Article Text

Abstract
Background The close relationship between joints and gut inflammation has long been known and several data suggest that dysbiosis could link spondyloarthritis (SpA) to inflammatory bowel diseases (IBD). The introduction of biological drugs, in particular tumour necrosis factor inhibitors (TNFi), revolutionised the management of both these diseases. While the impact of conventional drugs on gut microbiota is well known, poor data are available about TNFi.
Aim To investigate the impact of TNFi on gut microbiota.
Methods We evaluated 20 patients affected by enteropathic arthritis, naïve for biological drugs, treated with TNFi at baseline and after 6 months of therapy. All patients followed a Mediterranean diet. Patients performed self-sampling of a faecal sample at baseline and after 6 months of therapy. NGS-based ITS and 16S rRNA gene sequencing was performed, followed by the taxonomic bioinformatics analysis.
Results After 6 months of therapy, we detected a remarkable increase in Lachnospiraceae family (Δ +10.3, p=0.04) and Coprococcus genus (Δ +2.8, p=0.003). We also noted a decreasing trend in Proteobacteria (Δ −8.0, p=0.095) and Gammaproteobacteria (Δ −9, p=0.093) and an increasing trend in Clostridia (Δ +8.2, p=0.083). We did not find differences between TNFi responders (SpA improvement or IBD remission achieved) and non-responders in terms of alpha and beta diversity.
Conclusions Our findings are consistent with the hypothesis that TNFi therapy tends to restore the intestinal eubiosis.
- spondyloarthritis
- tumour necrosis factor inhibitors
- arthritis
- autoimmune diseases
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The study dataset is available upon reasonable request and is archived by the corresponding author. The protocol deposited with the Ethics Committee is also available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
To date, the manipulation of the intestinal microbiota is considered pivotal for the cure or control of several pathologies, which are sustained and fuelled by dysbiosis.
Scarce data are currently available about dysbiosis and inflammatory arthritis.
The impact of microbiota on rheumatic diseases and the effect of tumour necrosis factor (TNF) treatment on microbiota is inadequately investigated and not still completely understood.
What does this study add?
To our knowledge, this is the first study that evaluates the impact of anti-TNFs on the microbiota in patients with enteropathic spondyloarthritis.
How might this impact on clinical practice or further developments?
Our study contributes to reinforce the hypothesis that the therapy with anti-TNF alpha can affect microbiota by restoring intestinal eubiosis.
Based on this, the microbiota could play a key role in future targeted therapies.
Introduction
Enteropathic arthritis is included in a cluster of inflammatory joint diseases,1 according to the European Spondyloarthropathy Study Group classification criteria.2 Patients with enteropathic spondyloarthritis (SpA) show clinical features of axial3 and peripheral4 SpA, associated with either Crohn’s disease (CD) or ulcerative colitis (UC). The exact pathogenetic mechanisms linking gut inflammation with joint inflammation are still unclear, although shared genes and environmental factors might be involved.5
The role of microbiota in host health is well established, mainly through the maintenance of the mucosal integrity and anti-inflammatory immune response6–8; therefore, it is not surprising that dysbiosis, defined as the loss of microbiome diversity and composition in an individual, can promote autoimmune diseases.
Pieces of evidence regarding dysbiosis and SpA have been published 9–19 and data would suggest a link between SpA and inflammatory bowel diseases (IBD).9 20 21
The introduction of biological drugs, in particular tumour necrosis factor inhibitors (TNFi), revolutionised the handling of enteropathic SpA.22–26 Infliximab and adalimumab are approved for the treatment of CD and UC, and the 2019 recommendations encourage the use of these two TNFi monoclonal antibodies in patients with seronegative SpA and coexisting IBD.27
While the impact of TNFi on restoring gut permeability is well known,28–30 unsatisfactory data are available on microbiota and TNFi. Data acquired on animals would suggest that TNFi can restore gut permeability and microbiota.31 Few studies about the impact on TNFi on microbiota in humans affected by IBD or SpA would indicate a role of TNFi in restoring eubyosis32–34; yet, data on enteropathic SpA are still not available.32 33
Our study aimed to investigate the impact of TNFi on gut microbiota as well as the association of microbiome characteristics with inflammatory parameters in a population of enteropathic arthritis patients, who were treated with either adalimumab or infliximab.
Materials and methods
Patients recruitment and study design
Twenty patients were recruited at the Rheumatologic-Gastroenterologic Diseases clinic in Città della Salute e della Scienza di Torino, Italy, from June 2017 to December 2018.
Inclusion criteria comprised: patients of age greater than 18 years old and capable of providing informed consent before study participation; patients on a typical Mediterranean diet; CD or UC diagnosis in patients fulfilling criteria for axial or peripheral SpA (ASAS 20093 35); patients able to perform the sample’s test after appropriate training as indicated in the BMR Genomics protocol; patients naïve to TNFi, and treated for arthritis, IBD or both, according to current guidelines for rheumatic disease36 and IBD37 38; stable concomitant treatment in the previous 3 months and for all the duration of the study.
Exclusion criteria were: history of major bowel resection; history of minor bowel resection or digestive stoma in the previous 5 years; any contra-indication to TNFi therapy; refusal to sign the informed consent; linguistic or cognitive difficulties that did not allow a full understanding of the consent form process; pregnancy or breastfeeding.
Clinical history, physical examination, instrumental examinations, biochemical examination including C reactive protein (CRP), erythrocyte sedimentation rate (ESR), HLA-B27 and faecal calprotectin at the baseline and after 6 months were performed.
All patients were screened for Hepatitis B Virus (HBV), Hepatitis C Virus (HCV) and Mycobacterium tuberculosis (HBsAg, HBcAb, HBsAb; HCV-Ab; quantiferon-TB gold assay, chest X-ray) before starting biologicals, as per normal clinical practice. Faecal samples were collected for every participant: the first within 24 hours before starting TNFi, while the second after 6 months of therapy. After the discussion at the interdisciplinary rheumatic/gastroenteric board, treatment decisions were made based on clinical requirements.
