Article Text

Abstract
Introduction Axial spondyloarthritis (axSpA) is a chronic inflammatory disease that typically affects people in their second and third decades of life, which are important years for establishing a professional career. We aim to study outcomes of work participation (WP) and their associations with demographic and clinical confounders, in addition to prevalence of negative workplace experiences in axSpA.
Methods In total, 770 patients with axSpA participated in the multicentre, observational ATTENTUS–axSpA survey in Germany. Demographic information, clinical parameters and patient-related outcomes (including disease activity and function) with a focus on WP were prospectively recorded.
Results A high prevalence of negative workplace experiences was reported among the 770 patients analysed. Overall, 23.4% of patients were not employed and 6.5% received disability pensions. Current work cessation was prevalent in 120 patients, and 28 of those were out of work for 10 years or longer. Of the 590 currently employed patients, 31.9% reported absenteeism and 35.9% reported presenteeism for >1 month within the past year. Multivariate logistic regression identified low disease activity (Bath Ankylosing Spondylitis Disease Activity Index), better physical function (Bath Ankylosing Spondylitis Functional Index) and better global functioning (Assessment of SpondylAarthritis International Society–Health Index) as the main predictors for unimpaired WP (n=242). Importantly, biological treatment, disease duration, age, sex, education level and body mass index were not reliable predictors.
Discussion Despite improvements in pharmacological treatment options, we still observed substantially impaired WP in patients with axSpA. These data emphasise the high unmet need for targeted strategies to provide improved medical and social care.
- Spondylitis, Ankylosing
- Immune System Diseases
- Patient Reported Outcome Measures
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The data sets generated during and/or analysed during the current study are not publicly available. Novartis is committed to sharing with qualified external researchers access to patient-level data and supporting clinical documents from eligible studies. These requests are reviewed and approved on the basis of scientific merit. All data provided are anonymised to respect the privacy of patients who have participated in the trial in line with applicable laws and regulations. The data may be requested by writing to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Axial spondyloarthritis (axSpA) can result in impairments in physical function and all aspects of health-related quality of life.
Even though an improvement in work productivity after biological treatment has been shown, impairments still persist.
WHAT THIS STUDY ADDS
This study showed that a number of patients reported impaired work participation (WP) with a high frequency and long duration of withdrawal from work, sick leave, presenteeism and also a high prevalence of negative workplace experiences.
Patients with unimpaired WP showed lower disease activity, better physical function and better global functioning.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These data emphasise the unmet medical needs and thereby the necessity for targeted strategies for improving medical and social care for patients with axSpA.
Introduction
Axial spondyloarthritis (axSpA) is a chronic inflammatory disease that predominantly affects the axial skeleton, which can result in structural damage and permanent disability.1 In addition, disease flares can cause intermittent periods of functional incapability. Impairments in physical function and all aspects of health-related quality of life (HR-QoL) have been described,2 but better treatment options within the last decade have raised hope of improved treatment outcomes.3
AxSpA most frequently affects people in their second and third decades of life, which tend to be important years for establishing a professional career.4 5 The importance of work participation (WP) has been recently highlighted,6 and the European Alliance of Associations for Rheumatology (EULAR) taskforce has recently published points to consider for studies with WP as an outcome domain.7 Impairments in WP can be measured across different domains6 8–10 including disability pensions, unemployment, sick leave, absenteeism and presenteeism.
Even though an improvement in work productivity after biological treatment has been shown,11 impairments still persist.11 12 Previous studies specifically focusing on WP have limited their analysis to WP’s relation to typical clinical and demographic factors.10 13 14 Other studies15 have included patients with self-reported axSpA without a confirmed diagnosis. Other dimensions of WP, such as differences in treatment, workplace experiences and vocational rehabilitation have been investigated infrequently.16 Although most studies have been conducted in Europe,8 9 11 13–15 17 data on the different WP outcomes in the German axSpA population are scarce. Participation in the workforce and sick leave, and their impact on indirect health costs have been frequently analysed18; the impact of decreased work productivity and negative workplace experiences have been studied less intensively in patients with axSpA.
The aim of the current work is to characterise different outcomes of WP in patients with axSpA and their associations with demographic and clinical confounders. In addition, we explored the prevalence of negative workplace experiences in our cohort.
Methods
Study design, survey and procedure
The ATTENTUS–axSpA survey is a multicentre, observational, cross-sectional study conducted across Germany from November 2019 to July 2020. A total of 14 study centres participated in the project, which comprised hospitals with a rheumatological department, rehabilitation clinics and outpatient clinics. Recruited patients were asked to participate in the survey during a routine visit to their healthcare practitioner.
Inclusion criteria were a clinical diagnosis of axSpA, as defined by the International Classification of Diseases (ICD), 10th Revision, Code M45, confirmed by the treating rheumatologist. To increase data quality, clinical research associates monitored study sites to supervise inclusion/exclusion criteria, in particular to ensure that the included patients fulfilled the Assessment in SpondyloArthritis International Society 200919 and/or the modified New York diagnosis criteria20 (online supplemental table 1).
Supplemental material
Eligibility criteria were checked, and informed consent was obtained by a rheumatologist at each study site. Patient advocates (LH) were involved in the design of the study, development of outcomes, data interpretation, writing of the manuscript and dissemination of study results.
The survey consisted of 113 overarching questions (among them 40 self-generated questions) and included demographic information, questions related to WP including axSpA’s impact on work, and clinical information (relating to diagnosis, symptoms and treatment). The patients completed validated questionnaires such as the Work Productivity and Activity Impairment Questionnaire (WPAI)–axSpA,21 22 Bath Ankylosing Spondylitis Disease Activity Index (BASDAI),23 Bath Ankylosing Spondylitis Functional Index (BASFI),24 Assessment of SpondyloArthritis International Society–Health Index (ASAS-HI) including environmental factors25 and Health Assessment Questionnaire Disability Index (HAQ-DI).26 The survey was developed by medical experts and patient research partners represented by the German patient organisation for axSpA (Deutsche Vereinigung Morbus Bechterew e.V.), in order to generate data based on patient relevant questions that are not currently a part of validated questionnaires. There was no formal validation of the self-generated questionnaire.
