14 patients had chronic non-infectious diarrhoea, without clear endoscopic or histological evidence for the diagnosis of IBD, NHL or coeliac disease. Arthritis in patients with IBD or an alternative enteropathy may be falling under an enteropathic arthritis.21
In addition to typical extra-articular manifestations of SpA, such as psoriasis, dactylitis and IBD, 3/44 patients reported Raynaud’s phenomenon (patients 15, 17 and 41), which may suggest arthritis in the context of a connective tissue disease such as systemic lupus erythematosus (SLE), systemic sclerosis (SSc) or Sjögren’s syndrome (SjS).22 Those three patients, displayed in addition a positive ANA test that would be consistent with the diagnosis of one of the aforementioned connective tissue diseases. However, the rest of relevant classification criteria were not fulfilled.23–25 Further, 2/44 reported sicca symptoms and displayed a pathological Schirmer’s test (patients 21 and 40) that may suggest the diagnosis of SjS.25 Both of them displayed no ANA or other relevant autoantibodies, and labial salivary biopsy, performed in one of them, was not showing lymphocytic foci and was therefore not in line with the diagnosis of SjS. The presence of SpA-associated manifestations, such as sacroiliitis, dactylitis and IBD (table 3), was rather suggestive of articular inflammation in the context of a SpA in four of previously discussed patients with either Raynaud’s phenomenon or sicca symptoms.
Laboratory findings in patients with PAD with arthritis
Serological investigations are not considered helpful in differentiating arthritis in patients with PAD. Only 2 out of 42 tested patients were RF positive (figure 2A). In one of them (patient 13), sacroiliitis deviated from the joint involvement pattern of a RA, whereas the other (patient 28) had an early-onset arthritis, which was classified as JIA. CCP antibodies were negative in all 26 tested patients. A total of 8 out of 42 studied patients displayed an ANA titre higher than 1:160, and 3 of them displayed a titre higher than 1:320, though in the case of 3/8 patients ANA test has been performed after introduction of immunoglobulin replacement treatment, which may have affected ANA positivity and titre. None of the patients had antibodies against extractable nuclear antigen. Overall, among patients with positive ANA test, the presence of axial joint inflammation or IBD deviated from a typical connective tissue disease-associated arthritis. Ten out of 40 tested patients were HLA-B27 positive (figure 2B). Two out of the 10 patients that were HLA-B27 positive (figure 2A) had an axSpA, including sacroiliitis, whereas the rest were diagnosed with a peripheral SpA. Relatively higher immunoglobulin levels, especially IgA levels, have been long ago reported in patients with AS.26 27 Evaluation of the serum immunoglobulin levels at diagnosis of PAD revealed significantly higher IgG values in the subgroup of patients with inflammatory arthritis (p=0.004), whereas IgA and IgM levels were similar between patients with arthritis and those without (figure 3).

{kind=link}
{kind=link}
{kind=link}
Immunoglobulin levels at diagnosis of primary antibody deficiency, prior to the introduction of immunoglobulin replacement treatment (**, p<0.01).
Treatment of arthritis in patients with PADs
A total of 39/44 patients (88.6%) with arthritis were receiving an immunoglobulin replacement therapy. A total of 34/44 patients (77.3%) were on treatment with non-steroidal anti-inflammatory drugs (NSAIDs), prednisolone or various disease-modifying antirheumatic drugs (DMARDs), at last follow-up during the study. In two patients (ie, patients 21 and 23), current immunomodulatory treatment has been primarily commenced to treat ILD. In the remaining 32/44 of patients, arthritis was the reason for treatment with either NSAIDs, prednisolone or a DMARD. Eight out of 44 patients (18.2%) were receiving an NSAID monotherapy. Ten out of 44 patients (22.7%) were treated with a conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), most commonly hydroxychloroquine and methotrexate (MTX). A total of 11/44 patients were on a biological disease-modifying antirheumatic drug (bDMARD) treatment, including 4/44 on a TNF-inhibitor and 3 patients (including patient 21 with a concominant ILD) on rituximab. Anti-inflammatory treatments of patients with arthritis are summarised in table 3. Infectious complications after immunomodulatory treatment for arthritis included oral candidiasis in one patient, during treatment with high-dose steroids and MTX (patient 4) and recurrent oral candidiasis in a patient receiving secukinumab (patient 31), which led to prophylactic treatment with fluconazole. This patient also displayed a higher frequency of sinusitis and bronchitis, which led to antibiotic prophylactic treatment with azithromycin. Further, an additional patient (patient 28) reported a higher frequency of infections during treatment with prednisolone and MTX. The aforementioned anti-inflammatory regimen was ineffective in treating this patient’s polyarthritis and was therefore switched to rituximab, which enabled prednisolone tapering.