All participants filled out a food daily diary to verify the Mediterranean diet, the absence of food intolerance with the consequent bias due to food restrictions, and the intake of drugs different from standard therapy.
The design of the prospective study did not affect the treatment or other clinical actions. Patients were naïve to TNFi treatment or other biologicals. TNFi included infliximab and adalimumab.
The study was approved by the ethics committee and subjects provided prior written informed consent.
Samples collection, processing and analysis
Faecal samples were collected in 2 mL faeces collection tubes with screw caps, filled with DNA-stabilisation buffer provided by BMR Genomics, and stored at −80°C until further use. All patients were trained for faecal sample collection, to reduce as much as possible the sample contamination; all samples complied with quality control.
The processing performed through metagenomic NGS (next-generation sequencing or sequencing in parallel) by BMR Genomics laboratories included the amplification of the V3 and V4 regions of the 16S-gene using universal primers according to Takahashi et al 39 followed by sequencing on the Illumina MiSeq platform (San Diego, California, USA) in the Paired-End 2×300 bp format and the standard bioinformatic taxonomic analysis of the 16S NGS.
Patient assessment
All patients were scheduled for biological therapy and received the treatment at least until week 24. Clinical disease indices were evaluated at baseline and the end of the study using: (i) Visual Analogue Scale to measure pain and disease activity in all patients; (ii) Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) for axial involvement; (iii) Clinical Disease Activity Index (CDAI); (iv) Health Assessment Questionnaire-Disability Index (HAQ-DI) for peripheral involvement; (v) Harvey-Bradshaw Index for CD (HBI)40 or partial Mayo (pMAYO) score for UC. The BASDAI clinical response was defined as a BASDAI <4.41 The improvement in HAQ-DI was defined as a minimum clinically important difference of 0.22.42 Responders in the HBI for CD were defined by a decrease in the HBI score greater than or equal to 2 (or HBI ≤4 at 6 months), corticosteroid-free therapy. For patients with UC remission was defined as the reduction of the pMAYO43 by at least two points, or final score ≤1, in the absence of corticosteroids.
Statistical analysis
Continuous characteristics were presented as median and IQR or mean±SD. For proportions, absolute and relative frequencies were reported.
Mc-Nemar test was performed to analyse qualitative differences, while Wilcoxon test was applied to analyse mean differences (between paired samples).
Univariate regression models were implemented to test the microbiota differences between baseline and after 6 months (linear model for clinimetric variables and logistic model for IBD success or SpA improvement).
A p value <0.05 was considered to indicate statistical significance. The analysis was performed using R Statistical Software (Foundation for Statistical Computing, Vienna, Austria).44
Alpha diversity45 is a measure of the diversity of species within an ecosystem or sample; it is expressed by the number of species or Operational Taxonomic Units (OTU) observed in the sample, which is a measure of species richness and evenness in that sample. Alpha diversity was measured through the Simpson’s Diversity Index (equation 1) and Shannon-Wiener Diversity Index (equation 2) from the OTU occurrence matrix.46
The Simpson’s Diversity Index (D) was calculated using the following equation:
 (1)
(1)
in which n i is the total number of OTUs in a particular species, while N is the total number of OTUs in all species.
The Shannon-Wiener Diversity Index (H) was calculated using the following equation:
 (2)
(2)
in which p i is n i divided by N.
Beta diversity45 is a measure of the diversity of species between two or more ecosystems or samples; it is expressed as the total number of unique species among the samples which are under comparison. Beta diversity therefore provides the variability of observed taxa among samples. The beta diversity Index was calculated using the PAST software by inputting the OTU occurrence matrix.46 Principal Coordinates Analysis (PCoA) plots of Beta diversity were performed using the Bray-Curtis similarity index, with the transformation exponent equal to 2. To test the significance between groups, one-way analysis of similarity (ANOSIM) was carried out using Bray-Curtis distances, with the number of permutation set to 9999.
Results
Twenty patients met inclusion criteria and were accepted to participate in the study. Informed consent was obtained from study participants.
The overview of patient characteristics is summarised in table 1.
Demographic and biometrics characteristics
Surgery (ileocecal resection) had been performed in 9 (45%) patients before the last 5 years.
At the baseline 90% of patients received mesalazine, 60% of patients took systemic corticosteroids and 20% took an immunosuppressant (azathioprine). All patients followed a Mediterranean diet.
Clinical outcomes
After 6 months of therapy, no patient discontinued TNFi due to adverse events; 100% of patients achieved clinical IBD remission, while the success of the therapy (corticosteroids free) was only achieved in 65% of patients (13 out of 20). The improvement of rheumatic manifestations was reached in 70% of patients.
CRP decreased from a median value of 8.2 mg/L (4.8–20.8 mg/L) at T0 to a median value of 2.9 mg/L (1–4 mg/L) at T6 (p=0.001). Similarly, the ESR decreased from a median value of 21.5 mm/hour (10.8–34 mm/hour) at T0 to 11 mm/hour (7.8–21 mm/hour) at T6 (p=0.003). Calprotectin decreased from a median value of 207.5 µg/g (125.5–446.2 µg/g) at T0 to a median value of 81 µg/g (50–197.2 µg/g) at T6 (p=0.004).
As regards clinimetry, we noticed a BASDAI decrease from 5.2 (4.1–5.6) to 2.8 (2.5–4.3, p=0.013), CDAI decrease from 13 (10.5–16) to 7 (5.2–11, p=0.004) (see table 2).