This study was conducted in compliance with the ethical principles originating in or derived from the Declaration of Helsinki and all International Conference on Harmonisation Good Clinical Practice guidelines. All patients (or their representatives) signed an informed consent form, and the research protocol was reviewed and approved by an independent ethics committee or institutional review board. The Ethics Committee of the Hannover Medical School (EK MHH) approved this study.
Patients completed the questionnaire digitally on a tablet (HUAWEI MediaPad T5). The survey was conducted by Mondosano GmbH on behalf of Novartis Pharma GmbH and completed on a website managed externally by Mondosano GmbH.
A list of the study investigator at each participating site is provided in online supplemental table 1.
Sample selection
Presenteeism has been shown to anticipate future absenteeism; because of this, question 5 (presenteeism) of the WPAI-axSPA was used to calculate the sample size.11 Based on work from Shim et al,11 an SD of 20% was assumed. With a drop-out estimate of 10%, a sample size of 500 participants would allow a precision (radius of the 95% CI) of approximately 2%, and with 1000 participants, the precision would be approximately 1%. Moreover, the sample size was verified to generate valid data which can be generalised to the German axSpA population. The drop-out rate of 10% has been justified by experiences made in former questionnaires.
Data analysis
Survey interpretation and scoring
WP outcomes were assessed by direct questions. Short-term absenteeism (percentage of work time missed due to axSpA) and presenteeism (percentage of impairment while working due to axSpA) within the last week were calculated from the WPAI-axSpA following standard procedures.21 Additionally, we examined long-term absenteeism as the overall number of sick leaves within the last 12 months and long-term presenteeism was defined as the number health problems affected productivity while working within the last 12 months. All evaluated standardised questionnaires (ASAS-HI, BASDAI, BASFI and HAQ-DI) were assessed according to standard guidelines; detailed information can be found in the respective publications.27–29
Statistical analysis
All analyses were conducted using SPSS V.27. We used a standard significance criterion of α=0.05 for all analyses. For statistical analysis, the χ² test, Student t-test and non-parametric Mann-Whitney U test were performed as appropriate. We analysed a ‘full study population’ sample and, for a more detailed analysis of work outcomes, a ‘WP study population’ sample. The latter group was derived by excluding old age retirees and students to define a cohort of participants who should have full access to WP, that is, participants who are eligible to work. For describing the characteristics of the full study population and the WP study population, we determined absolute and relative frequencies (reported in percentages). For non-categorical variables, we reported the arithmetic mean and SD. To determine the impact of age on workplace experience, the WP was divided into two age cohorts based on the mean age of 47 years in the full set population. Particular focus was on general characteristics and work characteristics, including duration of work cessation, short-term and long-term absenteeism, presenteeism in relation to workplace experiences and the impact of disease activity and function on WP. Further, we examined descriptively whether there was a correlation between presenteeism and absenteeism, and presenteeism and impairment of daily activities. Because work impairment is a time-dependent process, we performed similar analyses in two age groups separated by the mean age of the WP study population. We used binary logistic regression to determine the main predictors for work impairment. Model assumptions were verified by testing for the absence of multicollinearity between the independent variables using the Pearson correlation matrix, variance inflation factors (VIFs) and condition indexes (CIs); a VIF of >10 and a CI of >100 suggest multicollinearity. We used WP (impaired vs unimpaired) as Bernoulli distributed target variable where impaired WP=0 and unimpaired WP=1. We computed univariate logit models independently for explanatory variables of particular interest (see table 1 for the variables). The maximum likelihood method was used to estimate regression coefficients. To decide whether to include a variable in multivariate regression, we evaluated the variables with regard to model significance and quality. Model quality of the fitted models was assessed by the −2 log likelihood value indicating deviance, the Cox and Snell pseudo R² (R2 CS), Nagelkerke pseudo R² (R2 N), and classification matrices indicating prediction quality. Variables that achieved significance in their univariate logit models and good model quality were included in the multivariate logit model. The multivariate model was assessed by these same criteria. For interval estimation, we used CIs and ORs exp(ßj). Additionally, we conducted a post hoc Games-Howell test to compare patient-reported outcomes (PROs) by different types of WP impairment (unimpaired WP, short-term presenteeism, short-term absenteeism, no employment and disability pension).
Univariate and multivariate logistic regression with WP as target variable (unimpaired WP=1, n=695)
Results
General characterisation of the full study population
A total of 770 participants completed that survey, which is defined as the full study population; the general characteristics of this cohort are outlined in table 2; further details can be found in online supplemental table 2.
Demographic, clinical, PRO and WPAI–axSpA characteristics of the full study population and the ≤47 and >47 years age subgroups
Over half of the patients (54.2%, n=417) had been diagnosed with axSpA more than 10 years prior to the study, with the most common diagnosis being ankylosing spondylitis (75.1%, n=578). The most commonly reported disease symptom was back pain (87.5%, n=674). Level of health status and physical function were mixed across patients, as indicated by mid-range means and SD in the PROs (table 2). Patients ≥47 years of age had a longer disease duration and higher impairments in physical function compared with patients <47 years of age (table 2). Furthermore, patients ≥47 years of age had a higher proportion of women and a higher body mass index (BMI), and a lower proportion had a university degree.