Discussion
Rheumatic manifestations and especially arthritis have been variably reported as autoimmune manifestations of PADs.12 14 28 In the present retrospective study, in a cohort of patients with PAD, the prevalence of inflammatory arthritis amounted to approximately 16%, which is higher than previously reported.9–12 The latter might be explained through selection bias, due to the fact that our outpatient clinic is a tertiary referral centre both for rheumatic disorders and primary immunodeficiency disorders (PIDs). We further aimed at providing a comprehensive characterisation of the course, the pattern of articular involvement and the associated extra-articular manifestations of inflammatory arthritis. Among established rheumatological entities characterised by articular inflammation, we find that PAD-associated arthritis can be commonly classified as SpA. Clinical features such as anterior uveitis, psoriasis, enthesitis, dactylitis and/or the coexistence of IBD mainly accounted for that. Further, association of arthritis with an enteropathy may represent a feature overlapping with enteropathic arthritis, especially in the subgroup of patients with IBD. In addition to enteropathy, arthritis associated with the presence of splenomegaly, which comes in line with previous reports associating autoimmunity with splenomegaly in CVID.29 30
Inflammatory arthritis represents the most common extra-articular manifestation of IBD.31 Further, the observation that arthritis can be the consequence of gastrointestinal infection in genetically predisposed subjects has provided an additional link between gastrointestinal and articular inflammation.32 Besides IBD-associated arthritis and postenteritis reactive arthritis, other gastrointestinal conditions, such as coeliac disease, Whipple disease and intestinal bypass, are associated with arthritis, highlighting a link between the gut and articular inflammation.32 33 Although the precise aetiology of arthritis in each of the aforementioned conditions remains unknown, they cumulatively suggest a gut component in its pathogenesis, entailing the interplay of microbial factors with host factors, which may result in bacterial overgrow, dysbiosis as well as in gastrointestinal inflammation and gut barrier dysfunction.
Gut microbiota and the integrity of the gut barrier have been suggested to contribute the development of arthritis, also in the absence of a manifest gastrointestinal condition.34–37 In RA, enhanced gut permeability has been reported to correlate with disease onset and activity as well as with tumour necrosis factor (TNF) inhibitor-induced remission, providing a likely mechanistic link between gut microbiota and articular inflammation. Changes in the composition of the gut microbiome have been reported in faecal and biopsy samples from patients with SpA, and the abundance of particular bacteria has been associated with disease activity.38 Further, in ileal biopsies from patients with SpA, the presence of adherent and invading bacteria associated with decreased expression of tight junction components.39 The latter, together with similar findings in HLA-B27 rats, suggests the relevance of dysbiosis and impaired gut barrier function in the pathogenesis of inflammation in SpA.38–40
Gastrointestinal inflammation is common in patients with PADs, and nearly half of patients with CVID with gastrointestinal symptoms who have undergone colonoscopy have been reported to display a non-infectious pathology, including NLH, microscopic colitis and IBD.41 42 Bacterial dysbiosis has been also identified in CVID, though evidence on its role in the pathogenesis of autoimmunity remains scarce.43 PAD-associated dysbiosis may stem from decreased secretory IgA, infections, antibiotics as well as dietary factors.43–45 In addition, microbial-related as well as the PAD-intrinsic antibody failure and associated enteropathies may compromise anatomical containment of commensal organisms in the gut.43 The latter may result in release of microbiota-derived products into the systemic circulation and consequently in systemic innate immune activation and higher risk for inflammatory complications, including arthritis.44 Given the aforementioned discussed association of both SpA and CVID with gut inflammation and gut dysbiosis, our observation that hypogammaglobulinaemic arthritis associates with enteropathy may extend the relevance of the gut–joint axis hypothesis to PAD-associated inflammatory arthritis.
The strong association of immunodeficiency with autoimmunity suggests that pathogenic pathways of immunological disorders can overlap.46 Those include defects in molecules with pleiotropic roles within the immune system or B cell-intrinsic and especially T cell-intrinsic defects may account for both immunodeficiency and autoimmunity. Impaired response to infections could also account for autoimmunity through diverse pathomechanisms, including molecular mimicry, superantigen-induced immune activation, release and enhanced presentation of self-antigens. 46 47 The role of altered microbiota and impaired gut barrier may represent an additional mechanism of autoimmunity in PADs, which needs to be further investigated.