Comparison of clinical variables between baseline and T6 (6 months)
Description of the microbiota composition and effect of TNFi on microbiota
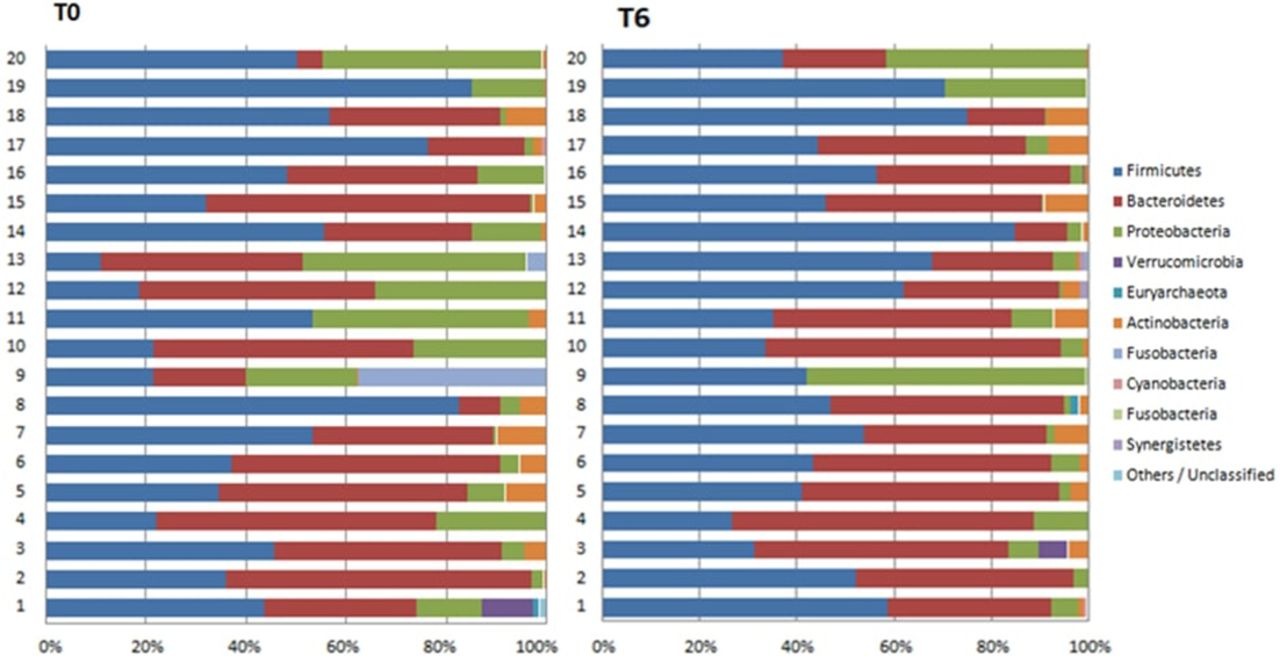
The faecal microbiota at baseline was characterised by a large proportion of Firmicutes (43.6% (29.5–53.8)) followed by Bacteroidetes (35.5% (19.1–50.3)), Proteobacteria (12.6% (3.4–23.3)), Actinobacteria (0.8% (0.1–4.5)) (see figure 1).

Distribution of phylum at the baseline (T0) and after 6 months (T6).
We compared the global composition of the faecal microbiota between T0 and T6. After 6 months of therapy, we observed noteworthy differences among the family of Lachnospiraceae (Δ +10.3, p=0.04) and the genus of Coprococcus (Δ +2.8, p=0.003), as shown in figure 2. We also observed an increase in the proportion of unclassified phyla (figure 1, Δ +10.3, p=0.015).
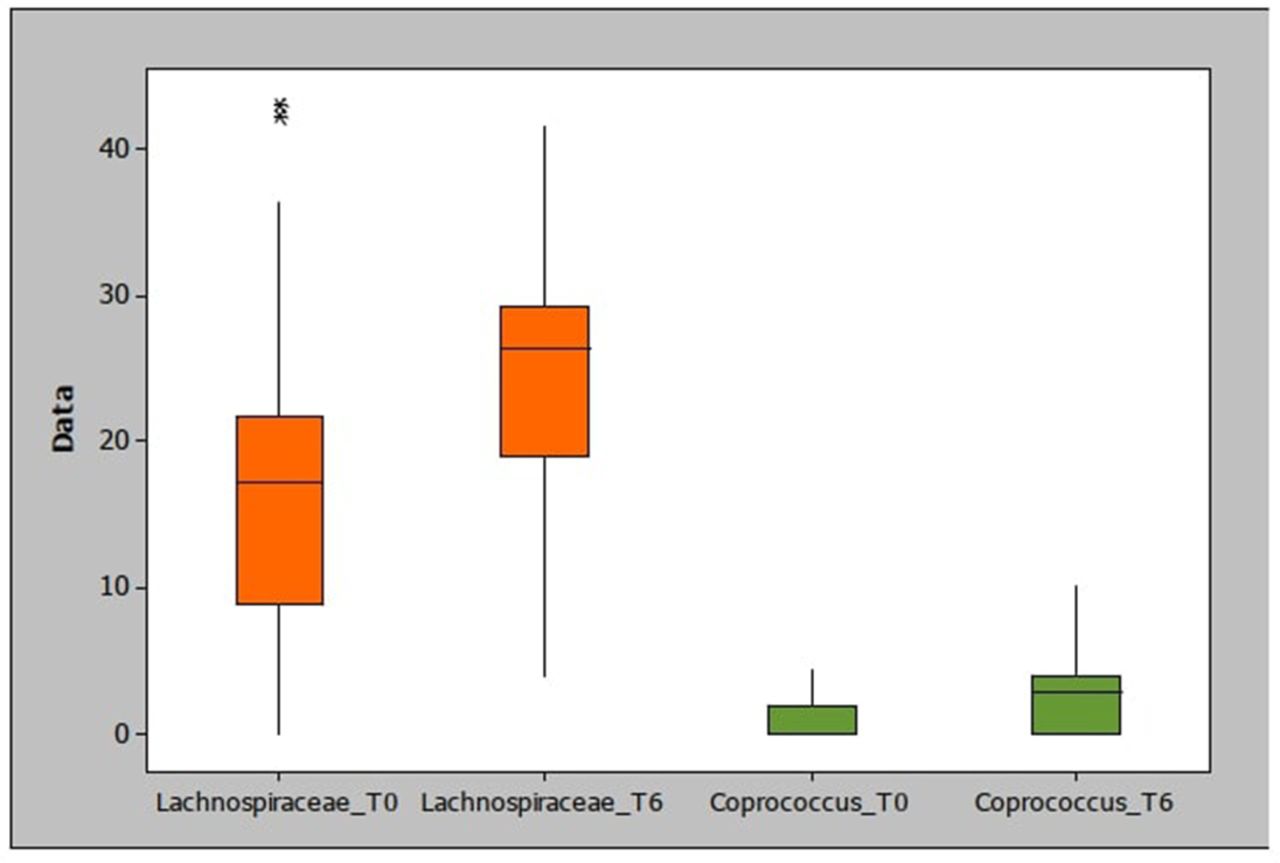
Comparison between Lachnospiraceae and Coprococcus at the baseline (T0) and after 6 months (T6) of therapy.