WP characterisation
We next explored the basic domains of WP. Figure 1A,B describe the work status of the full study population (n=770): 76.6% (n=590) of patients reported paid work (part-time: 17.1%, n=132; full-time: 59.5%, n=458); 23.4% (n=180) of patients were not employed. Specifically, 6.5% (n=50) received disability pensions (n=32 due to axSpA), and 3.8% (n=29) received unemployment benefits (n=14 due to axSpA). The prevalence of disability pensions increased with age, with a prevalence of 12.5% in the age group between 50 years and 59 years (figure 1C). A similar observation could be made for non-participation in the workforce, which was highest (19.0%) in the age group 50–59 years (figure 1C). Interestingly, we did not observe an increase with disease duration (online supplemental file 1).
Supplemental material

Work status and basic domains of WP in the study populations. (A) Definition of the study populations, (B) work status of the WP study population, (C) frequency of disability pensions and participation in the workforce for different age groups in the full study population and (D) frequency of absenteeism and presenteeism for different age groups in the WP study population. *Defined as <3 months’ sick leave within the past year. WP, work participation; WPAI, Work Productivity and Activity Impairment Questionnaire.
The WP study population consisted of 695 patients because old age retirees (n=68) and students (n=7) were excluded from the full study population. The mean age±SD of the WP study population (n=695) was 45.3±10.9 years, with 60.9% (n=423) of patients being male (n=423). Next, we calculated the frequency of patients with unimpaired WP, that is, patients who were currently employed, with no current presenteeism (≤20% by WPAI–axSpA), no current absenteeism (by WPAI-axSpA) and lack of prolonged sick leave within the last year (figure 1A). There was a larger proportion of patients who had impaired WP (65.2%, n=453) than unimpaired WP (34.8%, n=242). Importantly, 348 patients (50.1%) with impaired WP were nevertheless part of the workforce. A continuous increase in age did not impact (or was not associated with increased) absenteeism and presenteeism in the WP study population (figure 1D), contrary to what was observed for unemployment status and disability pensions (figure 1C,D), and no increase with disease duration was observed (online supplemental file 1). The WP study population of >47 years of age suffered from higher total impairment and a higher proportion were stated to be unemployed compared with the study cohort of ≤47 years of age.
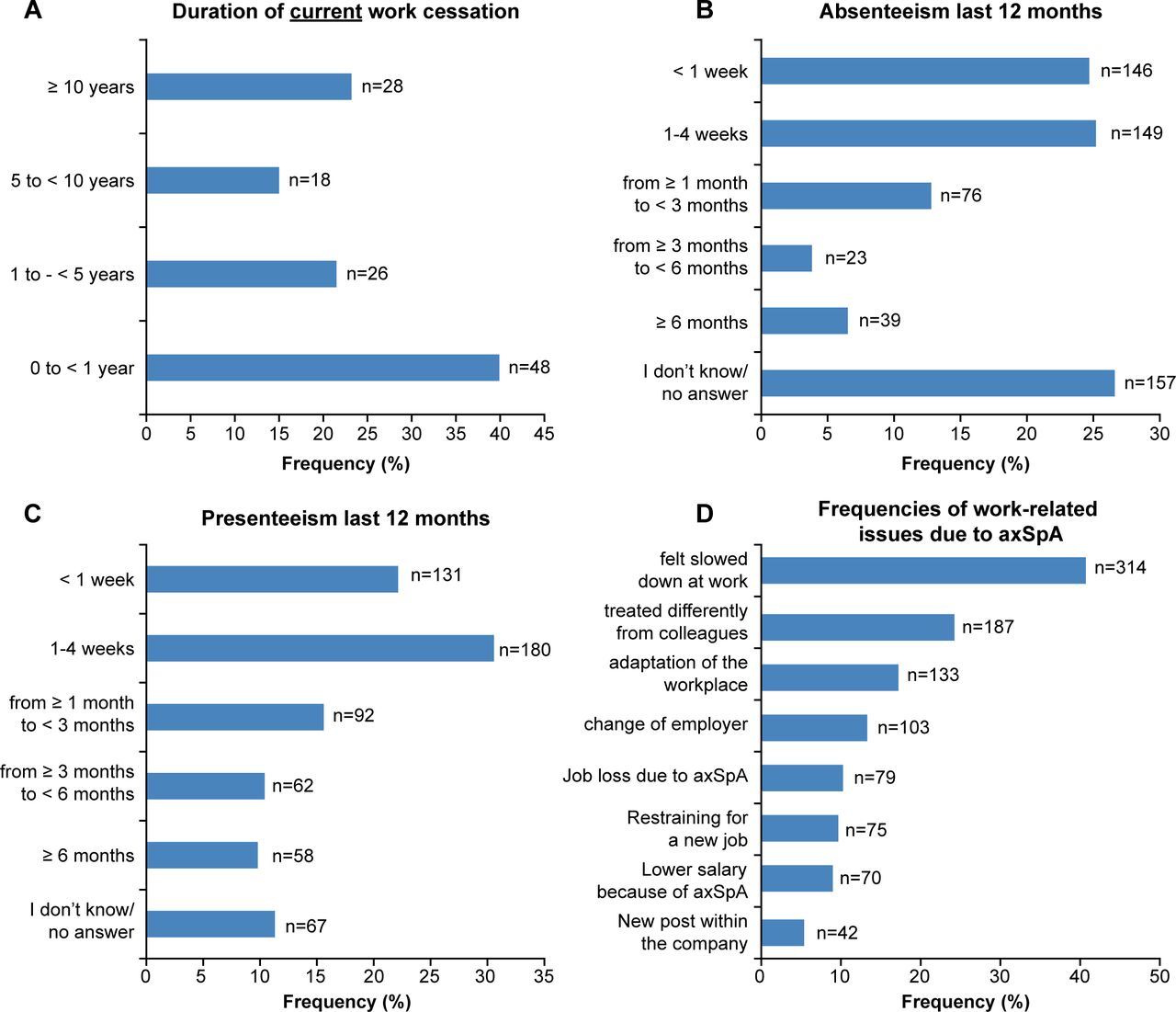
Duration of work cessation
Next, we investigated the duration of continuous work cessation. In the WP study population, 120 patients (15.6%) indicated an inability to work due to their axSpA disease (and for no other reasons). The mean duration of work cessation in these patients was 5.6 years. Importantly, only 48 of these patients (40.0%) were unable to work for a short duration of less than 1 year, but 72 (60.0%) were out of work for longer than a year, and 28 patients (23.3%) reported being unable to work for 10 years or longer (figure 2A). This indicates that long-term work cessation is a major problem in patients currently unable to work due to their axSpA. The mean durations of receiving disability pensions and unemployment benefits due to axSpA ranged between 7 years and 12 years. In summary, these data indicate that patients with axSpA who have ceased to participate in the work force frequently do so for continuous periods of time.