We finally found an association between atopic diseases and inflammatory arthritis in PADs. Focusing on each of the relatively common atopic diseases in our cohort, all three allergic rhinitis, atopic dermatitis and allergic asthma tended to be associated with arthritis. However, the role of each allergic condition needs to be evaluated in larger cohorts of patients with PAD. Several previous studies have evaluated the association between atopy and rheumatic disorders. Retrospective studies have demonstrated the association of asthma, atopic dermatitis and allergic rhinitis with RA.48–50 Further, AS has been reported to be associated with increased risk for atopic disease in the form of asthma and allergic rhinitis.51 Shared risk factors including genetic and environmental factors, such as smoking as well as overlapping pathomechanisms of immune dysregulation, including enhanced Th2 or Th17 diffetentiation and epithelial barrier dysfunction, may be relevant for the association of allergy with inflammatory arthritis.50
Treatment of arthritis was the same as in other rheumatological disorders and depended on the presence of axial joint inflammation as well as on comorbidities, such as ILD or IBD. In approximately 22% of studied patients, arthritis displayed a sustained remission in the absence of an anti-inflammatory treatment, which would be consistent with a self-limiting or monophasic disease course. Further, only in the case of a single patient anti-inflammatory arthritis was modified due to the activity of arthritis, which suggests a satisfactory therapeutic efficacy of chosen treatments. However, the possibility of avoiding DMARD treatment in patients with residual arthritis activity for fear of severe infections cannot be excluded,52 as standard measures for the evaluation of arthritis activity, such as the patient global assessment of disease activity or functional questionnaires, were not available. Further, prospective documentation of infectious manifestations under treatment with diverse csDMARDs and bDMARDs would clarify the influence of immunomodulatory treatment on infectious susceptibility in patients with PIDs.
Standard laboratory work-up of inflammatory arthritis included the measurement of autoantibodies, such ANA and RF as well as HLA-B27 test. Among patients with arthritis, the positivity rate of HLA-B27 amounted 25% and was therefore higher than the previously reported positivity of 10% in the German population.53 However, among the seven tested patients with axSpA, only two patients harboured HLA-B27, which suggests that susceptibility to arthritis including axial joint inflammation cannot be explained through HLA-B27 in the majority of patients with arthritis. Serological tests are of limited diagnostic value in patients with PAD, which—considering the present study—can be expanded to the differentiation of arthritis. However, the loss of antibody responses, which usually is an intrinsic feature of PADs, may have biased arthritis classification towards seronegative SpA. ANA positivity was in most cases due to a low antibody titre and could in case of some patients suggest the diagnosis of connective tissue disease, such as SLE or SSc, though relevant criteria were not fulfilled.
Our study has several limitations. As discussed previously, high frequency of inflammatory arthritis may reflect a selection bias due to fact that the present study has been conducted in a tertiary centre, which may result in under-representation of the ‘infections-only’ subgroup of patients. In addition, factors intrinsic to the retrospective study design affected evaluation of the therapeutic efficacy and tolerability of drugs employed to treat arthritis. Evaluation of tolerability would be especially relevant in view of the immunosuppressive effect of diverse csDMARDs and dDMARDs, which may worsen the PAD-intrinsic immunodeficiency.54,41 In the present study, only a minority of patients developed infectious complication as a consequence of their arthritis treatment, which may underestimate the impact of DMARDs and their immunosuppressive effect on patients’ immunodeficiency. The latter may depend on several parameters, including concomitant glucocorticoid treatment, the type of PAD as well as the vaccination status of tested patients, which should be evaluated through perspective studies with large numbers of treated patients.
In summary, our findings suggest that inflammatory arthritis is a common phenotypical trait of PADs. The PAD-intrinsic tendency to seronegative disease, together with the extra-articular manifestations associated with arthritis in PAD, represents features that overlap with SpA. Especially the association of arthritis in PADs with enteropathies suggests the likely pathogenic relevance of the gut–joint axis hypothesis, which needs to be further investigated.
Data availability statement
Data are available for formal research purposes only upon request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study was conducted in accordance with the Declaration of Helsinki and was also approved by the ethical committee of the Hannover Medical School (approval number 5582; 8875_BO_K_2020). All patients signed an informed consent form.
Acknowledgments
We thank all nurses, physicians and documentation personnel of the outpatient clinics of the Department of Rheumatology and Immunology of the Hannover Medical School for collecting blood samples, informing the patients about the study and documenting patients’ medications.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GS conceived and planned the study. GS and NMP took the lead in writing the manuscript. FA, DE and TW significantly contributed to drafting and revision of the paper. NMP and CCP contributed substantially to data acquisition and interpretation. GS is responsible for the overall content of this work as a guarantor. GS and NMP performed the statistical analysis. All authors approved the final version.
Funding This project was funded by the Rosemarie-Germscheid foundation. It was additionally supported by the Deutsche Forschungsgemeinschaft (German Research Foundation) under Germany’s Excellence Strategy (EXC 2155 'RESIST', project ID 39087428) and the German network for multiorgan autoimmune diseases (GAIN_01GM1910E) and the German Center for Infection Research (DZIF TTU 01.801).
Competing interests None declared.
Patient and public involvement statement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.