Despite the absence of statistically significant differences, we observed a trend in Proteobacteria (Δ −9.0, p=0.087), Clostridia (Δ +8.2, p=0.083) and Gammaproteobacteria (Δ −9, p=0.093), Lachnospiraceae (Δ +9.4, p=0.044) and Dorea (Δ +1.2, p=0.059).
The univariate analysis for the comparison of relevant microbiota variables (outcome) between clinimetric variables (covariates) and the delta (T6-T0) exhibited a significant result only for CRP (p=0.033) (table 3).
Univariate analysis to evaluate the association between clinimetric variables (covariates) and the delta (T6-T0) of relevant microbiota variables (outcome)
The univariate analysis for the comparison between clinimetric variables (covariates) and the delta (T6-T0) of relevant microbiota variables (covariates) and the IBD success/SpA improvement outcome did not show any significant correlation (table 4).
Univariate analysis to evaluate the association between the delta (T6-T0) of relevant microbiota variables (covariates) and the IBD success/SpA improvement (outcome)
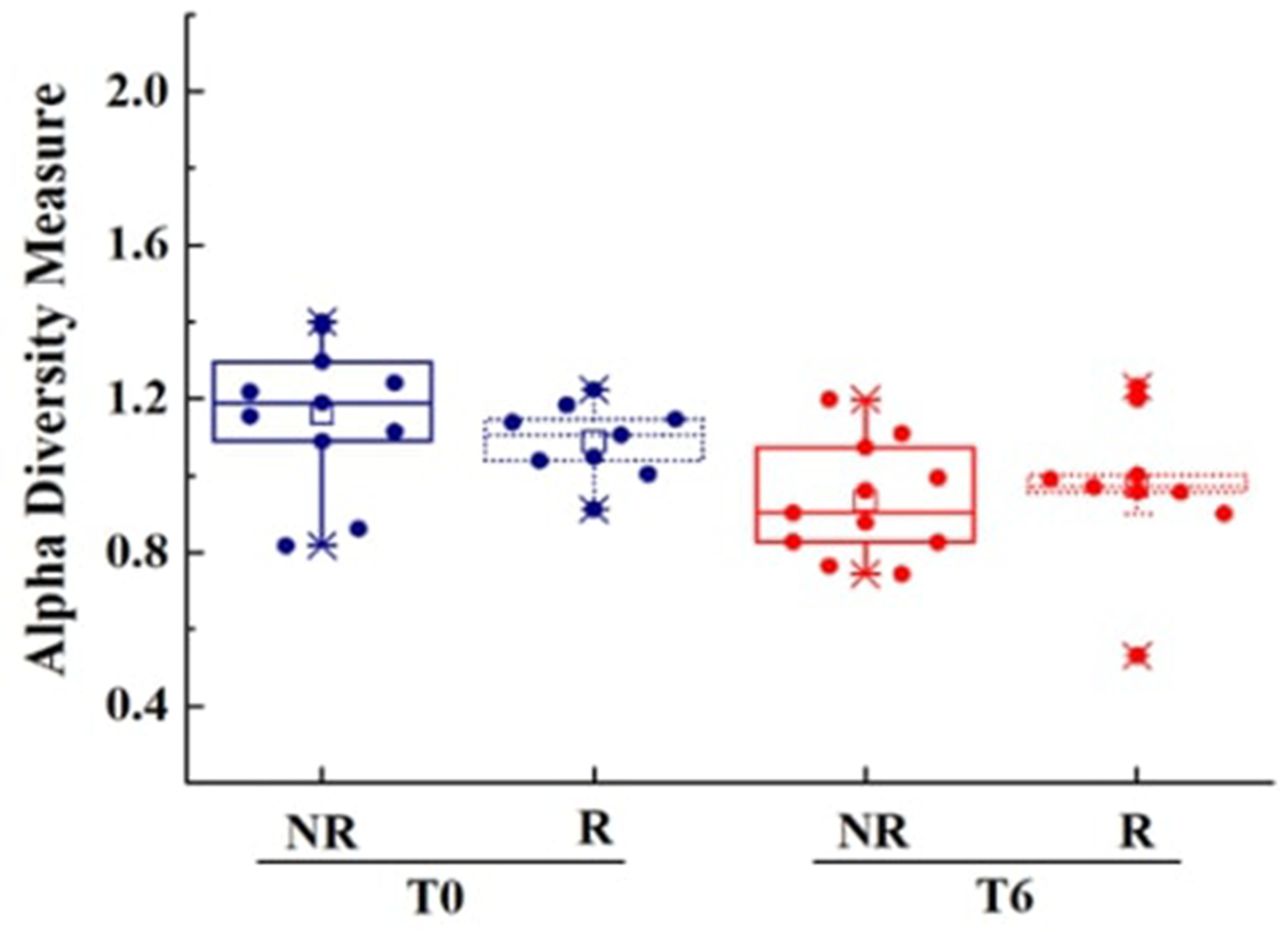
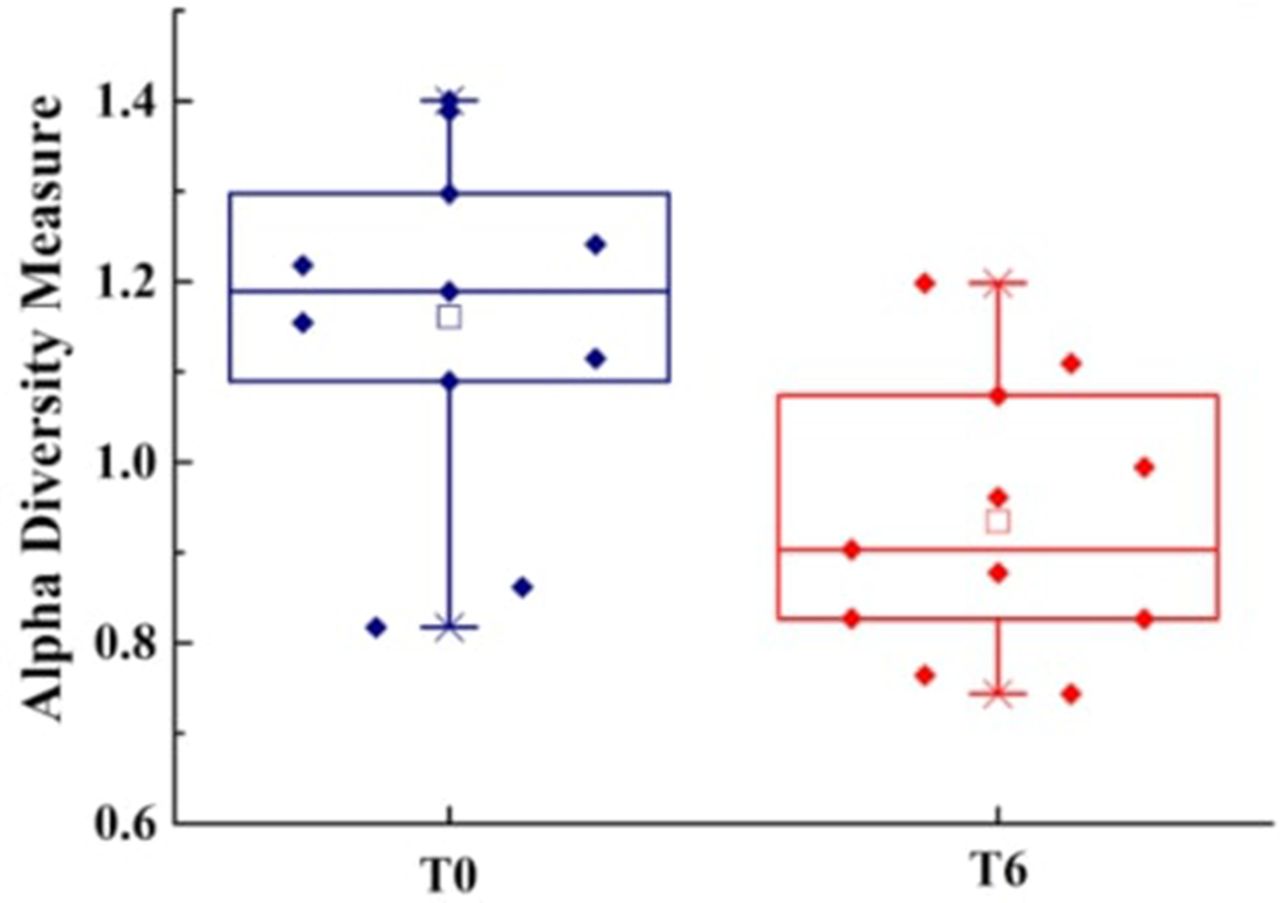
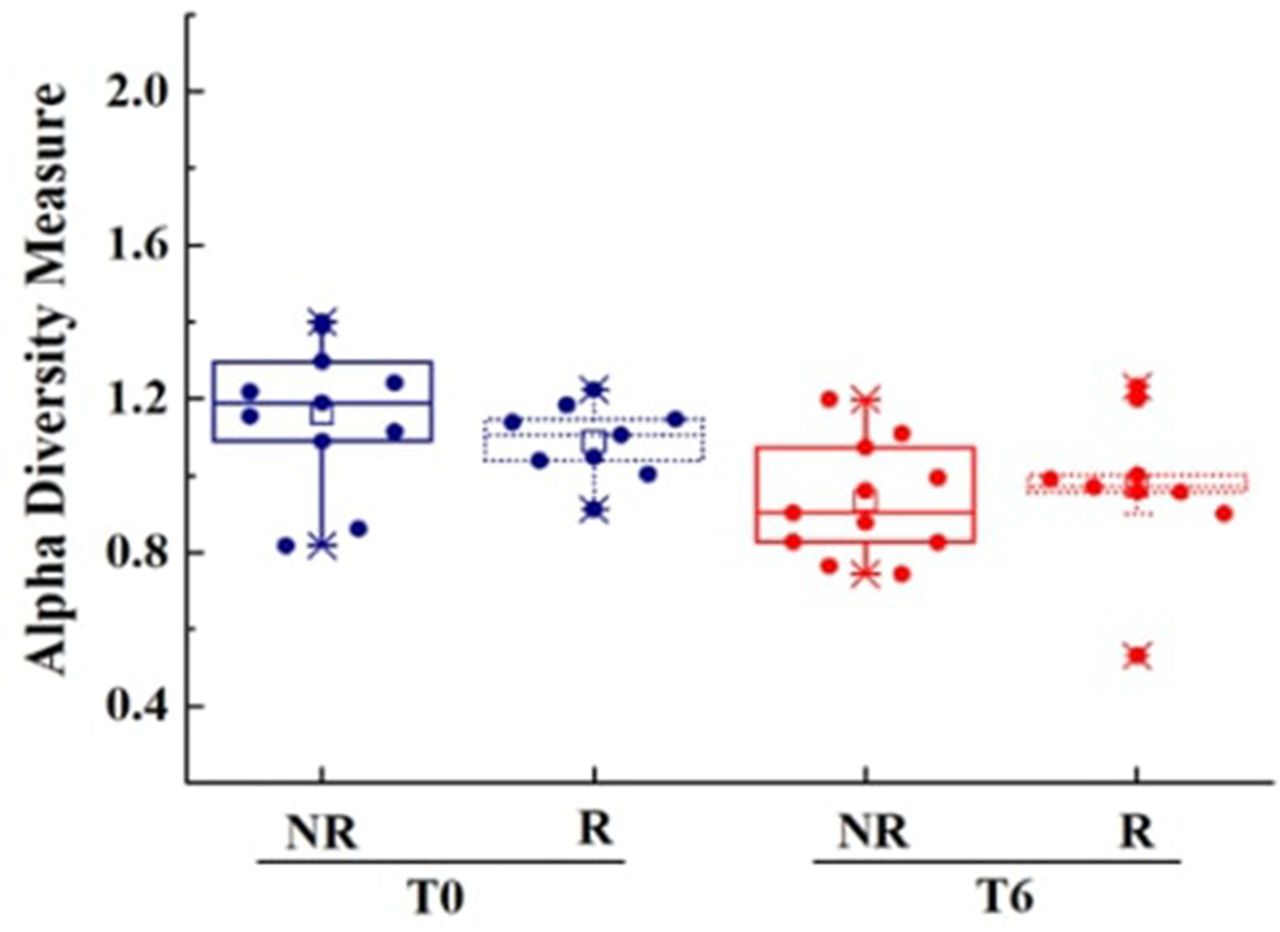
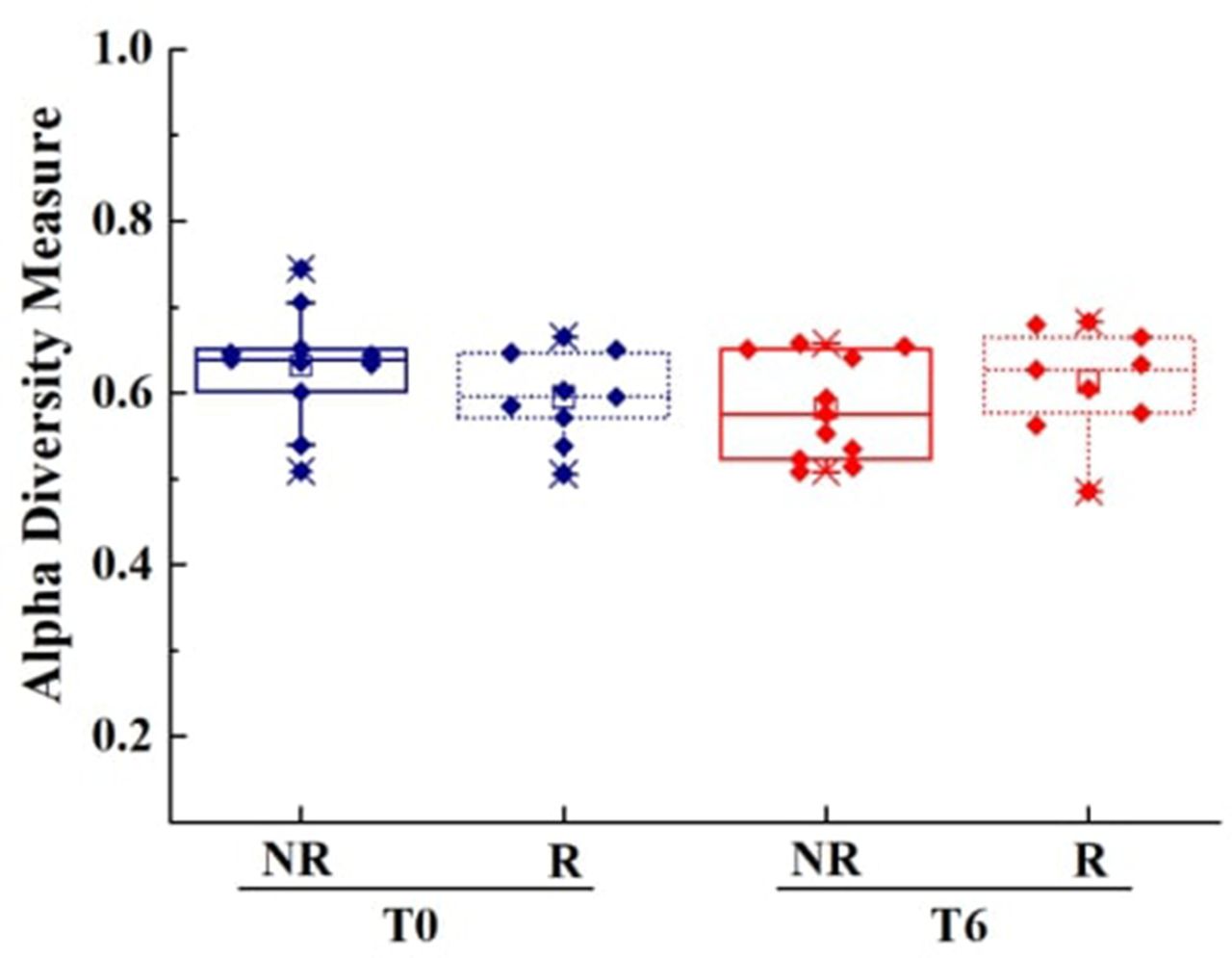
Finally, we compared alpha (intra-sample) and beta (inter-sample) diversity among patients at baseline and after 6 months of therapy (online supplemental files 1–6). We found a decrease of alpha diversity assessed by the Shannon-Weiner index in the class subgroup after therapy (figure 3). Comparing the responders group versus the non-responders one, we noted a meaningful reduction of alpha diversity determined by the Shannon-Wiener index only in the non-responder class group (figure 4) (online supplemental file 7); however, these results have not been confirmed when alpha diversity was assessed through the Simpson index (figure 5) (online supplemental file 8). When beta diversity was measured among population groups we did not identify differences either between T0 and T6 or between responders and non-responders.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Determination of alpha diversity at the class level assessed by the Shannon-Weiner index. Plot of alpha diversity against patients at basal (T0, blue) and after 6 months of treatment (T6, red); a comparison between non-responder patients (NR, line) and responder patients (R, dots) is also shown both at T0 and T6. Alpha diversity was calculated using the Shannon-Wiener Diversity Index (Eq. 2); the index for patients at T0 is significantly different from those at T6 (two-tailed t-test with unequal variance, p value=0.0013).