Long-term work impairments and negative workplace experiences. (A) Duration of current work disability in the WP study population, (B) duration of absenteeism within the past year (long-term absenteeism) among workers in the WP study population, (C) duration of presenteeism within the past year (long-term presenteeism) among workers in the WP study population and (D) frequencies of work-related issues due to axSpA among the WP study population. axSpA, axial spondyloarthritis; WP, work participation.
Short-term and long-term absenteeism
As axSpA is defined by intermittent disease flares in many patients, we were interested in understanding the relationship between short-term and long-term absenteeism. For long-term absenteeism, we analysed the overall number of sick leaves within the last 12 months. In our cohort, 433 patients reported at least some absenteeism in the past year. Of those, 146 patients (33.7%) reported absenteeism of less than 1 week and 149 patients (34.4%) between 1 week and 4 weeks within the past year. In addition, 138 patients (31.9%) reported absenteeism for ≥1 month within the past year (figure 2B). Consistently, in the WPAI-axSpA questionnaire, which focuses on the past 7 days, 450 patients (76.3%) reported not having lost any working hours in the past week and absenteeism within the past week occurred in 23.7% (n=140) of employed patients (online supplemental figure 2). These data indicate that absenteeism in the last 7 days does not give the full picture on work impairment as compared with data on longer time periods.
Supplemental material
Presenteeism and workplace experience
Patients were also asked how often they went to work despite not feeling healthy enough to work within the past year. Here, a large proportion of patients also reported extended periods of presenteeism (ie, long-term presenteeism) (figure 2C) with 35.9% (n=212) of patients reporting presenteeism for >1 month. Importantly, while there was no clear relationship between absenteeism and presenteeism, results indicated a positive correlation between presenteeism and impairment of daily activities in the WP study population (online supplemental figure 3A,B).
Supplemental material
We further explored whether negative workplace experiences due to axSpA played a relevant role in the full study population (figure 2D). We found that 40.8% (n=314) of patients reported, based on their personal assessment, disease limitations hindering their professional growth compared with their healthy counterparts. Other common work-related issues were paid sick leave, being treated differently from colleagues at work because of their disease and requiring adaptions in the workplace. Furthermore, 50.9% (n=392) of patients reported having adapted their living and working environment to their needs. Importantly, 33.4% of patients (n=257) reported factors that would contribute to volatility to the workforce such as change of employer (n=103), job loss due to axSpA (n=79) or retraining for a new job (n=75) during their professional career (figure 2D). In summary, decreased work productivity and negative workplace experiences were frequently reported by these patients with axSpA.
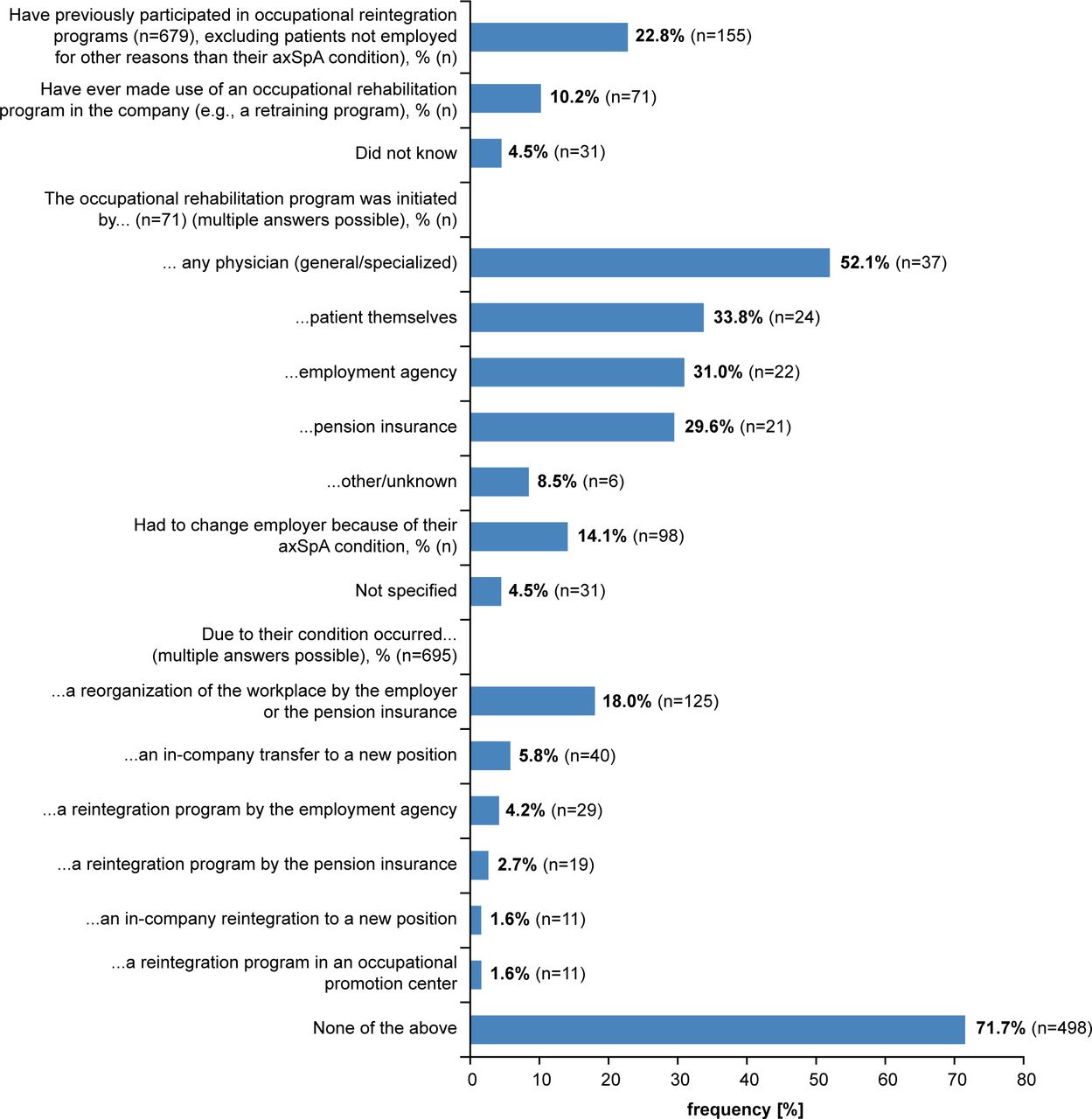
Vocational reintegration and rehabilitation programmes
In the WP study population, 22.8% (n=155) of patients had previously participated in vocational reintegration programmes and 10.2% (n=71) had previously taken part in rehabilitation programmes (figure 3). The mean time since last taking part in a vocational rehabilitation was 8.1 years. Further details regarding the impact of axSpA on work, as well as reintegration and rehabilitation programmes, can be found in online supplemental table 5.
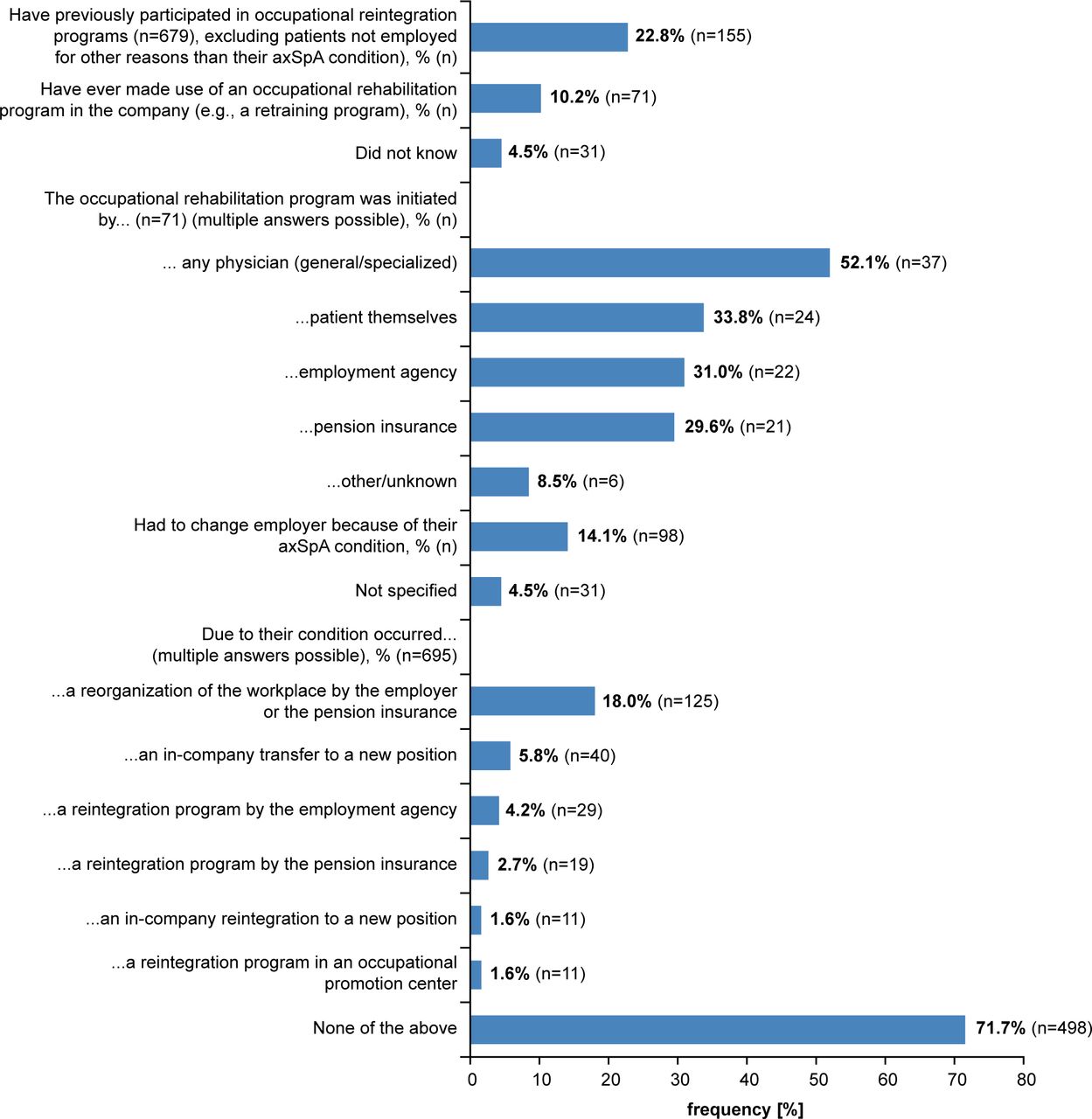
Vocational reintegration and rehabilitation programmes in the work participation study population. axSpA, axial spondyloarthritis.