Determination of the alpha diversity between non-responders at the class level assessed by the Shannon-Weiner index. Plot of the alpha diversity against non-responder patients at basal (T0, blue) and after 6 months of treatment (T6, red). Alpha diversity was calculated using the Shannon-Wiener Diversity Index (Eq. 2); the index for patients at T0 is significantly different from those at T6 (two-tailed t-test with unequal variance, p value=0.0053).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Determination of alpha diversity at the class level assessed by Simpson index. Plot of alpha diversity against patients at the basal (T0, blue) and after 6 months of treatment (T6, red); a comparison between non-responders (NR, line) and responders (R, dots) is also shown both at T0 and T6. Alpha diversity was calculated using the Simpson’s Diversity Index (equation 1); the index for patients at T0 is not significantly different from those at T6 (two-tailed t-test with unequal variance, p value=0.3288).
Discussion
The human gut microbiota is composed of approximately 100 trillion bacteria, belonging to several hundreds of different species.47 More than 90% of all colonic bacteria belongs to four phyla in the Bacteria domain: primarily in Firmicutes and Bacteroidetes phyla, followed by Actinobacteria and Proteobacteria phyla. Other less represented phyla include Verrucomicrobia and Fusobacteria.48 The distribution of these phyla varies along the gastrointestinal tract, depending on the different microenvironments and the nutrient availability.49
A healthy microbiota contributes to a healthy host. Indeed, microbiota not only plays a fundamental role in the metabolism of nutrients and drugs but it also contributes to the development and maintenance of the intestinal mucosal barrier integrity; additionally, it participates in the immune system regulation and defence against pathogens.6 7
The relationship between dysbiosis and several diseases was robustly established; for example, in periodontal disease,50 cancer,51 obesity,52 53 diabetes54 55 and chronic fatigue syndrome.56
Pieces of evidence on dysbiosis both in SpA and in IBD were also found, which would suggest a link between these two inflammatory diseases. For instance, germ-free rats HLA-B27+ not only developed gut inflammation but also joints inflammation after recolonisation.57 While the effect of some drugs on microbiota, such as metphormine, Proton-pump inhibitor (PPI) and antibiotics are well known, poor data are available on TNFi.
Since the efficacy of these drugs on SpA and IBD has been widely demonstrated, a dramatic improvement in inflammatory parameters both in the acute phase index (CRP, ESR) and in faecal calprotectin is not surprising.
The aim of our study was to check microbiota modification after TNFi in a population affected by enteropathic arthritis. While some data are available on IBD or SpA alone, no literature data exist on this cluster of patients. TNFi can have an impact on disease improvements not only by modifying the intestinal permeability but also with a direct action on the microbiota. For instance, animal models of PG-induced arthritis showed an impaired abundance on three of the most representative phyla and TNFi treated animals did not; TNFi was able to restore the relative abundance of such species, including Lactobacillus and Clostridium.30Additionally, a decrease in the major phyla of Firmicutes, in particular Faecalibacterium prausnitzii and Clostridium leptum species in both SpA and IBD,20 as well as an increase of Firmicutes to Gammaproteobacteria has been observed in CD.58 Therefore, we first investigated the microbiota composition before and after treatment at the taxonomic levels (phylum, order, family, genus and species), by comparing the faecal samples before and after 6 months of TNFi (adalimumab or infliximab) therapy. Focusing on microbiota at the phylum level, we observed a reduction of Proteobacteria from 12.6 (3.4–23.3) to 4.6 (2–6.9), which is consistent with literature despite the absence of statistical significance (p=0.09). Similarly, we ascertained the same trend for the Gammaproteobacteria class (Proteobacteria phylum) with a reduction from 10.8 (0–22.8) to 1.8 (0–6, p=0.09); contrarily, we spot an increase in the Clostridia class (Firmicutes phylum), which raised from 34 (18.9–47.2) to 42.2 (34.3–52.1, p=0.08). These results are consistent with the increase of Firmicutes/Proteobacteria ratio in IBD patients and seem to indicate a shift versus eubiosis after TNFi.
In the overall Lachnocpiraceae family, the gut microbiota showed a discordant trend between SpA and IBD, as it increased in the former and reduced in the latter. However, two genera of the Lachnocpiraceae family shared a similar trend between SpA and IBD; indeed, both in SpA and IBD, the Ruminococcus gnavus genus increased and the Roseburia genus decreased.59 From the analysis at the family level, we observed a significant increase of the members of the Lachnospiraceae family, which switched from 17.1 (9.2–21.1) to 26.5 (20–29.1, p=0.04); of particular interest was the Coprococcus genus, which switched from 0 (0–1.6) to 2.8 (0–4, p=0.003). Our data again would suggest an impact of TNFi on gut microbiota (figure 2).