Association between WP and demographic and clinical confounders
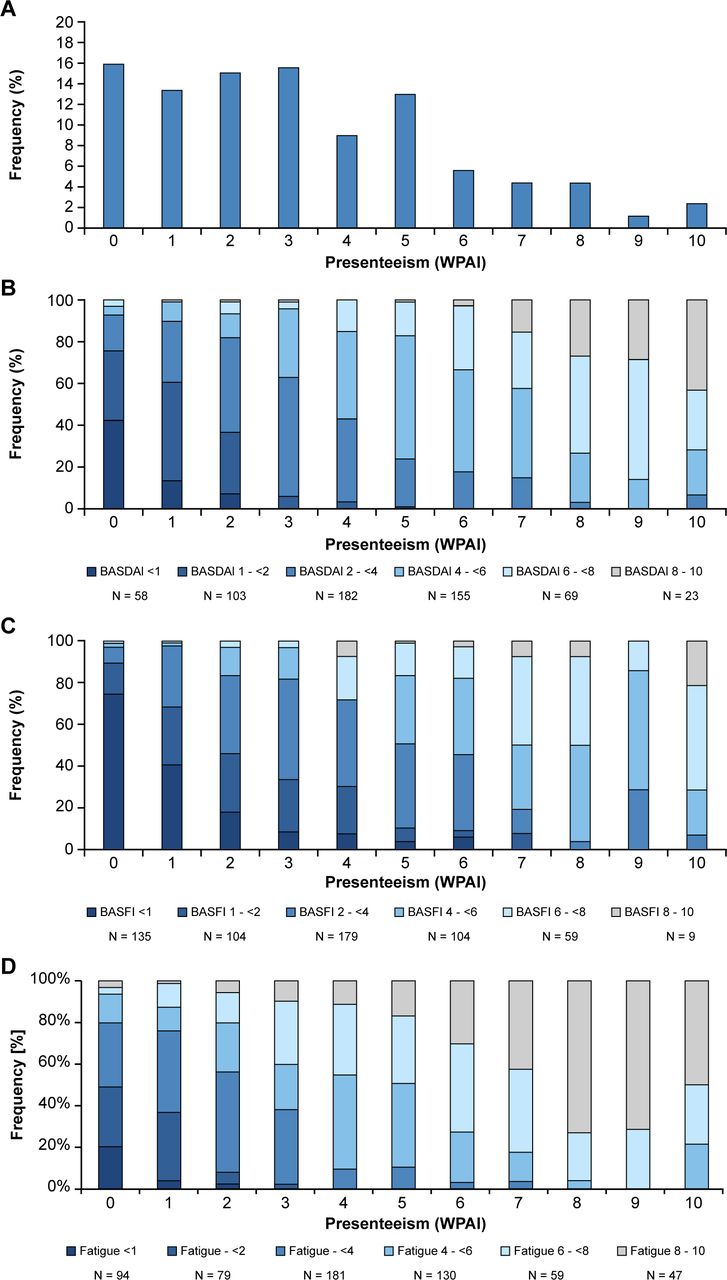
Relationship between presenteeism and disease activity and function:
Having described the different components of impaired WP, we aimed to better understand the relationship between short-term presenteeism and disease activity as well as function in the WP study population. We thus analysed the BASDAI and BASFI outcome measures in our patients with different degrees of presenteeism, according to the WPAI–axSpA. Only 15.9% (n=94) of patients reported a presenteeism score of 0 within the last 7 days, and we observed a broad distribution of the presenteeism values within our cohort (figure 4A). In addition, there was a clear increase in disease activity (figure 4B) impairments in functional capacities (figure 4C) and fatigue (figure 4D) with increasing presenteeism scores.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intensity of short-term presenteeism and its association with disease activity (BASDAI) and function (BASFI) in the WP study population. (A) Distribution of presenteeism, (B) presenteeism and BASDAI score, (C) presenteeism and BASFI score, (D) presenteeism and WPAI score. BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; WP, work participation; WPAI, Work Productivity and Activity Impairment Questionnaire.
Impact of disease activity and function on WP: To compare patients with different degrees of WP in logistic regression, we split the WP Study Population into patients with impaired WP and patients with unimpaired WP, as mentioned above (figure 1). Model assumptions of the independence of the explanatory variables were verified; the explanatory variables did not show a high correlation with each other (all VIFs<10 and all Cis<100; see further details and values of the correlation matrix in the online supplemental table 6). While univariate models with age, gender, education, employment, disease duration, and biological treatment as explanatory variables were statistically significant according to Chi-squared tests, only ASAS-HI, BASDAI, BASDAI≥4, BASDAI fatigue, BASDAI duration morning stiffness, and BASFI additionally showed good model quality (see table 1 and online supplemental table 5). Accordingly, only these latter PRO variables were carried forward to multivariate regression to assess which variables significantly predict WP. Given a good fit, high explanatory power, and high prediction quality (table 1), we accepted the model. The Chi-squared test suggests the model was significantly better than one without the explanatory variables (χ2=350.81, p<0.001; −2 log likelihood (null model)=547.587 [846.486], R2 cs=0.40, R2 N=0.55) with an overall prediction of 82.7% (unimpaired WP: 70.7%; impaired WP: 89.2%). ASAS-HI, BASDAI, and BASFI significantly predicted WP. Patients with impaired WP tended to have worse global functioning (ASAS-HI), impaired physical function (BASFI) and higher disease activity (BASDAI). The ORs imply that the chances of having unimpaired WP decrease by a factor of 0.866, 0.576 and 0.816 if the ASAS-HI, BASDAI and BASFI scores, respectively, increase by one point (ie, if health, disease activity and functional capacity worsen). The analysed BASDAI subvariables (≥4; fatigue and duration of morning stiffness) did not significantly influence WP.
The post hoc Games-Howell test also confirmed that patients with unimpaired WP had significantly better global functioning, physical function and lower disease activity (including less fatigue and duration morning stiffness) than patients with different types of WP impairment (see online supplemental table 8 and online supplemental figure 4A–E).
Supplemental material
Discussion
The aim of the current work is to characterise different outcomes of WP in a population of patients with axSpA and to examine the prevalence of negative workplace experiences in this cohort. We investigated the short-term and long-term durations of work outcomes and included questions about different workplace experiences.
In terms of general characteristics, the axSpA population reported in the current study is comparable to the general population in Germany across various characteristics, such as average age (male: 46.7 vs 43.2, female: 47.8 vs 45.8), BMI (male: 28.1 vs 26.5, female: 27.6 vs 24.9) and education (27.0% vs 18.0% with a degree in higher education).30 A high proportion of the employed patients showed presenteeism and in addition, we observed a high degree of negative workplace experiences. These included not only factors that might contribute to a lesser income but also factors that might influence participation in the workforce and lead to a higher risk of being at least temporarily unemployed. Self-reported discrimination at the workplace was frequent and adaptations at the workplace were often required. Our data support the literature reporting the severe impact of axSpA on WP.8–10 13 15 31
Long-term unemployment due to axSpA was reported, and a large proportion of patients received disability pensions. Importantly, cessation of workforce participation was frequently a long-term problem. Of patients eligible to work, the majority reported impaired WP. Almost a fifth of employed patients showed short-term absenteeism and sick leave was common. However, we demonstrated that short-term absenteeism, as analysed using the WPAI–axSpA, did not necessarily reflect the overall burden of sick leave over a year in our cohort. Random weekly variations of absenteeism are not likely to confound the results given in a large study population. However, a crucial factor for assessing the WPAI is the existence of current employment. This might be a significant problem in a population with a high proportion of workers with negative workplace experiences (eg, due to chronic diseases) who frequently change jobs and who, although unemployed, still consider themselves as part of the workforce. These patients would be a priori excluded from the analysis of the WPAI, and this might be a potential bias which could also explain the discrepancy between long-term absenteeism and short-term absenteeism as analysed via WPAI-axSpA. As such, our data suggest the importance of considering the choice and influence of outcome measures of work impairment.
Even though grave WP impairments existed in our population, only a small proportion of patients had previously participated in vocational rehabilitation or reintegration programmes, suggesting the need for better access to these programmes in Germany. Multivariate regression identified worse global functioning (ASAS-HI), impaired physical function (BASFI) and higher disease activity (BASDAI) as the main predictors of impaired WP. Other studies have already identified a correlation between these PROs and treatment,11 17 32–34 suggesting that treatments which target alleviating symptoms related to physical function and disease activity will likely also improve WP. BASDAI subvariables only reached significance in the univariate models, suggesting they were not able to explain any variance beyond the other predictors. Both short-term presenteeism and absenteeism are associated with PROs including higher disease activity and limitations in physical function.14 35 36 Interestingly, some patients with a low or very low BASDAI score reported at least some degree of presenteeism and a similar observation could be made for BASFI function. However, an increase in BASDAI activity resulted in higher impairments of work productivity compared with BASFI function. This descriptive examination of the data suggested an association between BASDAI and BASFI scores and short-term presenteeism in our cohort. Moreover, an increase in fatigue (BASDAI #1) suggests an association between fatigue and short-term presenteeism as well.
We found no differences in terms of disease duration; as WP is already substantially reduced in patients with early axSpA,17 effective fast-acting therapies are needed. Strikingly, biological treatment did not significantly improve WP. This supports some previous findings36 and highlights that the medical need remains high and requires urgent attention. Although other studies suggest biological treatment can lead to improvements in work disability and disease symptoms,36–39 substantial unmet needs remain.11 12 It may be that biological treatment improves outcomes for some domains of impairment but not all; for instance, Wallman and colleagues only found improved work disability after treatment, while disability pension levels remained similar.12 In addition to biological treatment, rehabilitation and reintegration programmes are likely to be required as they have a positive effect on quality of life in terms of physical function and pain.40–42 Additional effects can be achieved if rehabilitation is added with behavioural therapy, although it is unclear which effect is achieved by behavioural training and rehabilitation alone.43 Further, EULAR recommendations also cover a range of lifestyle behaviours, including exercise and diet recommendations, that are likely to complement treatment plans.44 Specialised rheumatological rehabilitation programmes use a multidisciplinary team approach to address the different individual needs of patients, including education and provision of self-management strategies which are addressed by recommendations.45–48 Rehabilitation programmes are an effective way to provide patients with axSpA the access to healthcare professionals, which may improve participation.47 49
Some studies show that various demographic variables such as age, sex and education are also associated with WP,6 9 35 50 although not consistently.36 While these variables were significant WP predictors in univariate analyses, we did not analyse them further due to poor model quality, and such results need to be interpreted cautiously.
The ATTENTUS–axSpA study was designed to collect data for a large population size and a multitude of measures allowing for a thorough overview of the axSpA population in Germany. The study included a variety of demographic, clinical and HR-QoL confounders, as well as vocational rehabilitation programmes and other work-related information about the impact of axSpA on work typically neglected in clinical settings and other studies (eg, adaptions at work, differences in treatment and workplace changes). These factors are important as WP is related not only to disease but also to other variables such as the social environment.51 52 Furthermore, the population was identified via diagnosis through rheumatologists at study sites and additional external monitoring was performed, making the results more reliable and specific to the axSpA population compared with other studies, such as the European map of axial spondyloarthritis (EMAS) survey15 which included patients with self-reported axSpA.