Literatures reports on the microbiotic population trends of SpA and IBD are often conflicting. In some cases, the population trend decreases in SpA and grows in IBD; in other cases, the population trend increases in SpA and decreases in IBD; in still other cases, the population trend in SpA is very similar to that in IBD.
In our study, the correct interpretation of results can be further complicated as, in some cases, samples were taken from patients affected both by SpA and IBD. Although, a typical dysbiosis in our cohort should be more similar to the IBD dysbiosis—which might indicate a greater impact of IBD than SpA on the microbiota of these patients—detected trends in SpA and IBD did not demonstrate a full statistical significance; we also did not identify any known bacterial alteration in IBD.
We discovered a significative decrease of the alpha diversity determined using the Shannon-Weiner index in the class subgroup between T0 and T6, but these findings have not been confirmed by the Simpson index (the best index to use with a small sample size). As to the evaluation of beta diversity, we did not spot differences between patients at T0 and T6 and between responders and non-responders.
Our data are consistent with findings from the Aden and colleagues study, in which two groups of patients affected by IBD or rheumatic diseases were treated with TNFi. They discovered that the treatment restored the microbiota with an increase in the alpha and beta diversity only for IBD patients; no differences were identified between responders and not responders.32
Another study concluded that the response to TNFi was affected by high disease activity and unstable microbiota composition, and patients with reduced biodiversity at baseline were more likely to fail the TNFi treatment. TNFi abolished the differences among patient groups, suggesting that the treatment can restore the microbiota, which happens independently to the clinical response.33 As a consequence of this, we performed further analysis to verify the impact of the inflammatory status on the change of the microbiota and check the relationship between the movement of the microbiota and the course of the disease. The univariate analysis showed that the CRP trend—a parameter of inflammation both for SpA and IBD—is consistent with the Coprococcus trend; this would confirm the hypothesis that the TNFi therapy tends to restore the intestinal eubiosis, by decreasing inflammation. We did not spot differences between responders and not responders, suggesting that TNFi can restore faecal microbiota and independently to clinical response.32
The sample size of our population was small, which heavily affected the power of our statistical analysis.
Our study did not compare the intestinal microbiota of patients with that of healthy people and, therefore, it does not establish the nature of the dysbiosis, which might play a key role in the pathogenesis of SpA. Furthermore, we did not compare groups of patients treated by TNFi or other concomitant treatment with those drugs regularly used by patients as maintenance therapy (such as mesalazine, azathioprine, steroids and antibiotics)60; thus, we cannot strongly affirm that modifications of microbiota are related to TNFi. To partially solve this bias, patients maintained the same therapy before and during the study period; moreover, all patients were treated with infliximab or adalimumab (etanercept was excluded). These drugs in vitro similarly mediate complement-dependent cytotoxicity and antibody-dependent cell-mediated cytotoxicity; they also affect in the same manner the proportion of cells undergoing apoptosis and the level of granulocyte degranulation.61
We analysed microbiota in faecal samples, which were used as a surrogate for the entire gut microflora. Although it is well known that the composition and function of the faecal microflora differ from that of the mucosal microflora48 and it also includes microbiota and virota, the evaluation of stool samples is currently the easiest way to assess intestinal microbiota and it allows the evaluation of the microflora from the entire gut tract.
Our study is based on 16S rDNA sequencing, which allowed us to investigate only bacteria and exclude the virobiota, the mycobiota and eucaryota inhabiting intestinal tract and playing a consistent role in the physiopathology of several diseases.62
We included into the study only patients with a typical Mediterranean diet, but we did not perform any specific evaluation on the diet; for instance, we did not determine the percentages of carbohydrates, fats and proteins intake, which might have affected the results.63
Although enteropathic arthritis is a well-known nosological entity, there are not clinimetric systems to evaluate the progress of this disease; therefore, the trend of both IBD and arthritis have been ascertained separately. Furthermore, literature concerning dysbiosis in these two pathologies often differs, leading to a distortion of our results.
Despite these limits and independently of the achievement of clinical success, our results unequivocally reveal a modification of the microbiota towards eubiosis related to TNFi. Based on this, the microbiota could play a key role in targeted therapies in the future.
Conclusions
Our study is a proof of concept study, which has explored for the first time the modification of microbiota composition towards eubiosis in relationship with the TNFi treatment. Our study would indicate an association of TNFi with the decrease of Proteobacteria and with the increase of Lachnospiraceae and Coprococcus. The study data would support the hypothesis the TNFi therapy, by decreasing inflammation, tends to restore the intestinal eubiosis. Our study is characterised by some limitations, including the small number of patients under analysis and the absence of a control, which prevents from a definitive conclusion; yet, it can be considered a starting point for future examinations on this topic.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. The study dataset is available upon reasonable request and is archived by the corresponding author. The protocol deposited with the Ethics Committee is also available.
Ethics statements
Patient consent for publication
Ethics approval
Comitato Etico Interaziendale of AOU Città Della Salute e della Scienza di Torino (n of approval 0056924).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Dott.Simone Parisi
Presented at Manuscripts previously presented at EULAR 2021 and published as a conference abstract. Ditto MC, Parisi S, Landolfi G, et al. POS0230 IntestinaL Microbiota changes TNF-Inhibitors induced in IBD-related spondyloarthritis. Ann Rheum Dis 2021;80:335.
Contributors MCD and SP contributed in the same way to the realisation of the study and to the writing of the paper. GL contributed to the development of the specific part of statistics on biodiversity and to review of the paper. GPC contributed to the analysis of the samples, CR contributed to the data collection, AZ, GC, CAS contributed to the statistical analysis of the study. RB, AF, DGR, MAstegiano, MAntivalle, PS-P and EF contributed to the review of the study and the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.