The comprehensiveness of the questions in this study offers a rich characterisation of the axSpA population that may guide future research and provide a framework for asking questions in a clinical setting, as well as direct workplace strategies to provide appropriate support. For instance, further distinction between patients according to their dominant domain of work impairment may provide insight if patients with distinct impairments also differ in other characteristics.
Impaired WP is not just limited to work life but can also create additional social and psychological burdens as well as indirect costs from an economic point of view (eg, sick leave and time loss). Despite multiple medical therapy options for axSpA and evidence for the effectiveness of biological treatment in improving outcomes, we observed substantially impaired WP in patients with axSpA. Current treatment recommendations emphasise the importance of considering patient characteristics, including sociodemographic factors, in therapy plans.53 54 This requires a thorough characterisation of the patient population and the complex relationships across different health domains. The current study stresses the need for adopting a broader view to fully understand the relevance of the different domains of work impairment and their impact on patients with axSpA.
AxSpA most frequently affects people in their second and third decades of life, which tend to be important years for establishing a professional career.4 5 The average age of patients in the current study was around 47 years of age, which is similar to cohorts published earlier.5 Although patients ≤47 years of age had a longer disease duration, the impairments in work productivity were similar to those in patients ≤47 and >47 years of age. Patients >47 years of age were more likely to be unemployed (35.2%) compared with patients ≤47 years of age (11.5%). Nevertheless, presenteeism and absenteeism differed in both groups, resulting in a higher total impairment score in the >47 cohort compared with patients ≤47. Perhaps future studies should aim to access the effect of AxSpA on a younger cohort.
However, there are several limitations to this study. The cross-sectional design does not allow for conclusions about temporal causality. The survey did not question the time course but recorded the patient’s condition at the time of survey completion only. Accordingly, we cannot draw conclusions about differences in WP that could occur over time. Further, we did not capture work capacity prior to disease onset. However, such data would be prone to errors in memory, whereas presenteeism and absenteeism questionnaires such as the WPAI, assessing the time frame of 1 week, have a reduced risk of incorrect recollection.51 In this study, we also asked about absenteeism in the last 12 months and the duration of the current work cessation. It must be emphasised that questioning about longer periods of times may increase the risk of recall bias.
Another limitation is that the self-reported WP and data on disease activity and physical function rely on PROs rather than objective measures such as the Ankylosing Spondylitis Disease Activity Score55 or the Bath Ankylosing Spondylitis Metrology Index.56 Self-generated questions of the survey were not validated by external experts other than the authors of this work and psychometricians. In addition, we were not able to assess the Ankylosing Spondylitis Disease Activity Score (ASDAS) level because we did not collect data for C reactive protein in this study. As no data about the frequency of consultation with the rheumatologist were collected, it was not possible to analyse the effect of tight control treatment on the working participation; therefore, we cannot determine if the WP results were influenced by the combination of short disease duration and tight control treatment.
As this study focused exclusively on the German population, it is difficult to draw conclusions about other populations as countries differ by various patient characteristics, such as the proportion of manual versus non-manual occupations, comorbidities and differences in employment, and health systems. Nevertheless, similar results have been found in various European countries,13 as well as in Asia,36 suggesting patients across different geographical locations face similar difficulties. Further, we did not distinguish the type of employment; however, given the physical restrictions of the disease, manual workers tend to be more affected.8 9
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The data sets generated during and/or analysed during the current study are not publicly available. Novartis is committed to sharing with qualified external researchers access to patient-level data and supporting clinical documents from eligible studies. These requests are reviewed and approved on the basis of scientific merit. All data provided are anonymised to respect the privacy of patients who have participated in the trial in line with applicable laws and regulations. The data may be requested by writing to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was conducted in compliance with the ethical principles originating in or derived from the Declaration of Helsinki and all International Conference on Harmonisation Good Clinical Practice guidelines. All patients (or their representatives) signed an informed consent form, and the research protocol was reviewed and approved by an independent ethics committee or institutional review board. The ethics committee of the Hannover Medical School approved this study. Eligibility criteria were checked and informed consent was obtained by a rheumatologist at each study site.
Acknowledgments
Medical writing support was provided by Tatjana Lux (co.medical, Berlin, Germany) and Dr Alexander Boreham (co.medical, Berlin, Germany). The authors also thank Ellen McKenna for providing medical writing support and assistance, which was funded by Novartis Pharmaceuticals Corporation in accordance with Good Publication Practice (GPP3) guidelines (http://www.ismpp.org/gpp3).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators NA.
Contributors All named authors meet the International Committee of Medical Journal Editors criteria for authorship for this article, take responsibility for the integrity of the work as a whole and have given their approval for this version to be published.Study concept and design: UK, DMO, SL. Acquisition of data: all authors Analysis and interpretation of data: All authors, Writing of the manuscript: all authors, Critical revision of the manuscript for important intellectual content: All authors, All authors had access to the data, commented on the report drafts, and approved the final submitted version.
Competing interests The study was sponsored by Novartis Pharma GmbH, Germany. UK received consultancy and speaker honoraria from AbbVie, Biocad, Chugai, Eli Lilly, Grünenthal, Janssen, MSD, Novartis, Pfizer, Roche and UCB; and grant/research support (unrestricted grant) from Abbvie, Amgen, Biogen, Fresenius, GSK, Novartis and Pfizer. DM-O received consultancy and speaker honoraria from Abbvie, Amgen, Berlin Chemie, Bristol Myers Squibb, Cellgene, Chugai, Fresenius Kabi, GSK, Jansen Cilag, Lilly, Medac, Merck Sharp & Dome, Mylan, Novartis, Pfizer, Sandoz Hexal, Sanofi and UCB. KH received consultancy and speaker honoraria from Abbvie, Chugai, Gilead, Lilly, Novartis, Sandoz Hexal and Sanofi. LH has no disclosures. SL and AH are employees of Novartis.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.